Data transparency aids care quality improvement.
- To help patients and their families make informed decisions about choosing health care, the Centers for Medicare and Medicaid Services (CMS) publicly reports quality performance measures.
- With understanding of these reported measures, nurses can lead improvements in healthcare with evidence-based practice that improves patient outcomes and reduces healthcare costs.
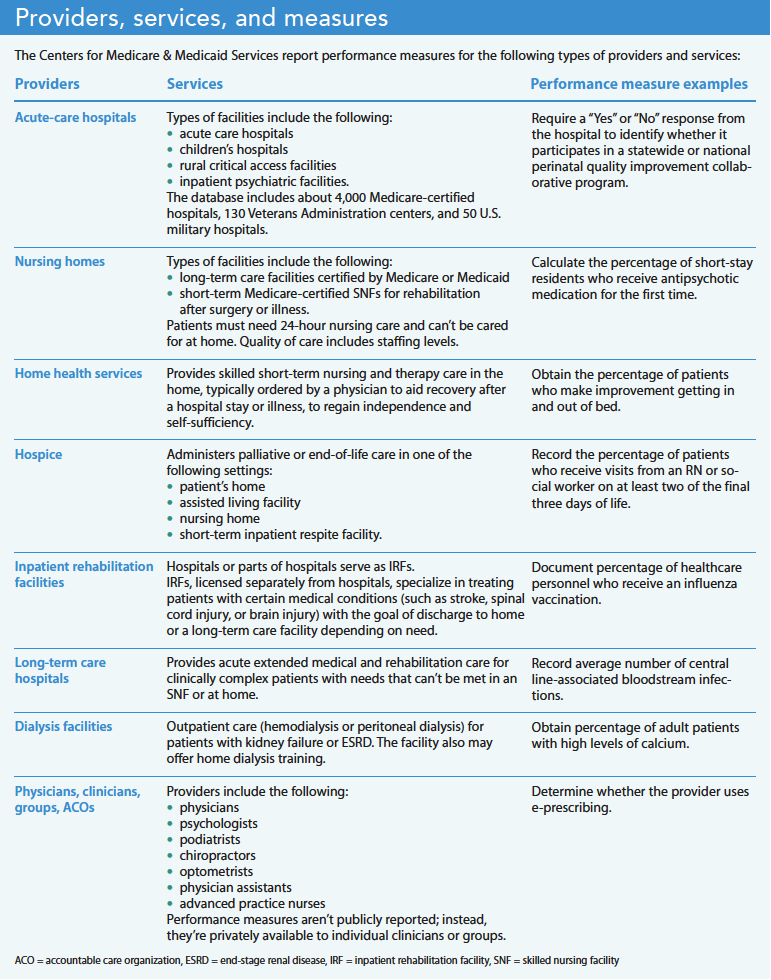
Medicare, the largest payer of medical expenses in the United States, provides primary health insurance for more than 60 million beneficiaries. To help patients and their families make informed healthcare choices, the Centers for Medicare & Medicaid Services (CMS) publicly reports quality performance measures for eight types of providers on the Medicare Care Compare website (medicare.gov/care-compare). In addition to informing patients, public reporting can drive providers to improve performance. (See Providers, services, and measures.)
According to a 2023 report by the Commonwealth Fund (an independent research group), the United States spends twice as much per year on healthcare compared to other high-income countries but has worse outcomes, including the shortest life expectancy, highest maternal and infant mortality, highest death rates for avoidable or treatable conditions, and highest rate of people with multiple chronic diseases. A central reason for this mismatch between cost and quality is a payment model that encourages quantity of services without always holding providers accountable for treatment effectiveness.
Several landmark reports by the Institute of Medicine (now known as the National Academy of Medicine [NAM]) explain the need to build a safer and more effective healthcare system and provide recommendations for improvement. The reports present a national agenda to redesign and improve the American healthcare system by identifying provider performance expectations and aligning payment with better patient outcomes. The framework for measuring quality of care includes the following:
- Effectiveness: Care is based on evidence, and every patient interaction and service moves the patient closer to meeting their goals.
- Efficiency: Providers use only needed resources, without duplicate or unnecessary care.
- Equity: Care doesn’t vary in quality based on personal characteristics such as race, gender, and income.
- Patient centeredness: Each patient’s values, preferences, and needs are respected and incorporated into the plan of care.
- Safety: Treatment doesn’t cause harm.
- Timeliness: Treatment is available without long delays.
You can view free NAM publications about healthcare quality, provider performance measurement, and payment at nam.edu.
Medicare Care Compare
The Medicare Care Compare website publicly reports providers’ performance and has a search feature for finding services and providers in a geographic area or a specific provider by name. Users can view each provider separately or compare up to three providers side-by-side. The site also shows how providers compare on each measure with similar providers locally and nationwide.
