Program development, implementation, and evaluation.
Takeaways
- Workplace violence is a growing threat in healthcare worldwide and rates of verbal and physical assault correlate with patient contact time, placing nurses in the highest risk category of all healthcare workers.
- All healthcare providers should be equipped with the knowledge to identify agitation and escalating behavior and possess the skills to de-escalate a potentially hostile situation.
- Management of aggressive patient situations (MAPS) curriculum incorporates a specific patient and healthcare perspective using adult learning strategies, differentiating it from other programs intended for a more general audience.
Workplace violence is a serious and growing global threat in healthcare. The Occupational Safety and Health Administration (OSHA) and the Bureau of Labor Statistics (BLS) report that hospitals rank among the most hazardous places to work due to various factors. The BLS notes that workplace violence events, defined as those requiring days off for the injured worker to recuperate, are five times more common in healthcare than in private industries.
Nurses at risk
Rates of verbal and physical assault correlate with patient contact time, which places nurses in the highest risk category of all healthcare workers. In the 2021 American Nurse Journal Nursing Trends and Salary survey of more than 4,500 nurses, over half reported being verbally assaulted by a patient.
A 2016 American Nurses Association health risk appraisal reported that 1 in 4 nurses had been physically assaulted by a patient or a patient’s family. Even more distressing is that these assaults are vastly underreported even at organizations with formal incident-reporting systems. For example, a study by the Emergency Nurses Association Institute for Emergency Nursing Research involving over 7,000 emergency department nurses found that most participants who were victims of workplace violence didn’t file a formal report.
Age and experience aren’t predictors of a nurse’s ability to de-escalate potentially violent situations, and improvement can’t occur without training. All nurses and other healthcare staff must be equipped with the knowledge to identify agitation and escalating behavior and possess the skills to de-escalate a potentially hostile situation.
In response to this rise in violence in healthcare settings, the National Institute for Occupational Safety and Health (NIOSH), OSHA, and The Joint Commission published reports and guidelines recognizing the importance of nurses’ and other healthcare providers’ abilities to prevent workplace violence, and the 117th Congress passed The Workplace Violence Prevention for Health Care and Social Service Workers Act (H.R. 1309). If passed by the Senate, this legislation will require employers to implement comprehensive plans to protect healthcare providers from violence and prohibit retaliation that discourages violent incident reporting.
To address this issue and answer the American Nurses Association (ANA) call to share interventions that help prevent workplace violence, the University of Tennessee Health Science Center College of Nursing (with approval from the institutional review board) partnered with Regional One Health to develop the Management of Aggressive Patient Situations (MAPS) program.
About MAPS
The MAPS program provides nurses and other healthcare staff with the confidence and skills to recognize aggressive patient behavior and de-escalate potentially hostile situations. The specific program objectives include establishing a core group of qualified instructors to provide education and training to hospital nurses and healthcare providers, increasing participants’ confidence in managing aggressive patient situations, and decreasing the number of hospital security calls for aggressive patient situations.
The initial program instructors included six hospital staff with expertise in nursing education, security, and management as well as two psychiatric mental health experts from the college of nursing. All instructors completed the 3-day MOAB® International Management of Aggressive Behavior instructor certification course, which focuses on preventing and diffusing aggressive behavior, managing stages of conflict, addressing physical confrontation, and controlling and restraining aggressive individuals.
MOAB offers instructors who complete the certification curriculum a 1-day course to train additional staff in their place of employment. The 1-day course provides strong basic principles in managing aggressive situations, but it focuses on a general audience and isn’t healthcare-centered. Our core group of instructors created the MAPS program to incorporate the fundamentals of managing aggressive behavior from a patient and healthcare perspective.
Curriculum development
Recommendations from NIOSH and The Joint Commission provided the foundation for MAPS program content development, with a strong emphasis on basic mental health guidelines for communication and management of patient anxiety. We also incorporated various learning strategies suitable for adult learners, including active learning approaches.
We developed three videos—each depicting an example of an agitated patient in one of the three stages of conflict (anxiety, verbal aggression and confrontation, and physical aggression)—and illustrated the use of appropriate de-escalation strategies by healthcare providers. The three videos used examples of real-life hospital scenarios involving agitated patients to develop simulation videos. Psychiatric mental health experts from the college of nursing developed the interventions depicted in the videos, using actors trained to portray patients to provide realism. We filmed the videos in a simulated state-of-the-art healthcare center with an acute-care setting. We then created debriefing questions for discussion after viewing each video. (See Debriefing questions.)
Debriefing questions

After viewing a workplace violence simulation video, participants were asked the following questions:
- If you could describe this experience in one word, what would it be?
