
- Many organizations lack role-specific competency-based orientation, leaving nurses to learn on the job.
- Traditionally, nurses learn the charge nurse role over time as they progress from novice to expert, which was sufficient with greater experienced-to-novice nurse ratios.
- This article highlights a hospital that developed a role-based competency program for charge nurses.
Nurses serve as frontline leaders. They must work in various capacities and manage constantly changing priorities. These clinical experts act as go-to resource problem solvers, overseers of patient safety and care quality, policy enforcers, and operational experts responsible for processes including staffing and coordinating nurse–patient assignments. Charge nurses play an integral role in a healthcare organization’s daily workflow and have direct impact on patient outcomes and healthcare financials.
Challenged by a widening transition-to-practice gap and exacerbated by the pandemic, the nursing workforce faces higher-than-average nurse departures. These departures require support for novice nurses in leadership roles. Nurse education leaders from a mid-Atlantic 12-hospital health system reviewed nurse feedback and best practices for improving support for clinical nurses. They identified charge nurse onboarding as an opportunity for improvement. The organization’s Magnet® nurse leaders understood that role validation during the pandemic required an innovative approach, so they developed a pilot, competency-based redesign to charge nurse role training for implementation at the health system’s multi-designated Magnet® hospital in Southeastern Virginia. (See The influence of Magnet.)
Understanding the charge nurse’s role in staffing
Charge Nurse University: Preparing future nurse leaders
The problem
Many organizations lack role-specific competency-based orientation, leaving nurses to learn on the job. According to Delamater and Hall, this gap is especially evident in charge nurse preparation. Pre-pandemic, our integrated health system offered sporadic non-standardized training at some hospitals and inconsistently paired shadowing experiences. As the pandemic progressed, all in-person nonessential classroom training halted. A team of nursing education and Magnet nurse leaders identified healthcare adjusted to new pandemic norms and charge nurse development as priorities.
Traditionally, nurses learn the charge nurse role over time as they progress from novice to expert. The approach proved sufficient during greater experienced-to-novice nurses ratios. However, it’s not sustainable for an expanding novice nurse workforce complicated by pandemic-induced staffing challenges. The need for formal role training became evident.
What we learned
In our review of the literature, we found little research or evidence-based information related to the impact of charge nurse development programs on nursing and patient outcomes. What we did find pointed to the positive impact of formalized charge nurse training.
Andronico and colleagues reported that challenges for novice charge nurses include competing role expectations, staffing levels, lack of leadership support, time constraints, and conflict management. Other reports noted that charge nurses desire training to help them manage conflict, understand unit finances, create a positive work environment, determine their leadership style, and enhance communication. Programs that include these topics result in improved systems thinking and ability to manage units.
According to Spiva and colleagues and Abel and colleagues, implementing a formalized training program and establishing role clarity helps improve staff retention and enhances patient satisfaction. Andronico and colleagues report that standardized training programs empower charge nurses and help them develop a sense of pride in this leadership role. They also noted that a charge nurse development program brings these nurses together, frequently for the first time, and allows participants to have their role and influence formally recognized. Formalized programs also create more positive work environments, which improve nurse satisfaction and lead to increased feelings of confidence and preparedness.
According to Yaghobian and colleagues, the dynamic charge nurse role requires core competencies (clinical, cognitive/perceptual, professional/legal, self-management, staff management, and effective communication) for success. However, limited research exists on developing these competencies into a formalized training plan.
Our understanding of the barriers and enablers to the charge nurse role gave us insight into potential challenges we might encounter when developing and implementing a formalized program. In addition, nurse leaders and professional development practitioners within our organization recognized the need for a rejuvenated program to provide standardized content systemwide and allow for an enhanced supported role experience.
What we did
We conducted our pilot project on a single 24-bed medical-surgical nursing unit, with an oncology sub-specialty. The average experience of a charge nurse on this unit was a little over 1 year. Their ages ranged from 20 to 49 with varied ethnicity. Average daily unit census was 24.3 patients pre-intervention and 24.7 post-intervention. The daily average number of patients with COVID-19 was 3 pre-intervention and 4.16 post-intervention. Charge nurses were in-staffing (caring for their own patient assignment) 75% of the time pre-intervention and 35% post-intervention.
After conducting focus groups with the health system’s charge nurses, we created a role-based competency program to establish standard competence and to provide charge nurses with support and foundational tools to begin or further develop within their role. The intervention included four components: charge nurse competency tool, formalized training, shadowing, and an electronic toolkit.
