Sarah Woods*, a 46-year-old woman with type 2 diabetes mellitus, arrives at the endocrinologist’s office for a routine visit. She complains of fatigue, anxiety, and “a racing heart.” She states she has felt particularly stressed since the recent death of her mother who had Alzheimer’s disease. She denies having had any recent illness.
In additional to diabetes, Ms. Woods’ medical history includes hypercholesterolemia, osteoporosis, and dermatomyositis (an autoimmune disease). Her current medications are:
- atorvastatin 10 mg daily
- baby aspirin 81 mg daily
- hydroxychloroquine sulfate 200 mg daily
- methotrexate 15 mg subcutaneously weekly
- metformin 1000 mg twice a day
- insulin aspart (Novolog) before meals, 1 unit per 15 carbs
- insulin glargine (Lantus) 11 units at bedtime.
Physical assessment reveals a slightly enlarged thyroid with no tenderness. Ms. Woods’ eyes are noticeably swollen, and her skin is warm and moist. No tremor is observed. Her vital signs are
- blood pressure 162/58 mm Hg
- heart rate 120 beats per minute
- respirations 20 per minute
- temperature 99.5 F.
The endocrinologist orders several laboratory tests and schedules Ms. Woods for a 24-hour radioactive iodine uptake test (RAIU) the next day. Results include:
- random blood glucose: 319 mg/dL
- glycosylated hemoglobin (A1C): 6.9%
- thyroid-stimulating hormone (TSH): 0.2 mlU/L
- triiodothyronine (T3): 276ng/dL
- Free thyroxine (T4): 3ng/dL
- RAIU: increased uptake within the thyroid.
Based on Ms. Woods’ signs and symptoms and the results of diagnostic tests, the endocrinologist confirms that she has Graves’ disease, a type of hyperthyroidism. Ms. Woods is informed of her diagnosis and is started on methimazole, an antithyroid medication. She is instructed to monitor for signs of infection because she is also on methotrexate; both methotrexate and methimazole can cause agranulocytosis.
Disorders of the thyroid gland are fairly common and are most prevalent in women, who are 5 to 10 times more likely than men to have thyroid disease. The most common form of hyperthyroidism is Graves’ disease. Patients with Graves’ disease often have other autoimmune disorders such as dermatomyositis and arthritis, as was the case with Ms. Woods. This article discusses hyperthyroidism, including pathophysiology, diagnosis, and management, with the main focus on Graves’ disease.
What goes wrong in hyperthyroidism?
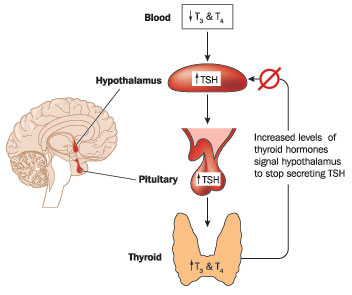
The thyroid gland wraps around the trachea in the anterior portion of the neck. It secretes two “thyroid” hormones (T3 and T4), which regulate body metabolism. Both T3 andT4 are made from tyrosine (an amino acid) and iodine. Most of T3 and T4 secreted into the circulation is bound to specific proteins; only about 1% of it is “free” or able to affect body cells. However, that 1% of active hormone regulates the metabolic rate of nearly all body tissues, enabling cells to function as they should. The thyroid gland is regulated by thyroid stimulating hormone (TSH) from the pituitary gland, which, in turn, is regulated by the hypothalamus. Calcitonin, a hormone that affects blood calcium levels, is also secreted by the thyroid gland. (See Regulation of thyroid gland.)
In Graves’ disease, the body produces immunoglobulins that latch onto the TSH cell receptor sites in the thyroid; this stimulates excess secretion of T3 and T4. The elevated levels of T3 and T4 cause the pituitary gland to decrease its secretion of TSH. Environmental triggers, such as stressful life events and current infections, can cause the onset of Graves’ disease.
Causes of other types of hyperthyroidism, include
- formation of nodules from iodine deficiency (toxic multinodule goiter)
- viral infection of the thyroid gland (thyroiditis)
- excessive pituitary secretion of TSH (secondary hyperthyroidism).