- How did this experience make you feel?
- How would you describe this patient’s experience?
- How would your new knowledge help you during this experience?
- Would you have done anything differently to prevent this patient’s behavior from escalating?
Before hospital-wide implementation of the MAPS program, the instructors conducted a pilot teaching session with healthcare leaders from the hospital and faculty from the college of nursing. After attending the session, they provided verbal feedback and written evaluations based on the level of achievement of the learning objectives. In response, the instructors made minor changes to the content. (See Learning objectives.)
Learning objectives
After completing the Management of Aggressive Patient Situations program, participants should be able to do the following:
- Gain awareness of the current state of healthcare violence in the United States.
- Recognize how cultural awareness influences the clinician/patient relationship.
- Recognize the role of self-awareness and self-reflection in managing aggressive patients.
- Identify cultural norms in response to anxiety.
- Use self-reflection to understand factors that contribute to feeling threatened.
- Differentiate between verbal and nonverbal communication.
- Identify common body languages used to communicate.
- Gain proficiency in the use of therapeutic communication strategies.
- Gain proficiency in the use of strategies to reduce emotional confrontation.
- Recognize the three stages of conflict with an emphasis on patients and their families.
- Implement strategies for diffusing aggressive behavior based on the identified stage of conflict.
Implementation
Starting in October 2017, the hospital began offering MAPS about every 2 weeks, with each session accommodating 20 to 30 nurses and other healthcare providers. Two certified instructors taught each 4-hour training session, rotating throughout the implementation period. From October 1, 2017, to June 30, 2019, 311 nurses and healthcare staff completed the program.
Evaluation
With permission from the author, we used Thackery’s Confidence in Coping with Patient Aggression instrument to measure participant confidence pre- and post-MAPS training. Many researchers use this instrument for its high degree of reliability and validity. The instrument uses a Likert scale with 10 items scored from 1 to 11; lower scores represent less confidence and higher scores, greater confidence.
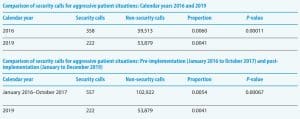
To measure the results of our goal to reduce the number of hospital security calls for aggressive patient situations, the security department provided the total number of aggressive patient security calls for calendar years 2016 through 2019, and our team collected emergency department (ED) data from admission records. To account for monthly and seasonal variations in ED admissions, we compared the yearly proportion of aggressive patient security calls before MAPS training and after.
Outcomes
Of the 311 who participated in the training, 164 completed all the questions on the pre- and post-training instrument. Of those, 133 (81%) were women, 27 (16.5%) were men, and 4 (2.5%) didn’t identify; 103 (63%) were registered nurses, and 61 (37%) were other healthcare staff, including patient care assistants, emergency medical technicians, medical care technicians, and licensed practical nurses. We used the Wilcoxon signed-rank test to compare Confidence in Coping with Patient Aggression scores before and after training and the Wilcoxon sum-rank test to compare changes between genders and registered nurses vs. other healthcare staff. We used the Chi-squared test to compare the proportions of aggressive patient security calls before and after training.
All participants’ confidence in managing aggressive patient situations increased. The findings showed statistically significant improvement for all 10 questions and for the average score for all questions (P<0.001). We found no significant difference when comparing registered nurses and other healthcare staff (P>0.2). (See Increased confidence.)
Increased confidence
After participating in the Management of Aggressive Patient Situations program, nurses and other healthcare staff demonstrated improved confidence in managing potentially violent situations with patients and families.
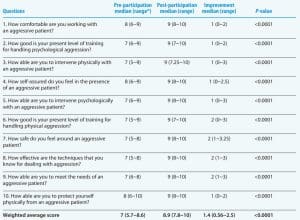
*The interquartile range contains the second and third quartiles, or the middle half of the data set.
The proportion of patient security calls from January to December 2016 compared to 2019 decreased significantly (P=0.000011). We observed a similar decrease in aggressive patient security calls when we compared calls from January 2016 to October 2017 (21 months before MAPS training) with calls for 2019 (P=0.00067).
Reduced calls
After the Management of Aggressive Patient Situations program, calls to security about aggressive patient situations decreased.
Looking ahead
We continue to track aggressive patient security calls, but many variables influence this outcome, including the steady rise in violence across the country (which may contribute to increased security calls) and the COVID-19 pandemic (which has resulted in lower rates of ED visits).