All of the current unit charge nurses attended formalized training in the fourth quarter of 2021 and were validated with the competency tool. Novice charge nurses participated in the shadowing component; experienced nurses did not.
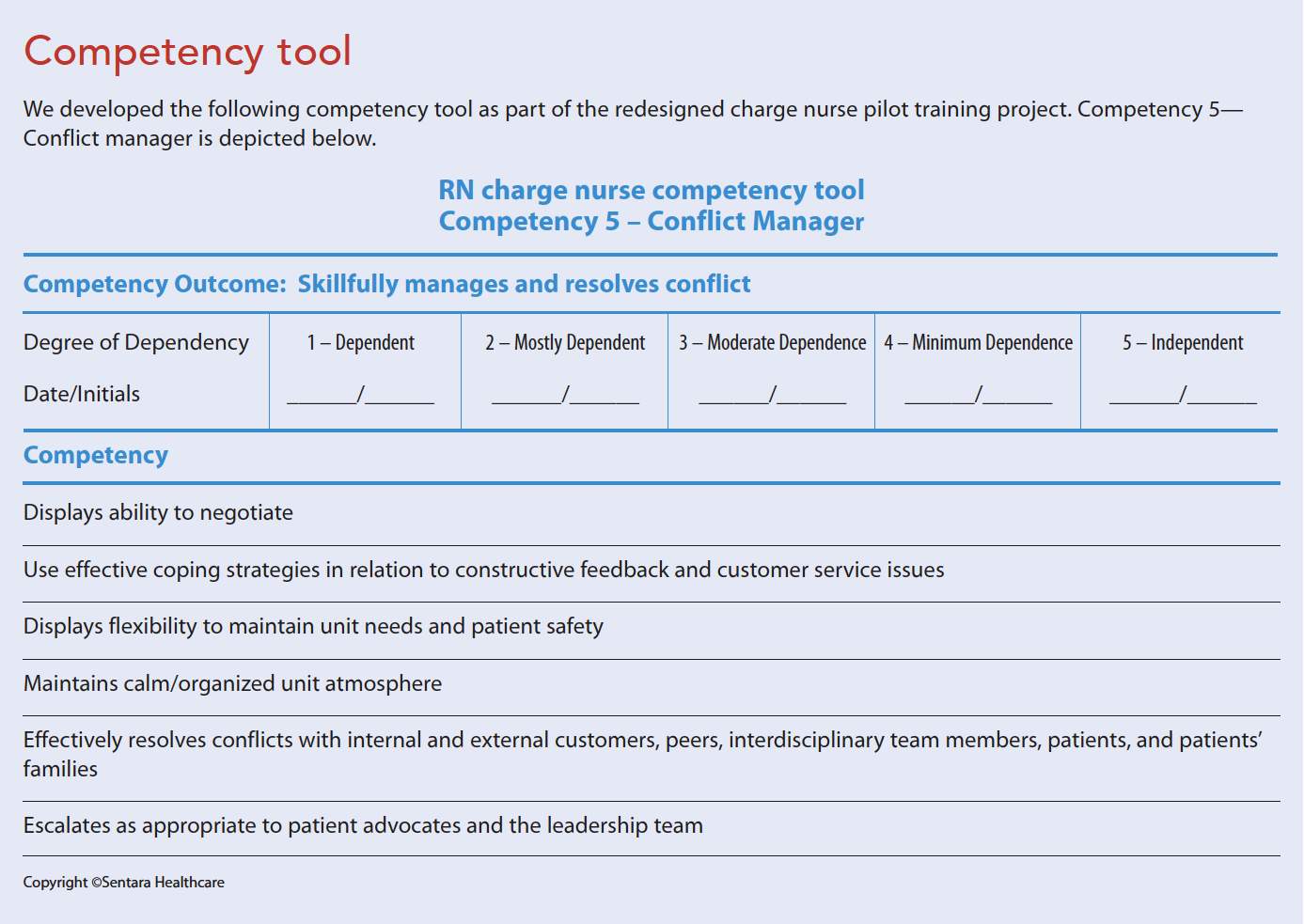
Competency tool
Based on best practices, the competency tool defines and establishes recommended charge nurse selection criteria, which help identify those who possess the characteristics, potential, and willingness to develop for the role. The tool focuses on seven core competencies based on research by Yaghobian and colleagues: proficient/expert clinician, leader, communicator, customer service and experience champion, conflict manager, problem solver, and unit operation expert. The tool can be applied to most areas and includes a customizable section to add patient- and unit-specific items. (See Competency tool.)