What are signs and symptoms of hyperthyroidism?
When the thyroid gland overproduces thyroid hormones, the body’s energy sources (fats, proteins, and carbohydrates) are metabolized more rapidly. This hypermetabolism leads to increased oxygen consumption and cardiac workload. The beta receptors of the sympathetic nervous system are also stimulated, which adds to the increased demand on the body. This increased demand is manifested by elevated heart rate, temperature, and blood pressure.
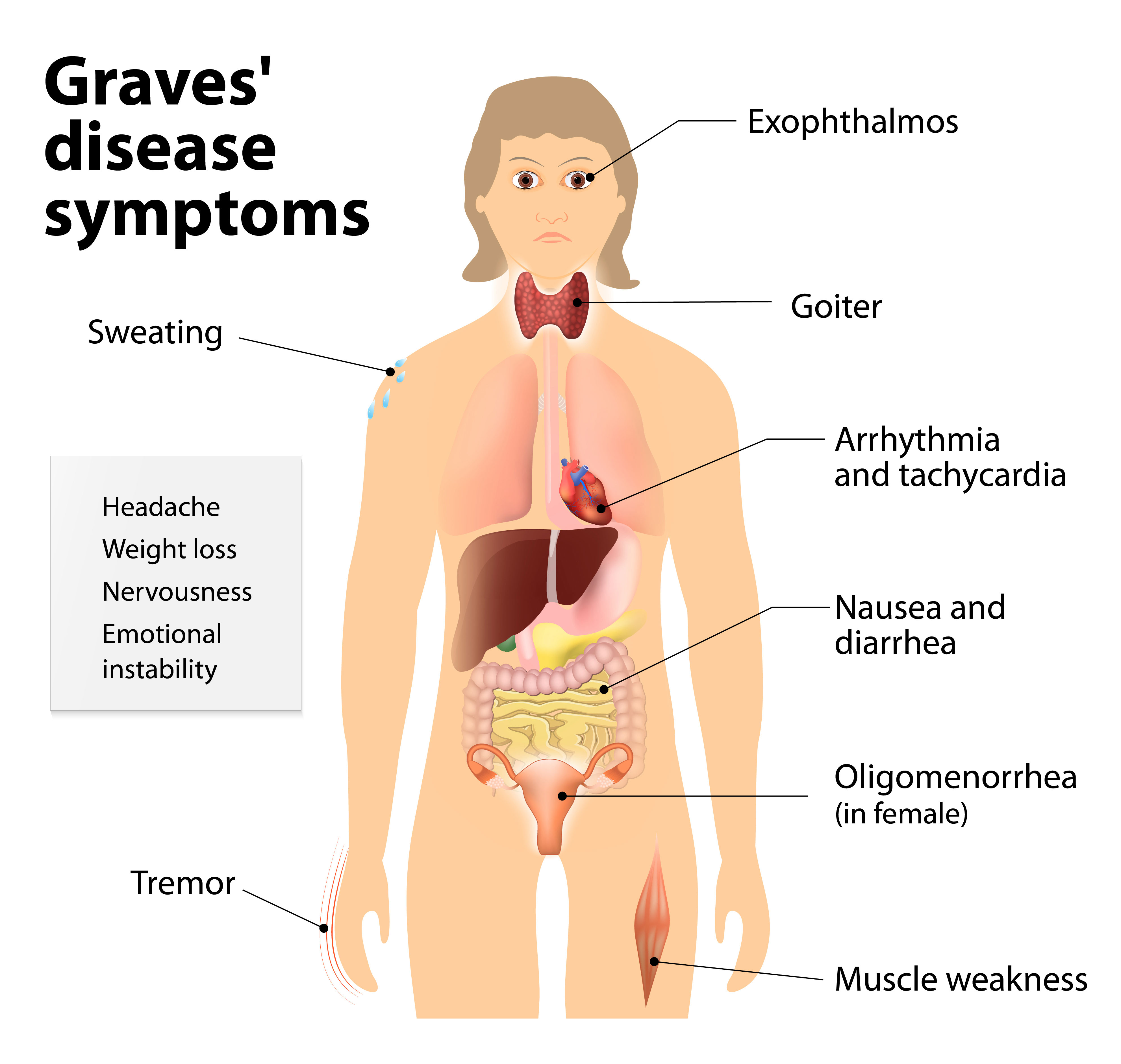
Many patients with Graves’ disease show these signs:
- Goiter. Increased metabolism and vascularity of the thyroid gland can cause it to enlarge and form a goiter.
