
Bringing stroke diagnosis and treatment to your front door.
- Mobile stroke units (MSUs) are specialized ambulances equipped to evaluate, diagnose, and treat strokes in the prehospital environment.
- They’ve been shown to reduce door-to-treatment time by bringing specialized healthcare providers, compute tomography imaging, and thrombolytic therapy to the patient’s front door.
- Patients who receive care in an MSU not only benefit from early diagnosis and potential treatment with thrombolytics but also benefit from triage to appropriate comprehensive stroke centers for additional neurologic care.
According to the American Heart Association, someone dies from a stroke every 3 minutes and 33 seconds, and 64% of these strokes occur outside of the hospital. Treatment with I.V. thrombolytics, the standard of care for ischemic strokes, can be administered only within the first 4.5 hours of when the patient was last known to be well, preferably within the first 60 minutes after the onset of stroke symptoms. Thrombolytics quickly dissolve the blood clot causing the stroke and restore blood flow to the affected brain tissue. (See Stroke stats.)
Mobile stroke units (MSUs), ambulances equipped to evaluate, diagnose, and treat strokes in the prehospital environment, decrease door-to-thrombolytic administration time, cut door-to-thrombectomy time, reduce the risk of mortality and long-term disability, and improve patient outcomes.
Stroke stats
According to the American Heart Association
- Approximately 795,000 Americans experience new or recurrent ischemic or hemorrhagic strokes annually.
- More than 147,000 of these individuals die.
- 87% of strokes are ischemic (caused by a blood clot in the brain).
- 13% of strokes are hemorrhagic (caused by a ruptured blood vessel in the brain), including intracerebral and subarachnoid hemorrhage.
- Strokes are the fifth leading cause of death in the United States and a major cause of serious long-term disability.
MSU history
The first MSU, established in Germany in 2008 and similar to current MSUs, consisted of a specialized ambulance equipped with a CT scanner, specially trained healthcare providers, point-of-care (POC) laboratory equipment, telemedicine, and thrombolytics. The onboard crew provided diagnosis and treatment at the scene, triaged the patient, and transported them to an appropriate stroke center for further evaluation and care. The MSU model soon spread to other countries, including the United States, where Memorial Hermann-Texas Medical Center in Houston initiated the first program in 2014. Research continues to demonstrate positive patient outcomes and benefits.
MSU crews
In the United States, typical MSU crews include one to two paramedics, an RN, a CT technologist, and a neurologist who’s consulted remotely via telemedicine. The RNs and paramedics require high-level qualifications, including Advanced Cardiac Life Support, National Institutes of Health Stroke Scale (NIHSS) certification, and advanced airway management training. They also must receive additional stroke training and education, as well as annual stroke-specific continuing education. The onboard crew communicates via telemedicine with the dedicated neurologist who collaborates with a neuro-radiologist to review CT imaging obtained in the MSU.

MSU equipment
MSUs vary, but most carry equipment that standard advanced life support (ALS) ambulances don’t. Onboard equipment typically includes a head CT scanner, mobile WiFi, telemedicine capabilities, neurology-specific medications, POC laboratory equipment, advanced airway technology, a transport ventilator, I.V. infusion pumps, and equipment for ultrasound-guided I.V. insertion. The CT scanner is the most significant piece of equipment that differentiates an MSU from a typical ALS ambulance. With the ability to visualize the brain and intracranial circulation in the prehospital setting, CT scanning and CT angiography (CTA) can aid prehospital diagnosis of ischemic strokes, large vessel occlusion, and intracranial hemorrhages.
Many MSUs come equipped with secure mobile WiFi and telemedicine, which allows a neurologist to examine the patient and speak with family members at the scene. Mobile WiFi also permits the MSU crew to review the patient’s electronic health record (EHR) and, in some cases, electronically sign off orders and document medication administration in real time. MSU laboratory equipment includes specialized POC tools for reporting a basic metabolic panel, hemoglobin and hematocrit, blood glucose level, and international normalized ratio.
Although no standardization exists for MSU medications, most have thrombolytics, anti-epileptic drugs (AEDs), mannitol, hypertonic saline, phytonadione (vitamin K), and prothrombin complex concentrate (PCC). AEDs, such as phenytoin and levetiracetam, treat post-stroke seizure activity; hyperosmolar medications, such as mannitol and hypertonic saline, treat cerebral edema; and vitamin K and PCC aid anticoagulation reversal in patients with coagulopathy.
