Learn about heart failure medications to ensure improved outcomes
Takeaways:
- Learn about the newest medications to treat heart failure, including adverse effects, indications, and nursing implications.
- Stages and classes of heart failure established by the American Heart Association and the New York Heart Association aid in determining the best medication for specific patients.
 HEART FAILURE currently affects six million Americans, with an estimated 870,000 new cases annually. Reasons for this increase include an aging population; comorbid conditions such as diabetes, hypertension, and obesity; and higher survival rates after heart attacks, which can predispose survivors to heart failure.
HEART FAILURE currently affects six million Americans, with an estimated 870,000 new cases annually. Reasons for this increase include an aging population; comorbid conditions such as diabetes, hypertension, and obesity; and higher survival rates after heart attacks, which can predispose survivors to heart failure.
No matter where you work as a nurse, caring for a patient with heart failure is inevitable, so you should know which medications will provide the most benefit and the potential side effects you’ll need to assess for. This article reviews the medications recommended by the American Heart Association (AHA) and the American College of Cardiology Foundation Guideline for the Management of Heart Failure.
Stages and classes of heart failure
Two reliable indices are used to stratify heart failure: the AHA stages and the New York Heart Association (NYHA) functional classes.
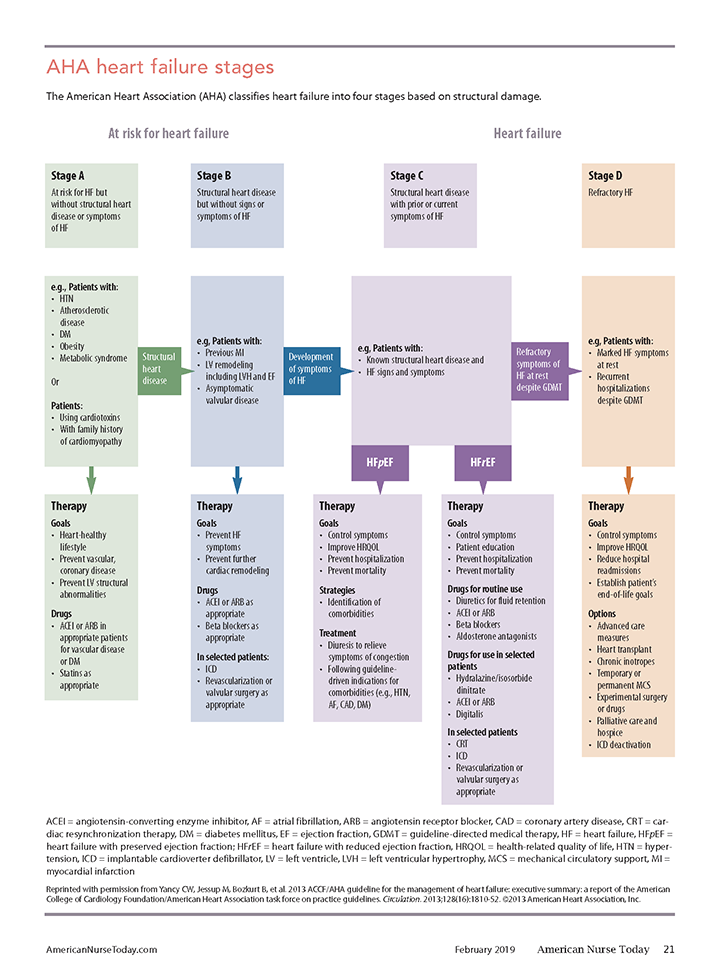
The AHA classifies heart failure into four stages based on structural heart damage. (See AHA heart failure stages.) Stages A and B require minimal medications. Stage C is broken into two categories— heart failure with a preserved ejection fraction (HFpEF, ejection fraction > 45%) and heart failure with reduced ejection fraction (HFrEF, ejection fraction < 45%). Patients fall into these categories based on their left ventricle’s ability to pump blood or relax and fill with blood. Stage D of the AHA classification requires additional interventions beyond medication.
Originally published in 1928 and updated over the years (the last update was 1994), the NYHA heart failure classification is still used today. It categorizes classes I through IV according to subjective patient symptom assessment. (See NYHA heart failure classification.)
