
Effective management requires patient advocacy.
Pain in all stages of care—from acute to chronic—can result in debilitating and distressing effects that leave patients feeling as though they have no control. To advocate on behalf of patients, nurses must understand the barriers to pain control, the types of prescribed opioids and their use in palliative and end-of-life care. When patients can’t advocate for themselves, nurses hold the best position to provide that support.
Barriers to adequate pain control
Barriers to adequate pain control include lack of healthcare provider and nurse education, provider bias, regulatory concerns, inadequate assessment, and trepidation about the side effects patients may experience, especially respiratory depression. Compounding these factors, some providers and nurses lack understanding of the difference between opioid use disorder and tolerance as well as between acute and chronic pain management strategies. In addition, patients and families may have misconceptions about pain, unrealistic expectations for its control, and concern about cost.
Substance use disorder, a valid concern, requires that healthcare providers distinguish between manipulative behavior driven by addiction and the physiologic need for increased amounts of medication due to tolerance. Frequently, people with substance use disorder require a higher starting dose of pain medication to achieve appropriate pain control.
Common opioids prescribed for palliative care
Opioids come in different forms and can be administered via various routes. This article focuses on I.V. administration. In the acute setting, providers frequently request a palliative care consult to manage severe pain. The most commonly prescribed opioids include I.V. morphine sulfate, hydromorphone, fentanyl, buprenorphine, and methadone. (See Patient control.)
Patient control
Patients with continuous pain require continuous medication, not only upon request. If using a patient-controlled analgesia pump, the basal rate equals the amount of medication administered hourly, making it the continuous control. Increased pain may be incidental with a known cause (such as movement) or idiopathic (no cause can be identified), so a short-acting bolus dose allows the patient to self-administer medication for optimal control. For patients unable to self-administer a bolus, the nurse can administer an ordered clinician dose.
Morphine
Typically, I.V. opioid pain control in the hospital begins with morphine because of its short half-life (approximate amount of time it takes the body to clear half of the drug), which simplifies titration in response to the patient’s pain. For example, if the patient becomes too sedated, the dose can be titrated down and the body will metabolize it quickly. Morphine serves as the benchmark for determining the most appropriate dose of the new form or agent when switching to another form of morphine or changing to another opioid (opioid rotation). Although I.V. morphine may be appropriate for the hospital setting, conversion to an alternate form or agent will be necessary before the patient is discharged home. Patients with continuous pain may go home with an ambulatory infusion pump or transition to an oral form.
Not all pain responds to morphine and some patients may experience adverse side effects, such as nausea or pruritus (itching), that affect quality of life. In those situations, the provider will rotate opioids. Experts have proposed theories about why one agent may provide relief while another doesn’t, but no clear understanding exists.
Hydromorphone
In palliative care, hydromorphone frequently is the agent of choice after morphine. Nurses should be aware of the differences in potency and dosing. Hydromorphone is approximately seven times more potent than morphine (1 mg of hydromorphone equals approximately 7 mg of morphine [exact dose conversions vary]), so less hydromorphone is required to control pain. Improper dose conversions when switching from one opioid to another increases the risk for adverse effects.
Fentanyl
Fentanyl may be prescribed as an alternative if morphine or hydromorphone aren’t effective or if the patient can’t tolerate these drugs. Fentanyl can be administered intravenously, sublingually, or via a transdermal patch. Fentanyl has a higher potency than morphine with dosage forms in micrograms, not milligrams. For example, in some conversion tables, 25 mcg of fentanyl is equal to 1 mg of morphine. Nurses should know the conversion tables used in their facility. After establishing the I.V. fentanyl dose, the provider may transition the patient to transdermal administration.
The transdermal patch provides effective continuous pain control. The dose noted on the patch label equals the dose the patient will receive each hour. Significant clinical factors play a role when considering transdermal administration for a patient. For example, the patient must have adequate subcutaneous fat to absorb the drug, which means this route of administration wouldn’t be effective for a patient who’s cachectic. In addition, because the transdermal medication may take up to 17 hours to reach a steady state, the patient may require a short-acting I.V. opioid for effective pain management. Because transdermal dosages can’t be titrated, the patch is not appropriate for treating acute pain.
