If you can auscultate the heart sounds of a child and identify his or her condition, you may be the difference between a delayed diagnosis and timely treatment. With the right skills and knowledge, you can assess pediatric patients confidently and provide pertinent information to parents and other clinicians, thus easing fears and promoting better outcomes.
How to listen
If you’re learning to identify normal and abnormal pediatric heart sounds, keep this in mind: Actually auscultating pediatric patients is a better way to learn than listening to recordings. While learning to recognize heart sounds, try the inching technique. Move the bell of the stethoscope in small increments around the various areas of the chest to identify the different heart sounds.
Before examining a child, make sure you’re in a quiet environment where you can listen without distraction from outside noise and identify what’s happening inside the patient’s chest. You’ll perform the examination with the child sitting, standing, and lying. Changing the patient’s positions will allow you to detect murmurs and determine their origins.
Always listen with the bell and the diaphragm of the stethoscope. You’ll hear low frequencies with the bell and high frequencies with the diaphragm. Auscultate using an orderly sequence covering all appropriate areas, including the anterior and posterior chest walls, neck, and axillae. Remember, disease processes and congenital abnormalities displace heart valves, so your area of auscultation will be broader when you assess a child.
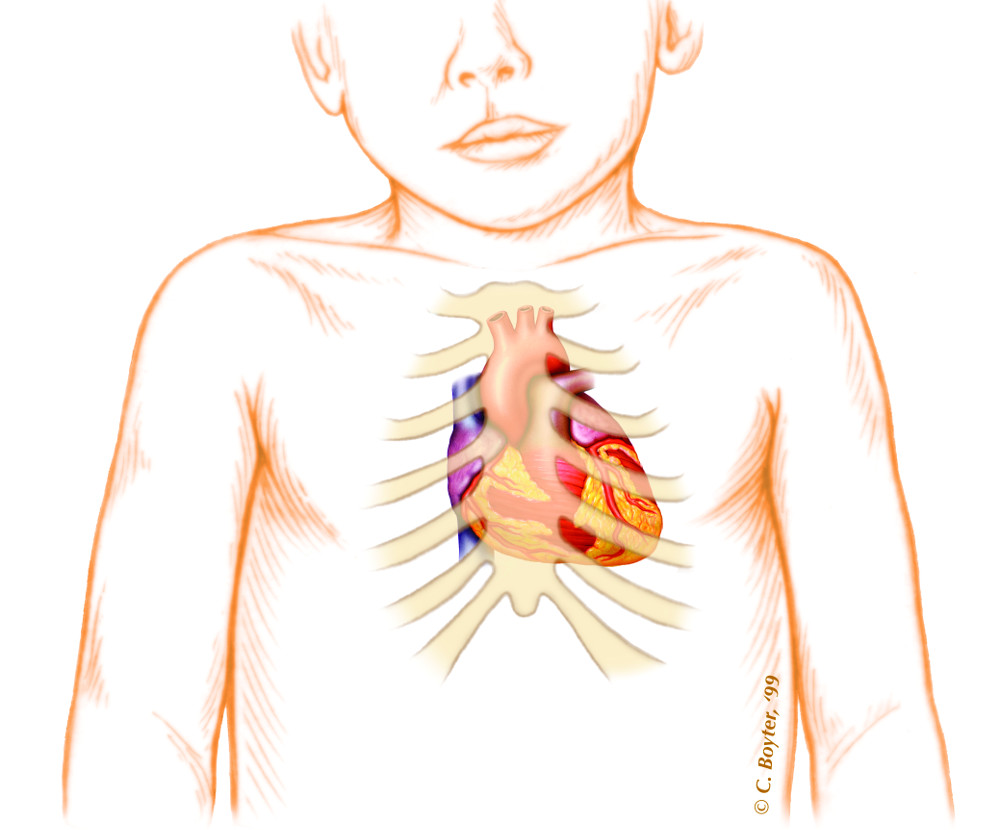
Where to listen
The four regions you’ll auscultate are the tricuspid, pulmonary, mitral and aortic areas.
- The tricuspid area extends from the fourth or fifth intercostal space (ICS) down to the subxiphisternal region and from the left sternal edge to the right of the sternum.
- The pulmonary area includes the second ICS at the left sternal border.
- The mitral area includes the apex of the heart (the fifth ICS at the midclavicular line). This area extends medially to the left sternal edge and laterally to the axillary region.
- The aortic area is centered at the second right ICS and includes the suprasternal area, the neck, and the third left ICS. (See (a href=”” target=”_blank”>Listening posts for pediatric heart sounds.)