NYHA heart failure classificationThe New York Heart Association (NYHA) system classifies heart failure based on a patient’s ability to function in daily life.
|
Medication classes
Heart failure treatment requires careful balancing of several medications that affect preload (amount of ventricular stretch at the end of diastole) and afterload (pressure the heart must work against to eject blood). In addition to the following medication classes, hydralazine/isosorbide dinitrate, sacubitril/valsartan, and ivabradine are indicated for heart failure treatment. (See New medications for treating heart failure.)
New medications for treating heart failureThese three new medications can be used to treat heart failure. Hydralazine/isosorbide dinitrate The drugs isosorbide dinitrate and hydralazine have been combined into a single pill to reduce both cardiac preload and afterload through venous and arterial vasodilation. Indications: This medication decreases deaths and hospitalization in African Americans, who are less responsive to angiotensin-converting enzyme (ACE) inhibitors because of suspected differences in endothelial function. Adverse effects: Adverse effects include headache, dizziness, and orthostatic hypotension. Nursing points: Advise patients to change position slowly to prevent falls due to postural changes in blood pressure. Ivabradine Ivabradine, the first sinoatrial (SA)-node modulator approved to treat heart failure, decreases normal SA node activity and lowers heart rate. It does not affect myocardial contractility. Indications: Ivabradine decreases hospitalizations in patients with poor ejection fraction (< 35%) and resting heart rate > 70 beats per minute (bpm). Adverse effects: Adverse effects include bradycardia and hypotension. Nursing points: Administer ivabradine as ordered if a patient’s heart rate is ≥ 70 bpm. Sacubitril/valsartan This is the first in a new class of heart failure medication called angiotensin receptor neprilysin inhibitors. It combines an angiotensin receptor blocker (valsartan) with a neprilysin enzyme inhibitor (sacubitril). Neprilysin breaks down natriuretic peptides, which are responsible for sodium and water loss when ventricles are overloaded. Delaying their breakdown lengthens their effects and removes more sodium and water from the body, decreasing intravascular volume and blood pressure, resulting in decreased preload and afterload. Indications: Sacubitril/valsartan is indicated to reduce the risk of hospitalization and death in patients with chronic heart failure and reduced ejection fraction. Adverse effects: Adverse effects include dizziness, fatigue, cough, hypotension, and hyperkalemia. Nursing points: Sacubitril/valsartan should not be given with an ACE inhibitor. |
Angiotensin-converting enzyme inhibitors
Angiotensin-converting enzyme (ACE) inhibitors cause vasodilation in both the venous and arterial systems, so they decrease both preload and afterload, increasing blood flow to vital organ systems and improving ejection fraction. These medications also block the enzyme needed to convert angiotensin I to angiotensin II. Angiotensin II is a strong vasoconstrictor that raises blood pressure, releases aldosterone, and leads to sodium and water retention. ACE inhibitors prevent this cascade of effects.
Examples: Captopril, enalapril, and lisinopril.
Indications: ACE inhibitors decrease the risk of death and hospitalizations in patients with HFrEF.
Adverse effects: Adverse effects include hyperkalemia, renal failure, and a dry, persistent cough associated with increased bradykinin. If the cough is intolerable, the provider may discontinue the ACE inhibitors in favor of an angiotensin receptor blocker (ARB).
Nursing points: Although the cough can be annoying, explain to the patient that it’s a side effect of the medication and encourage him or her to continue its use.
Angiotensin receptor blockers
Similar to ACE inhibitors, ARBs block the action of angiotensin II. However, they work at a different level of interaction with angio ten – sin II, reducing the risk of hyperkalemia or cough that’s seen with ACE inhibitors. ARBs block angiotensin II receptors in the blood vessels and the adrenal glands. In the blood vessels, ARBs cause venous and arterial dilation to reduce both preload and afterload. Blocking angiotensin II receptors in the adrenal glands decreases the release of aldosterone, which in turn increases the excretion of sodium and water.
Examples: Valsartan and losartan.
Indications: ARBs are sometimes substituted for patients who can’t tolerate ACE inhibitors.
Adverse effects: ARBs are well tolerated and have minimal side effects.