To maintain consistent transdermal absorption, avoid placing heating devices over the patch and remember that increases in body temperature can increase absorption. Monitor patients for mental status changes, especially those with a fever. Patches should be changed every 3 days. To avoid overdose, remove the current patch before placing the new one. To improve absorption, place each new patch in a different area. Even after removal, transdermal patches still contain medication and can pose a danger to others. Follow your organization’s disposal guidelines to keep healthcare workers and patients safe.
Buprenorphine
Buprenorphine, not used as commonly as other opioids and requiring careful management, does have a place in pain management. Most opioids allow for gradual increases to compensate for tolerance without limit. In other words, no maximum dose exists and most opioids can continue to be increased to the point of pain control. However, switching from any other opioid to buprenorphine may displace the current opioid from the pain receptor, leading to withdrawal.
In addition to pain management, benefits of buprenorphine include reduced risk of respiratory suppression and physical dependence compared to other opioids. Some buccal and sublingual formulations contain naloxone and are used to help patients recover from opioid use disorder.
Methadone
Most providers won’t rotate first to methadone for chronic pain control because it takes 5 to 7 days to build up in the bloodstream. Although oral methadone is inexpensive, the I.V. form can be cost prohibitive. Estimates vary, but methadone has a half-life of about 59 hours. If clinicians inexperienced with methadone switch the patient to a short-acting opioid, this can lead to the stacking of the respiratory depressive effect of the short-acting opioid on top of the long half-life of methadone. This can cause severe, sometimes life-threatening, respiratory distress. A short-acting opioid can be used for breakthrough pain control, but providers should use caution. Remember that methadone prescribed to treat substance use disorder doesn’t double as pain treatment.
Opioid adverse effects
The most common opioid adverse effects (nausea and pruritis) typically resolve within days. Patient comfort in palliative care includes managing side effects, but if the patient has reliable pain relief, the opioid shouldn’t be changed. Instead, control the side effect. If the side effect can’t be controlled, then the provider should rotate to another opioid. (See Managing common adverse effects.)
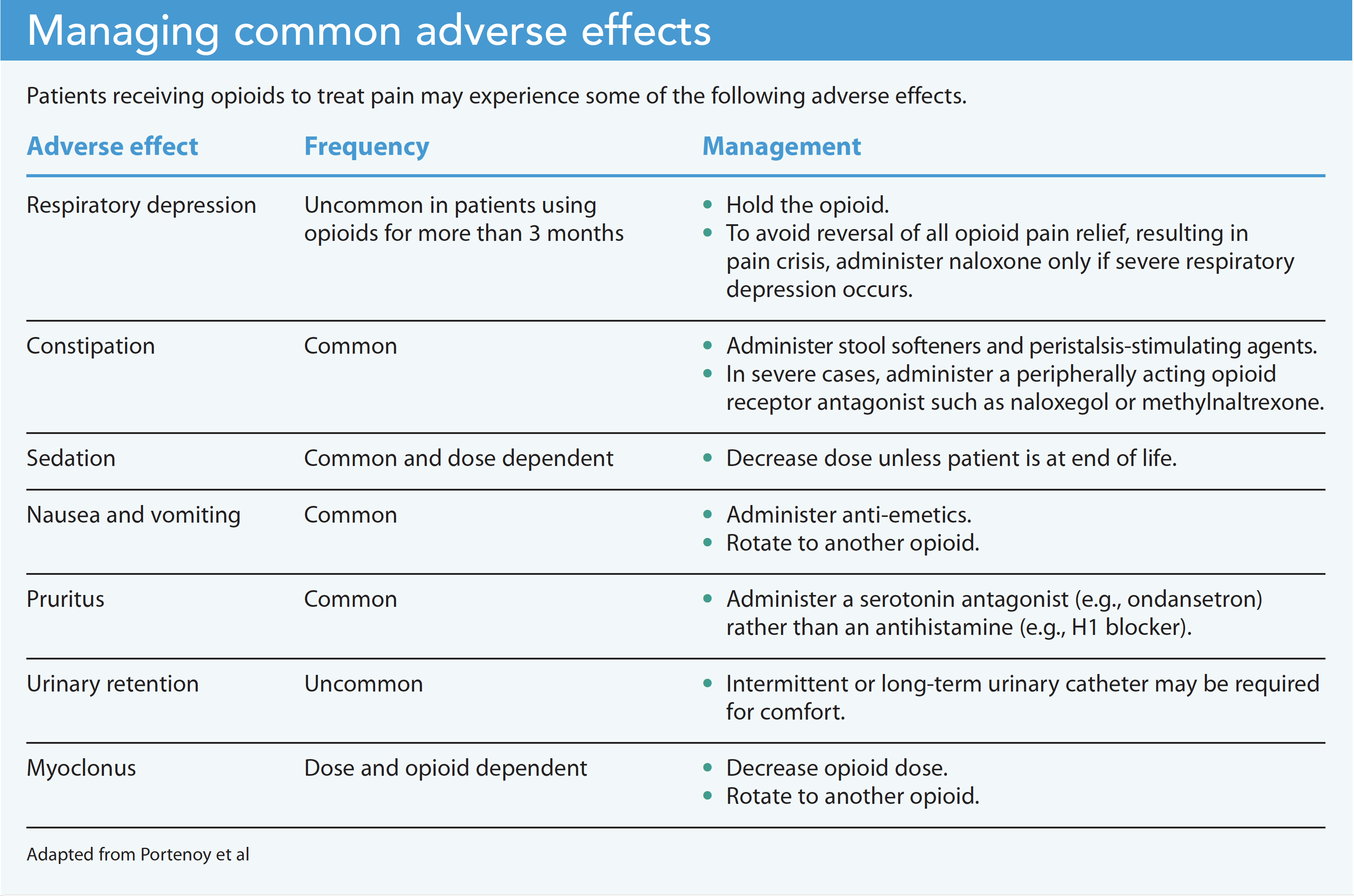