Formalized training
The formalized training component (a prerequisite for the third component) aligns with the core competencies, serves as a foundation for nurses new to the role, and provides a refresher for seasoned charge nurses. A live, virtual format supports inclusivity, accomodates social distancing requirements, and ensures access for charge nurses across the multi-state health system. Virtual learning engagement strategies, which instructors incorporate at spaced intervals throughout the 4-hour class, include polling, videos, chat, breakout scenario sessions, interactive worksheets, and gaming.
Shadowing
The 3-day charge nurse shadowing experience allows for introduction and familiarization with unit-specific daily role responsibilities. In focus group feedback, charge nurses identified the need for a shadowing experience prior to starting the role. This protected time provides an opportunity for competency validation by the experienced charge nurse, professional development practitioner, or unit manager.
Electronic toolkit
The electronic toolkit, housed on the health system’s intranet site for easy access, includes resources and tools for practice, including a customizable daily unit checklist. It also provides resources for those who want peer coaching or additional leadership and change management education.
How we assessed outcomes
We measured success of this pilot project using a performance improvement framework, which included observing pre- and post-intervention nurse- and patient-sensitive metrics for performance and quality improvement. We also conducted a survey to elicit participant feedback about the intervention. The intervention occurred in the fourth quarter of 2021, with pre-intervention in the third quarter of 2021 and post-intervention in the first quarter of 2022. We continue to review additional post-intervention data points for potential empirical outcome examples.
Measures
To determine the program’s success, we reviewed unit census, COVID-19 population, charge nurse demographics, patient satisfaction, nursing satisfaction, patient-sensitive metrics, and participant training feedback. We collected post-training learning data via an electronic survey to measure the impact on attendee self-reported confidence and satisfaction with the class. In addition, we used patient-sensitive metrics within the National Database of Nursing Quality Indicators (including patient falls, hospital-acquired pressure injuries [HAPI], catheter-associated urinary tract infection [CAUTI], central line–associated bloodstream infection [CLABSI], methicillin-resistant Staphylococcus aureus [MRSA], Clostridium difficile [C. diff], and workplace assault rates) pre- and post-intervention to determine if strengthening the charge nurse role impacts patient outcomes.
Similarly, because the charge nurse role supports teamwork and provides an additional nursing resource, we reviewed several questions within the health system’s patient experience vendor database. We compared the unit’s Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) scores against the national benchmark. HCAHPS questions, isolated based on course content, included the following: Did nurses treat you with courtesy and respect? Did you get help as soon as you wanted? Did you get help going to the bathroom as soon as you wanted? How do you rate this hospital? In addition, we reviewed 2020 and 2021 nursing satisfaction survey scores; the 2021 scores were collected during the intervention and compared against a vendor-supported pulse survey conducted during the first quarter of 2022. Nine questions were isolated for the 2022 pulse survey based on charge nurse course content.
Results
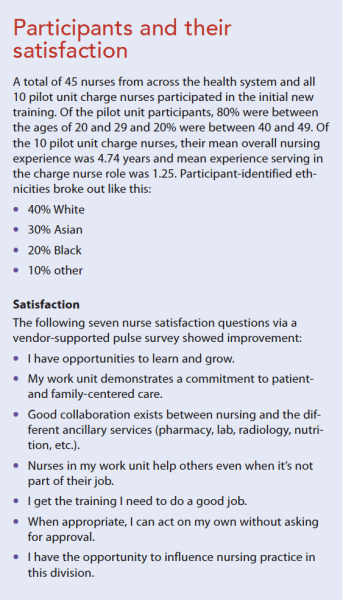
Even with increased bed occupancy and high COVID-19 daily and average unit census, the pilot intervention showed enhanced nursing satisfaction, increased nursing retention, and improved or stable performance in patient-sensitive metrics. A total of 45 nurses from across the healthcare system and all 10 charge nurses from the pilot unit participated in the first class. Of the 45 nurses, 98% reported improved role confidence and satisfaction with the course information, tools, and resources. In a longitudinal survey with a 36% response rate (n=16), charge nurses reported one or more changed behaviors as a result of attending the course. (See Participants and their satisfaction.)
The pilot unit’s patient satisfaction scores for “How do you rate this hospital?” and “Did your nurses treat you with courtesy and respect” improved post-intervention. Responses for “Did your nurses treat you with dignity and respect?” improved from 1.5% above the national benchmark pre-intervention to 5.75% above the benchmark post-intervention. Similarly, pre- and post-intervention responses for “How do you rate this hospital?” improved from 9.5% below the national benchmark to 6.16% above. Scores for patients receiving help and toileting assistance as soon as they wanted did not improve.