Although many Medicare beneficiaries are older, CMS requires that hospitals receiving Medicare payments also report performance measures intended to improve health for younger populations. For example, users can find maternal care information related to the percentage of mothers whose deliveries were scheduled before 39 weeks of pregnancy, when a scheduled delivery wasn’t medically necessary. For surgical centers, users can discover the rate of unplanned hospital visits within 7 days of orthopedic surgery.
Medicare Care Compare also includes individual physicians, advanced practice nurses, and other prescribing clinicians to help the public find providers enrolled in Medicare. The site includes general information about clinicians and groups (names, addresses, phone numbers, and medical specialties) as well as details about board certification, education, gender, and group and hospital affiliation. Some clinicians receive organization or group-based scores rather than individual scores.
In addition, individual Medicare-certified healthcare providers have access to dozens of performance measures and comparisons not available to the public. The Merit-Based Incentive Payment System (MIPS) and Alternative Payment Models (APMs) collect these measures, which providers can use to increase Medicare payment based on quality of care.
Where quality scores come from
Various researchers from universities and other settings develop and select CMS performance measures. Since 2015, the CMS-sponsored Core Quality Measures Collaborative (CQMC), a group of healthcare leaders, has represented several healthcare and payment organizations. Nurses frequently lead the development and testing of the performance measures. Originally, CQMC resided at the National Quality Forum (NQF) in Washington, D.C., which creates workgroups to set priorities and goals in evidence-based measure selection that can be used across care settings. Now, Battlelle, an independent nonprofit research organization, reviews and endorses measures for federal programs.
Although many performance measures differ among each type of healthcare setting, they follow a similar format. For example, patient education about medication serves as a performance measure in all healthcare settings, whereas preventing unnecessary hospitalization relates to post-acute care settings.
The NAM reports classify healthcare quality measures as structural, process, outcome, cost of care, or patient experience of care. Structural measures describe the healthcare provider or facility (for example, use of electronic health records and the provider–patient ratio). Process measures indicate what the provider does (for example, the length of time a patient remains in the emergency department [ED] or the tests routinely performed for a specific medical condition).
Outcome measures may include the incidence of repeat hospitalizations, surgical mortality rates, or the ability of the patient to remain in the community after discharge from home healthcare. Frequently, providers report measures using standardized documentation required by CMS. For example, skilled nursing facilities use the Minimum Data Set (MDS), home healthcare uses the Outcome and Assessment Information Set (OASIS), and hospice care uses the Hospice Outcomes and Patient Evaluation (HOPE). When possible, CMS uses measures taken from claims and Medicare billing information. Researchers can access de-identified government data (such as rehospitalization rates and ED visits without hospitalization), which are in the public domain, at data.cms.gov/provider-data.
A value measure for a specific provider organization also shows whether Medicare spends more, the same, or less on an episode of care compared to the national average for that type of provider (cost of care). The national average value number is 1. A higher score indicates that Medicare spends more per patient; a lower score, that Medicare spends less; and a score of 1, that Medicare spends about the same per patient for an episode of care. CMS defines “value” as improvement in health outcomes for the cost of achieving that improvement. The cost of care for surgery or treating a specific medical condition can vary by thousands of dollars for organizations in the same city.
Patient experience of care represents the patient’s reported perception of care received and whether they would recommend the provider to others. This measure is reported separately from facility-collected performance data. According to the Agency for Healthcare Research and Quality, an independent contractor surveys recently discharged patients using the Consumer Assessment of Healthcare Providers and Systems (CAHPS). The questions differ slightly for each type of healthcare setting, but CAHPS asks about provider communication and staff responsiveness to patient needs in all settings.
Star ratings
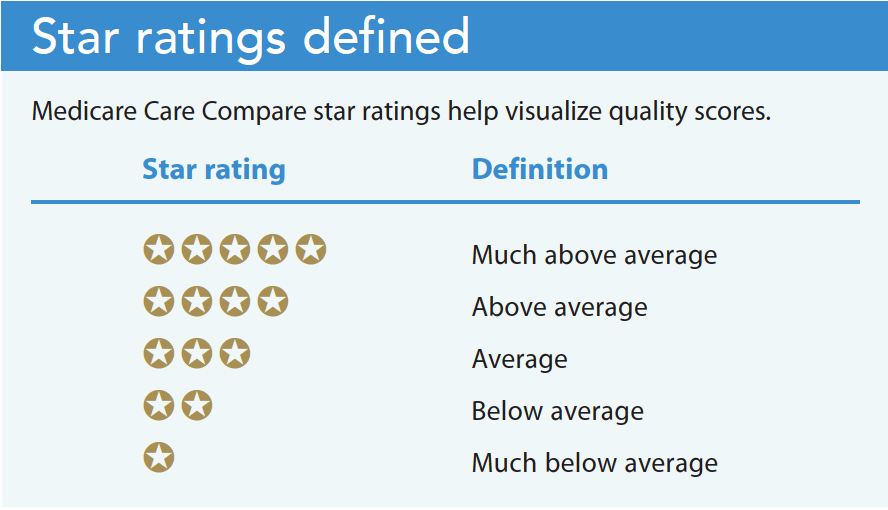
To make quality scores easier to visualize on the Medicare Care Compare website, quality ratings range from 1 to 5 stars (more stars indicate better quality care). Measures included in the star ratings differ by type of organization, but all have an overall star rating and a patient survey rating. Frequently, a difference exists between the overall care star rating reported by the organization and the CAHPS star rating. (See Star ratings defined.)