Constipation is an unavoidable opioid side effect, especially with chronic use. Although the severity of some side effects may decrease over time or a patient may develop a tolerance, patients do not develop a tolerance to constipation, which can lead to obstipation and, in severe cases, bowel obstruction. The opioid’s affinity for bowel receptors slows peristalsis, mucus production, and anal sphincter contraction regardless of how long the patient receives the medication. Constipation severity is patient-specific. Even in the absence of constipation, all patients receiving opioids should have a bowel regimen ordered, including stool softeners and agents that promote peristalsis. Be alert for other non-opioid medications and disease states that can increase the risk for constipation.
Pain management at end of life
Nurses should have familiarity with several concepts (including tolerance and intent) when managing patients in the process of dying.
Tolerance
Some nurses inexperienced in caring for dying patients may feel uncomfortable administering high doses of pain medication. Remember the concept of tolerance and that patients may require increases in medication to achieve an optimal level of pain control. Methods of I.V. administration may differ in these patients. For example, patient-controlled analgesia (PCA) may be appropriate in palliative settings, but a patient moving closer to death may become more somnolent and usually can’t push the bolus button on the PCA pump. In these situations, the provider will set a basal rate with intermittent clinician dosing at set intervals. In addition to higher doses of opioids, various routes of administration may be used, including subcutaneous, oral, and rectal. (See Administration routes.)
Administration routes
Treating pain at end of life may require using various medication administration routes.
Oral route
The oral route is preferred if the patient can swallow and absorb the medication. Hospice and long-term care facilities frequently use the oral route of administration. However, most hospitalized patients at
the end of life can’t take oral pain medication. A full discussion of oral pain medication is beyond the scope of this article, but remember that maximizing pain control requires both long- and short-acting opioids.
Rectal route
The rectal route of medication administration isn’t preferred because of variable absorption, which presents challenges when making adjustments for adequate pain control. This method is more commonly used to treat patients in home hospice and those in nursing homes.
Subcutaneous route
For patients at the end of life who can’t take oral pain medications and have limited I.V. access, providers prefer the subcutaneous route. Benefits include ease of administration and adequate pain control. However, if administered too quickly, subcutaneous infusion can lead to a large pocket of fluid in the subcutaneous space, which may affect the rate of absorption and hinder patients from receiving adequate continuous pain control. Follow the manufacturer’s guidelines for subcutaneous administration of opioid medications. Due to rate limitations, medications may need to be concentrated by the pharmacy, so note the ordered route. Administering a concentrated subcutaneous medication by I.V. creates a safety hazard because it will be absorbed too quickly.