- Exophthalmos. Protrusion of the eye globes occur because of fat accumulation and inflammation of the orbital eye contents.
- Pretibial myxedema. An increase in the inflammatory process causes swelling and inflammation on the front of the shins.
As you may recall, Ms. Woods had a slightly swollen thyroid and exophthalmos. Other signs and symptoms of Graves’ disease include irritability, anxiety, and sleeplessness. (See Signs and symptoms of Graves’ disease).
What diagnostic tests are used for hyperthyroidism?
In addition to clinical signs and symptoms, simple laboratory tests aid in the diagnosis of hyperthyroidism. Pertinent tests are TSH, T3, T4, and free T4. The patient also may be tested for the presence of thyroid antibodies.
In Graves’ disease the problem is within the thyroid gland (primary hyperthyroidism), so the TSH will be low and the T3, T4, and free T4 levels will be elevated, as was the case with Ms. Woods. Elevation of all three levels indicates the hyperthyroidism is caused by a disorder of the hypothalamus or pituitary gland (secondary hyperthyroidism).
The RAIU is a nuclear imaging test especially helpful for diagnosing hyperthyroidism because it directly measures the ability of the thyroid gland to take up iodine. Iodine is used for T3 and T4 production, so increased uptake of the iodine signifies excess production of T3 and T4. (See chart for a summary of the types of hyperthyroidism.)
One week after her diagnosis, Ms. Woods arrives in the emergency department in acute distress. She says, “I think I’m having a heart attack! My heart is racing and I feel so short of breath!” Her vital signs are: 168/92 mm Hg, heart rate 136 beats per minute, respirations 24 per minute, and temperature 101.9 F.
In response to the nurse’s questions, Ms. Woods explains that she has been ill the last 4 days and has lost 5 pounds. Although she started taking the methimazole, she has not been able to take it regularly because of nausea and vomiting. The nurse recognizes that Ms. Woods may be going into thyroid storm and needs to be admitted to a unit with telemetry monitoring.
Thyroid storm: A grave emergency
Thyroid storm is the worsening of hyperthyroid signs and symptoms. Although it’s a rare complication of hyperthyroidism, it can be fatal. Without prompt intervention, patients like Ms. Woods may develop heart failure and circulatory collapse, and their temperature can rise to dangerous levels.
Precipitating events that put a patient at risk for thyroid storm include trauma, surgery, infection, stress, and nonadherence to a medication regimen. In the case of Ms. Woods, it is likely that the medication had not yet reached a therapeutic level because of her nausea and vomiting. She is also grieving the recent loss of her mother, adding to the stress of being ill.
Essential goals for the patient with hyperthyroidism showing signs of thyroid storm are management of symptoms, restoration of nutritional balance, initiation of a therapeutic regimen, and education for the patient and family.
Management of symptoms
- Place the patient on a cardiac monitor and monitor for dysrhythmias.
- Monitor vital signs with special attention on temperature and heart rate elevations.
- Replace electrolytes and monitor fluid status.
- Administer oxygen to treat dyspnea and (possible) heart failure.
- Administer beta blockers to decrease sympathetic activity symptoms.
- Administer acetaminophen to reduce temperature. Salicylates, such as aspirin, should be avoided because they prevent thyroid hormone from binding to proteins in the blood; this would result in higher levels of active (unbound) thyroid hormone.
- Provide a calm and quiet environment to decrease anxiety and irritability.
- Maintain a cool room and environment. This may include the use of a cooling blanket.