Rates of HAPI, CAUTI, CLABSI, MRSA, and C. diff remained at zero pre- and post-intervention. Fall, fall with injury, and nursing assault rates decreased post-intervention. Event tracking showed a trend toward positive compliments and reduced negative safety events. Nursing turnover reduced from 19.2% pre-intervention to 0.0% post-intervention.
Limitations and future implications
The quality improvement design, location, size, and timing limited the generalizability of our conclusions. We conducted the pilot on a single 24-bed inpatient medical-surgical oncology unit with 10 charge nurse program participants. A substantial COVID-19 surge during the post-intervention measurement period and an average daily unit census above the unit’s standard also presented challenges.
Even in light of these limitations, the organization intends to build on the charge nurse program by assessing ongoing professional development needs and conducting annual content reviews for alignment with evidence-based trends. Successful findings during the pilot triggered expansion of the project throughout the healthcare system. Leaders at each division will identify potential charge nurses as certified and targeted for continuing education and professional development goals. They’ll also preplan the need to introduce new charge nurses into the role based on future staffing requirements. Investing in nursing staff professional development leads to improved nurse retention, a common characteristic of Magnet-recognized organizations.
Facilitating improvement
Results from this pilot project facilitated several improved nurse and patient outcomes. A potential exists for units to improve quality measures by focusing on charge nurse development. Implications for all nurse leaders include the adoption of Magnet principles, which guide nursing workforce improvements to compensate for the widening transition-to-practice gap and loss of experienced bedside nurses. Suggested next steps include pilot repetition within additional patient care areas and implementation on a broader level without pandemic-related surges.
Teresa E. Bilyeu is the director of patient care services/Magnet® Program director at Sentara Leigh Hospital in Norfolk, Virginia. Theresa A. Diloy is a nursing professional development specialist at Sentara Healthcare in Chesapeake, Virginia. Jolene J. Dorrell is the system manager of education at Sentara Healthcare. E. Misa Ewing is director of patient care services at Sentara Leigh Hospital. Billie Jo Herwick is a clinical nurse manager at Sentara Leigh Hospital. Jennifer B. Kreiser is vice president /chief nursing officer at Sentara Leigh Hospital. Susan A. Winslow is system director of professional practice & clinical education at Sentara Healthcare.
American Nurse Journal. 2023; 18(1). Doi: 10.51256/ANJ012350
Key words: Magnet, charge nurse, competency-based orientation, COVID-19
References
Abel SE, Hall M, Swartz MJ, Madigan EA. Empowerment of front‐line leaders in an online learning, certificate programme. J Nurs Manag. 2020;28(2):359-67. doi:10.1111/jonm.12933
American Nurses Credentialing Center. 2023 Magnet® Application Manual. Silver Spring, MD: American Nurses Credentialing Center; 2021.
Andronico J, Getting C, Hughes CH, Ciccolini K. Developing and standardizing an orientation for outpatient charge nurses. J Contin Educ Nurs. 2019;50(11):517-21. doi:10.3928/00220124-20191015-08
Bateman JM, King S. Charge nurse leadership training comparison: Effective and timely delivery. Pediatr Nurs. 2020;46(4):189-95.
Cable S, Graham E. “Leading better care”: An evaluation of an accelerated coaching intervention for clinical nursing leadership development. J Nurs Manag. 2018;26(5):605-12. doi:10.1111/jonm.12590
Chervoni-Knapp T. The staffing shortage pandemic. J Radiol Nurs. 2022;41(2):74-5. doi:10.1016/j.jradnu.2022.02.007
Delamater L, Hal, N. Charge nurse development: What does the literature say? Nurs Manag. 2018;49(7):34-40. doi:10.1097/01.numa.0000538914.53159.fc
Spiva L, Davis S, Case-Wirth J, et al. The effectiveness of charge nurse training on leadership style and resiliency. J Nurs Adm. 2020;50(2):95-103. doi:10.1097/NNA.0000000000000848
Yaghobian M, Farhan R, Navipour H, Vanaki Z. Competencies of charge nurses: A systematic review and thematic synthesis. J Pak Med Assoc. 2020;70(7):1225-31. doi:10.5455/JPMA.38686.


