Although recent publications using other types of training resources have demonstrated an increase in confidence in managing aggressive patient behavior after training, no recent publications have demonstrated a clinical outcome such as a decrease in security calls. The healthcare community has yet to recognize universally accepted methods for reducing risk and managing aggressive patient behavior, which requires more research to evaluate various training methods. The MAPS program incorporates a patient and healthcare perspective using adult learning strategies, differentiating it from leading programs intended for a general audience. The simulation videos, based on real-life hospital scenarios and developed by psychiatric mental health nursing faculty and healthcare providers, portray patients in various stages of conflict and illustrate the use of appropriate de-escalation strategies.
Because incidents of serious workplace violence are considerably more common in healthcare than in private industries, programs implemented in healthcare organizations should be designed specifically for their unique needs. We’ve incorporated MAPS training into hospital orientations and our bachelor of science in nursing and doctor of nursing practice curriculum, and we recommend that all staff complete a MAPS refresher course every 2 years.
We recently developed the MAPS Train the Trainer program and are currently in the implementation and evaluation phase. This 2-day program certifies healthcare providers to teach MAPS to employees within their organization. All certified trainers receive a MAPS teaching packet, which includes a PowerPoint presentation, handouts, learning activities, simulation videos, and a teaching guide.
Call to action
Nurses across the United States are aligning in support of actions that prevent workplace violence. The ANA convened a professional issues panel to develop policy and identify strategies to address barriers to nurses and other healthcare workers who report violence and abuse and to strengthen zero-tolerance policies. A Nurse’s Call to Action and other ANA resources are available here.
Sara W. Day is professor and assistant dean at the Center for Community and Global Partnerships at The University of Tennessee Health Science Center College of Nursing in Memphis. Jacqueline Sharp is an assistant professor and PMH concentration coordinator for advanced nursing practice and doctoral education at The University of Tennessee Health Science Center College of Nursing. Gabrielle L. Jackson is a psychiatric mental health nurse practitioner at Alma Wellness Associates in Memphis, Tennessee. Randall L. Johnson is an associate professor and BSN program director at The University of Tennessee Health Science Center College of Nursing. Kimberly A. Smith is a professional development specialist in behavioral health at Regional One Health in Memphis, Tennessee. Xueyuan Cao is an assistant professor at The University of Tennessee Health Science Center College of Nursing. Wendy Likes is dean and professor and Ruth Neil Murry Endowed Chair at The University of Tennessee Health Science Center College of Nursing.
This program was funded by a grant from Tennessee Hospital Association, Promise for Nursing.
References
ANA Enterprise. Healthy Nurse Healthy Nation: Year four highlights 2020-2021. Am Nurse J. 2021;16(10):29-39.
de la Fuente M, Schoenfisch A, Wadsworth B, Foresman-Capuzzi J. Impact of behavior management training on nurses’ confidence in managing patient aggression. J Nurs Adm. 2019;49(2):73-8. doi:10.1097/NNA.0000000000000713
Emergency Nurses Association. Emergency department violence surveillance study. November 2011.
Ferrara KL, Davis-Ajami ML, Warren JI, Murphy LS. De-escalation training to medical-surgical nurses in the acute care setting. Issues Ment Health Nurs. 2017;38(9):742-9. doi:10.1080/01612840.2017.1335363
Georgia Nursing. ANA’s new health risk appraisal evaluates nurses’ health, wellness, safety. 2014;74(1).
Hartley D, Ridenour M, Craine J, Morrill A. Workplace violence prevention for nurses on-line course: Program development. Work. 2015;51(1):79-89. doi:10.3233/WOR-141891
H.R. 1309 (116th): Workplace Violence Prevention for Health Care and Social Service Workers Act.
Nau J, Dassen T, Needham I, Halfens R. Sensitivity, specificity and predictive value of Confidence in Managing Patient Aggression Scale on de-escalating behaviour. J Clin Nurs. 2011;20(17-18):2584-6. doi:10.1111/j.1365-2702.2010.03597.x
Occupational Safety and Health Administration. Workplace violence in healthcare: Understanding the challenge. December 2015.
Phillips JP. Workplace violence against health care workers in the United States. N Engl J Med. 2016;374(17):1661-9. doi:10.1056/NEJMra1501998
Senior R. 2021 nursing trends and salary survey results. Am Nurse J. 2021;16(11):15-20.
Story AR, Harris R, Scott SD, Vogelsmeier A. An evaluation of nurses’ perception and confidence after implementing a workplace aggression and violence prevention training program. J Nurs Adm. 2020;50(4):209-15. doi:10.1097/NNA.0000000000000870
Thackrey M. Clinician confidence in coping with patient aggression: Assessment and enhancement. Prof Psychol Res Pract. 1987;18(1):57-60. doi:10.1037/0735-7028.18.1.57
U.S. Bureau of Labor Statistics. Fact sheet: Workplace violence in healthcare, 2018. April 2020.