- Provide eye care if the patient has exophthalmos: Administer artificial tears to reduce dryness and corticosteroids to reduce inflammation.
Restoration of nutritional balance
- Collaborate with a registered dietician; because of the hypermetabolic state, caloric intake must be increased to 4000-5000 calories per day.
- Encourage six meals per day. Meals should be high in protein (1-2g/kg of ideal body weight) and carbohydrates to combat the effects of excessive hunger and weight loss.
- Monitor blood glucose levels every 6 hours and administer additional insulin as needed per protocol.
Initiation of a therapeutic regimen
- Administer antithyroid medications, which stop the production and release of excess T3 and T4. Plasmapheresis or dialysis may be needed in emergency states to quickly decrease circulating levels of T3 and T4.
Patient and family education
- Teach patient and family about hyperthyroidism and the need for antithyroid medication.
- Encourage patient to follow up with his or her regular healthcare provider.
- Provide information about on-line resources such as The American Thyroid Association or the National Institutes of Health.
Ms. Woods is placed on a cardiac monitor and oxygen, and an I.V. is started. She is given propranolol to lower her heart rate and blood pressure and acetaminophen to decrease her temperature. A loading dose of methimazole 30 mg is also given. Ms. Woods is stabilized and 3 days later she returns home on oral methimazole (10 mg three times/day).
Long-term treatment options for hyperthyroidism
After the patient with thyroid storm, or acute hyperthyroidism, has been stabilized, it’s important to start on-going treatment. Options include oral antithyroid medications, radioactive iodine (RI), or surgery.
Oral medications
Some patients effectively manage their hyperthyroidism with long-term antithyroid medications. (See Medications for treating hyperthyroidism.) The medications may be tapered as the patient reaches a normal thyroid state. It is essential to educate patients about the need to consistently take the medication and to monitor for any adverse effects.
Radioactive iodine (RI)
A calculated dose of RI is ingested and taken up by the thyroid gland. Over the course of 6 to 8 weeks, some of the over-functioning thyroid tissue is destroyed. Several doses may be needed to obtain the desired effect. Patients undergoing RI treatment need to limit close contact with others for 3 days after each dose. If RI destroys too much thyroid tissue, the patient will need lifelong thyroid replacement medication.
Surgery
A partial or total thyroidectomy may be performed to alleviate the symptoms of hyperthyroidism. This option is usually reserved for patients who do not respond to other treatment modalities or who have a specific area of the thyroid that is overactive. Patients who undergo a total thyroidectomy will need lifelong thyroid hormone replacement.
Ms. Woods returns 2 weeks later to her endocrinologist’s office. She states she feels much better and that she has been able to take her medication. Her vital signs and TSH level are within normal limits. She has joined a grief support group that she plans to attend weekly. The nurse reviews Ms. Woods treatment plan with her.
Challenge of hyperthyroidism
Hyperthyroidism is a disorder that can affect many body systems. If signs and symptoms are not promptly recognized and treated devastating effects may occur. The nurse plays an important role in the assessment, management, and education for this disorder.
Julia Hooley is director of the Center for Study and Testing, and Stephanie Reagan is an associate professor of nursing at Malone University School of Nursing and Health Sciences in Canton, Ohio.
Selected references
American Thyroid Association. www.thyroid.org
Adams M, Urban C. Pharmacology: Connections to Nursing Practice. 3rd ed. Boston, MA: Pearson; 2016.
Ghandour A, Reust C. Hyperthyroidism: a stepwise approach to management. J Fam Pract. 2011;60(7):388-95.
Morton P, Fontaine D. Critical Care Nursing: A Holistic Approach. 10th ed. Philadelphia, PA: Wolters Kluwer | Lippincott, Williams & Wilkins; 2013.
National Institute of Diabetes and Digestive and Kidney Diseases. Graves’ disease. 2015.
Science and Technology in Action. 6th ed. Thyroid cancer. 2013.
Walton, B. The highs and lows of thyroid diseases. Ohio Nurse. 2015; 8(4).
*Name is fictitious.


















{kind=link}
{kind=link}