Nursing points: ARBs and ACE inhibitors shouldn’t be used interchangeably. ACE inhibitors are preferred over ARBs because they’re associated with a decrease in morbidity and mortality.
Beta blockers
Beta blockers decrease sympathetic nervous system stimulation, lowering heart rate and blood pressure and improving left ventricular function, hemodynamics, and exercise tolerance. They have moderate afterload reduction effects and slightly reduce preload.
Examples: Bisoprolol, carvedilol, sustained-release metoprolol.
Indications: Beta blockers slow the progression of symptoms in patients with HFrEF and allow more time for ventricular filling prior to ejection in patients with HFpEF.
Adverse effects: Adverse effects of beta blockers include fluid retention, fatigue, bradycardia, and hypotension.
Nursing points: Fluid retention may worsen heart failure but can usually be managed with diuretics. If bradycardia or hypotension are problematic, the provider may reduce the beta blocker dose. Because of decreased heart rate and blood pressure associated with beta blockers, they shouldn’t be administered at the same time as ACE inhibitors.
Diuretics
Loop diuretics act on the ascending limb of the loop of Henle to inhibit sodium and chloride reabsorption, leading to increased urinary excretion of sodium and water.
Examples: Furosemide, bumetanide, and torsemide.
Indications: Loop diuretics are the preferred diuretics to increase urinary excretion of sodium and water when managing heart failure. Dose adjustments may be necessary based on sodium and fluid intake.
Adverse effects: Electrolyte loss.
Nursing points: Instruct patients to decrease their dietary intake of sodium, weigh themselves daily, and take the diuretic early in the day to prevent nocturia. Hypokalemia is a side effect of loop diuretics, so monitor patients’ serum potassium levels.
Aldactone antagonists
Aldactone antagonists decrease all-cause mortality, sudden cardiac death, and heart failure symptoms when added to the treatment regimen of patients with heart failure and HFrEF.
Examples: Spironolactone or eplerenone.
Indications: Aldactone antagonists are indicated for use in patients with HFrEF.
Adverse effects: Aldactone antagonists inhibit potassium excretion and may lead to hyperkalemia.
Nursing points: Advise patients taking an aldactone antagonist to avoid salt substitutes, nonsteroidal anti-inflammatory drugs, and foods high in potassium to reduce the risk of hyperkalemia. Monitor serum potassium, blood urea nitrogen, creatinine, and creatinine clearance levels. If a patient also is taking an ACE inhibitor, assess for signs of renal insufficiency.
Improving outcomes
When you understand the mechanisms of action, indications, and adverse effects of the medications used to treat heart failure, you can deliver nursing care that improves outcomes and provide patients and family members with the education they need to manage the condition.
Kelley H. Pattison is an assistant professor at Western Michigan University, Bronson School of Nursing in Kalamazoo.
Selected references
Arcangelo VP, Peterson AM, Wilbur V, Reinhold JA. Pharmacotherapeutics for Advanced Practice: A Practical Approach. 4th ed. Philadelphia, PA: Wolters Kluwer; 2017.
Benjamin EJ, Blaha MJ, Chiuve SE, et al. Heart disease and stroke statistics—2017 update: A report from the American Heart Association. Circulation. 2017;135(10):e146- 603.
Burchum J, Rosenthal L. Lehne’s Pharmacology for Nursing Care. 10th ed. St. Louis, MO: Elsevier; 2019.
Dolgin M; Criteria Committee of the New York Heart Association. Nomenclature and Criteria for Diagnosis of Diseases of the Heart and Great Vessels. 9th ed. Boston, MA: Little Brown & Co; 1994.
Gordin JS, Fonarow GC. New medications for heart failure. Trends Cardiovasc Med. 2016;26(6):485-92.
Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology Foundation/American Heart Association task force on practice guidelines. J Am Coll Cardiol. 2013;62(16): E147-239.
Yancy CW, Jessup M, Bozkurt B, et al. 2017 ACC/AHA/HFSA focused update of the 2013 ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines and the Heart Failure Society of America. J Am Coll Cardiol. 2017;70(6):776-803.
ant2-Heart Failure-118

