Although goals of care are patient-specific, maximizing comfort is common among all patients at end of life. As patients transition toward death, consider discontinuing vital sign parameters. Respiratory and blood pressure rates that previously would have required decreased dosing of pain medication no longer apply. Most patients can’t speak at this point, so use established assessment skills and monitor for nonverbal cues of discomfort, such a facial grimacing, vocalization, or restlessness. Use evidence-based tools (such as the Pain Assessment in Advanced Dementia scale and Critical Care Pain Observation Tool) to support your assessment.
Intent
As a patient’s vital signs and wakefulness decrease, you may feel concern that your actions will result in the patient’s death. The fear of administering the last dose of pain medication is real and shouldn’t be dismissed, but education can help alleviate it. Remember the concept of intent. When a patient dies after pain medication administration, your intent is to provide comfort, not to take the patient’s life.
All major nursing organizations (including the American Nurses Association, Oncology Nursing Society, and the Hospice and Palliative Nurses Association) support the concept of intent. Keep in mind that someone will always give the last dose, whether it’s you or another nurse. In addition to making the patient as comfortable as possible, providing pain control eases loved ones’ concerns and ensures the grieving process is a little less difficult.
Effective advocacy
Patients in pain frequently can’t speak up for themselves, especially as they approach the end of life. To advocate effectively for patients, familiarize yourself with the various pain management agents and strategies. Understanding opioid half-life, tolerance and rotation, as well as tolerance and intent, will help you support vulnerable patients.
Diana Karius is a clinical nurse specialist at Cleveland Clinic in Cleveland, Ohio.
References
American Nurses Association. Position statement: The ethical responsibility to manage pain and the suffering it causes. 2018. nursingworld.org/practice-policy/nursing-excellence/official-position-statements/id/the-ethical-responsibility-to-manage-pain-and-the-suffering-it-causes
Benítez-Rosario MA, Rosa-González I, González-Dávila E, Sanz E. Fentanyl treatment for end-of-life dyspnoea relief in advanced cancer patients. Support Care Cancer. 2019;27(1):
157-64 doi:10.1007/s00520-018-4309-8
Centeno C. Methadone and dignity: Advanced medicine for the end of life. J Palliat Med. 2017;20(11):1180-1. doi:10.1089/jpm.2017.0516
Coyne P, Mulvenon C, Paice JA. American Society for Pain Management Nursing and Hospice and Palliative Nurses Association position statement: Pain management at the end of life. Pain Manag Nurs. 2018;19(1):3-7. doi:10.1016/j.pmn.2017.10.019
Fitzgerald Jones K. Buprenorphine use in palliative care. J Hosp Palliat Med. 2019;21(6):540-7. doi:10.1097/NJH.0000000000000598
International Association for the Study of Pain. IASP announces revised definition of pain. July 16, 2020. iasp-pain.org/PublicationsNews/Newsdetail.aspx?ItemNumber=10475
National Consensus Project for Quality Palliative Care. Clinical Practice Guidelines for Quality Palliative Care. 4th ed. 2018. National Coalition for Hospice and Palliative Care.
nationalcoalitionhpc.org/wp-content/uploads/2020/07/NCHPC-NCPGuidelines_4thED_web_FINAL.pdf
Paice JA. Pain. In: Dahlin C, Coyne P, Ferrell B, eds. Clinical Pocket Guide to Advanced Practice Palliative Nursing. New York, NY: Oxford University Press; 2017; 1-14.
Paice JA. Pain management. In: Rolling Ferrell BR, Paice JA, eds. Oxford Textbook of Palliative Nursing. 5th ed. New York, NY: Oxford University Press; 2019; 116-31.
Portenoy RK, Mehta Z, Ahmed E. Prevention and management of side effects in patients receiving opioids for chronic pain. UpToDate. January 3, 2022. uptodate.com/contents/prevention-and-management-of-side-effects-in-patients-receiving-opioids-for-chronic-pain
Raja SN, Carr DB, Cohen M, et al. The revised International Association for the Study of Pain definition of pain: Concepts, challenges, and compromises. Pain. 2020;161(9):1976-82. doi:10.1097/j.pain.0000000000001939
Swarm RA, Paice JA, Anghelescu DL, et al. Adult cancer pain, version 3.2019, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2019;17(8):977-1007doi:10.6004/jnccn.2019.0038


