Much of the data used to calculate the star rating system come from clinical documentation. When provided care isn’t adequately documented, the star rating may not fully represent the quality of care provided. This highlights the importance of documenting nursing assessments and interventions.
The complex star rating system weighs and combines many measures for facets of care to establish the overall provider rating. For the hospital quality star rating, in addition to the patient experience of care, the overall score summarizes measures related to mortality, safety, readmission, and timely and effective care. Each area has multiple measures. For example, the mortality measure includes seven specifics for death rates from heart attack, stroke patients, and other causes. In addition, the area of timely and effective care includes specific measures for inpatient and outpatient care, including the percentage of patients who left the ED before being seen and follow-up after an outpatient colonoscopy procedure.
For the 15,000 skilled nursing facilities that receive Medicare payments, three sources of star ratings for the overall measure include unannounced annual health inspections by state inspectors, staff levels and turnover, and quality-of-care measures documented in the MDS resident assessment document. Staffing levels reflect RN hours per resident per day and total nurse staffing (including RN, licensed practical nurse/licensed vocational nurse, and nurse aide hours per resident per day). Weekend nurse staffing on Saturdays and Sundays also is monitored and reported. Medicare no longer uses facility-reported staff numbers; instead, it derives the measure from facilities’ payroll data, which, according to Gandhi and colleagues, has improved staff level measurement accuracy.
Achieve national goals
Publicly reported performance measures help achieve national goals for improving the patient experience of care, enhancing population health outcomes, advancing health equity, decreasing costs, and improving clinician work life and well-being. Nurses serve as patient advocates when they teach patients and the public about Medicare Care Compare to find providers based on their individual needs.
Susan M. Hinck is a community health nurse at Springfield Greene County Health Department in Springfield, Missouri.
American Nurse Journal. 2023; 18(5). Doi: 10.51256/ANJ052348
References
Agency for Healthcare Research and Quality. CAHPS patient experience surveys and guidance. May 2022. ahrq.gov/cahps/surveys-guidance/index.html
Centers for Medicare & Medicaid Services. Care Compare: Doctors and clinicians initiative. March 8, 2023. cms.gov/medicare/quality-initiatives-patient-assessment-instruments/physician-compare-initiative
Centers for Medicare & Medicaid Services. Consumer assessment of healthcare providers & systems (CAHPS). January 25, 2023. cms.gov/Research-Statistics-Data-and-Systems/Research/CAHPS
Centers for Medicare & Medicaid Services. Core measures. December 1, 2021. cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/QualityMeasures/Core-Measures
Centers for Medicare & Medicaid Services. Design for Care Compare nursing home five-star quality rating system: Technical users’ guide. January 2023. cms.gov/Medicare/Provider-Enrollment-and-Certification/CertificationandComplianc/downloads/usersguide.pdf
Centers for Medicare & Medicaid Services. Five-star quality rating system. February 21, 2023. cms.gov/Medicare/Provider-Enrollment-and-Certification/CertificationandComplianc/FSQRS
Connor L, Dean J, McNett M, et. al. Evidence-based practice improves patient outcomes and healthcare system return on investment: Findings from a scoping review. Worldviews Evid Based Nurs. 2023;20(1):6-15. doi:10.1111/wvn.12621
Gandhi A, Yu H, Grabowski DC. High nursing staff turnover in nursing homes offers important quality information. Health Aff. 2021;40(3):384-91. doi:10.1377/hlthaff.2020.00957
Gunja MZ, Gumas ED, Williams RD. U.S. Health Care from a Global Perspective, 2022: Accelerating Spending, Worsening Outcomes. Commonwealth Fund. January 2023. commonwealthfund.org/publications/issue-briefs/2023/jan/us-health-care-global-perspective-2022
Lewis C, Horstman C, Blumenthal D, Abrams MK. Value-based care: What it is and why it’s needed. Commonwealth Fund. February 7, 2023. commonwealthfund.org/publications/explainer/2023/feb/value-based-care-what-it-is-why-its-needed
Key words: Medicare, Medicare Care Compare, performance measures, value-based purchasing