When performing a pediatric cardiac assessment, listen for normal heart sounds first, then for systolic heart murmurs, and finally for diastolic murmurs. Determine if the sounds are normal or abnormal. After you learn to identify normal pediatric heart sounds, identifying abnormal heart sounds and murmurs becomes easier. Always be sure to make reference to the respiratory and cardiac cycles when assessing pediatric heart sounds.
Recognizing heart sounds
The first heart sound (S1) represents the normal closing of the mitral and tricuspid valves. The closing of the mitral valve is called M1, and the closing of the tricuspid valve is called T1. Low-pitched and long, S1 occurs at the start of the cardiac cycle and is coordinated with the apical impulse. You’ll hear S1 best at the apex of the heart, the left lower sternal border, or the mid-left sternal border.
The second heart sound (S2) occurs when the aortic and pulmonic valves, also known as the semilunar valves, close. The closing of the aortic valve, called A2, is loud. The closing of the pulmonic valve, called P2, is quieter. Best heard at the upper left sternal border, S2 marks the beginning of diastole. This heart sound has a normal physiologic split caused by the difference in the way the right and left chambers fill. Increased filling of the right chambers during inspiration occurs as blood flows back through the vena cava. Decreased filling of the left chambers results from blood retention in the small vessels. Listen for S2 splitting. No split or a wide split indicates a problem.
The third heart sound (S3) is a normal finding in children. S3 results from the ventricular wall not expanding fully, which causes early diastole. The sound is also related to rapid filling of the ventricle. You’ll hear S3 best by placing a child in the left side-lying position and auscultating the fourth ICS at the left sternal edge. Normally, S3 is loud on inspiration and softer on expiration. A high-pitched S3 in a pediatric patient may indicate heart failure, anemia, left-to-right shunting, or a hyperdynamic heart that’s being stimulated to overwork.
The fourth heart sound (S4) has a low-frequency and occurs in late diastole. This abnormal sound results from decreased ventricular compliance or heart failure. Also called atrial sound, atrial gallop, and presystolic gallop, S4 often is confused with heart murmurs.
Distinguishing murmurs
A heart murmur is a turbulent sound originating in the heart or vascular system. About 50% of children have heart murmurs. The most common is Still’s murmur, an innocent murmur that typically occurs in children between ages 2 and 6. Best heard at the beginning of systole over the pulmonary and mitral areas, Still’s murmur is low-pitched and has a musical quality. Sitting or standing may alter the intensity of this murmur.
Other common, innocent pediatric heart murmurs include pulmonary ejection murmur, pulmonary flow murmur, and cervical venous hum. The pulmonary ejection murmur usually occurs in children ages 8 to 14. You can hear it and the pulmonary flow murmur in early to mid-systole at the upper right sternal border. You’ll hear the pulmonary flow murmur best on the left sternal border at the second and third ICSs; it may radiate to the axillae or back. The most common continuous murmur, the cervical venous hum, occurs most commonly in children between ages 3 and 6. You’ll hear it only when a child sits. If the child turns his head, it disappears.
You may also detect the systolic regurgitant murmur or early or late diastolic murmurs. You’ll hear a systolic regurgitant murmur throughout systole beginning with the S1 at the pulmonary area. This murmur results when blood moves from a heart chamber with high pressure to one with lower pressure.
You’ll hear diastolic murmurs best between the S2 and S1. Early diastolic murmurs occur immediately after S2 and result from inept aortic and pulmonic valves. Mid-diastolic murmurs result from mitral and tricuspid stenosis—rare conditions in children. Late diastolic murmurs, which are also uncommon in children, are caused by blood flow through an abnormal mitral or tricuspid valve.
Adding value
Distinguishing heart sounds in pediatric patients can be challenging. By honing your skills, you can make yourself more valuable to your colleagues and, of course, to pediatric patients and their parents.
Selected references
Evangelista J. Assessment of pediatric heart sounds. Am J Nurse Pract. 2007;11(3):15-18.
Favrat B, Pecoud A, Jaussi A. Teaching cardiac auscultation to trainees in internal medicine and family practice: Does it work? BMC Med Educ. 2004;4:5. www.ncbi.nlm.nih.gov/pubmed/15056393. Accessed March 5, 2009.
Pelech A. The physiology of cardiac auscultation. Pediatr Clin North Am. 2004;51(6):1515-1535.
Patricia Vanderpool is a nurse practitioner in family practice for American Health Network in Edinburgh, Indiana and the owner of Private House Call practice in New Castle, Indiana.

