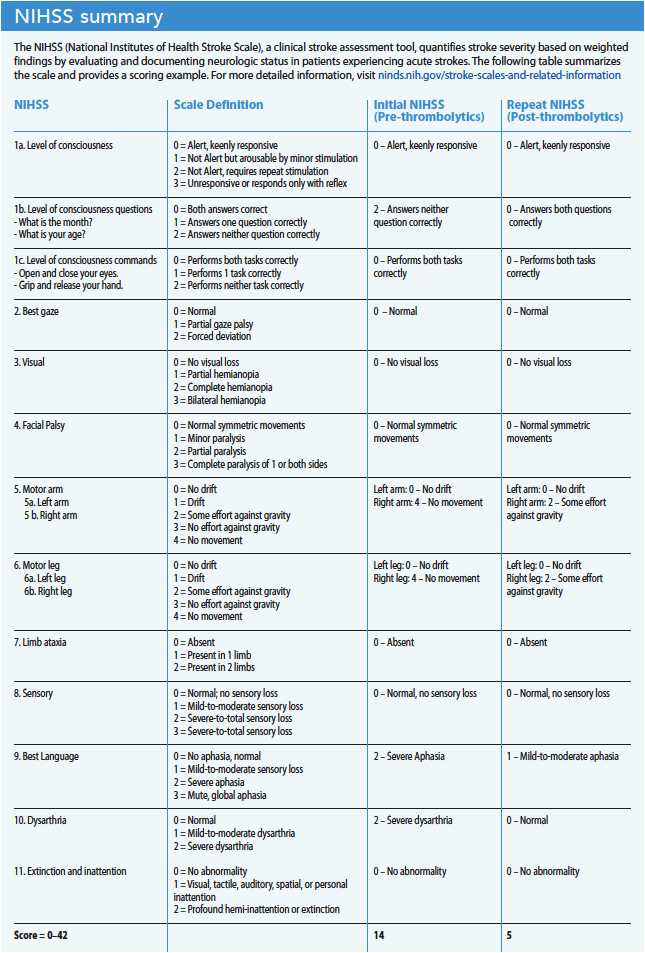
The MSU RN and paramedic establish peripheral I.V. access and draw blood for laboratory analysis while simultaneously performing a physical assessment and NIHSS examination, obtaining past medical history (including home medications and allergies), and providing report to the neurologist on the telemedicine screen. Mr. Harrison’s NIHSS is 14: 2 for level of consciousness questions (not alert, requires repeat stimulation), 4 for right arm (no movement), 4 for right leg (no movement), 2 for best language (severe aphasia), and 2 for dysarthria (severe dysarthria). The onscreen neurologist places orders for a non-contrast CT of the head and POC lab work into the patient’s EHR. All MSU crew members don lead aprons and neck protection as the CT technologist completes the head scan. (See NIHSS summary)
The technologist sends the CT results to a picture archiving and communication system, which makes the imaging available to the MSU neurologist and the collaborating neuro-radiologist. The MSU crew completes the POC lab work and communicates the results to the neurologist. After reviewing the CT imaging, the neurologist determines that Mr. Harrison doesn’t have a hemorrhage. The MSU neurologist and crew discuss whether the patient meets inclusion criteria for thrombolytic therapy and then speak with Mr. Harrison and his family to explain the risks and benefits of this treatment.
MSUs and thrombolytics
Alteplase (0.9 mg/kg with a maximum total dose of 90 mg) has been the gold standard for thrombolytic therapy in the treatment of acute ischemic strokes since 1996 when it was approved by the U.S. Food and Drug Administration. Initially, 10% of the total dose is given as an I.V. bolus over 1 minute, with the remaining dose given as an I.V. infusion over 60 minutes. (See Thrombolytic history.)
Thrombolytic history
Thrombolytics were discovered in the early 1930s, but they weren’t recognized as a treatment for acute ischemic strokes until the 1950s. However, it wasn’t until the 1970s, with the invention of computed tomography (CT) to aid differentiating between ischemic and hemorrhagic strokes, that experts recognized the vital role thrombolytics can play in early treatment. In 1995, a study by the National Institute of Neurological Disorders and Stroke demonstrated alteplase as an effective treatment for acute ischemic strokes.
Taqui and colleagues compared MSU evaluation and treatment times to a control group of patients transported to the emergency department (ED) via traditional emergency medical services (EMS). They concluded that MSUs administered thrombolytics 38.5 minutes faster than when patients were transported to the ED via EMS. Grotta and colleagues also compared treatment times between MSU and traditional EMS. They showed that the percentage of patients treated with thrombolytics within 60 minutes of the last time they were known to be well was 33% via MSUs and only 3% via traditional EMS transport. This study also showed a decrease in mortality and long-term disability at 90 days.
After Mr. Harrison and his family agree to proceed with thrombolytic therapy, the neurologist orders alteplase, which she calculates based on the patient’s weight of 187 lbs. (85 kg). The RN and paramedic verify and administer a 7.7 mg alteplase I.V. bolus over 1 minute and then initiate an I.V. infusion of 68.8 mg alteplase over 60 minutes (total dose of 76.5 mg). The neurologist determines the appropriate destination for Mr. Harrison based on the patient’s preference, where he typically receives care, and the capabilities of the facility. After choosing the destination, the neurologist calls report to the receiving hospital’s ED physician and the MSU transports the patient.
During travel to the hospital, the MSU team continually monitors Mr. Harrison. If he requires any treatment for hypertension or has other needs during transport, the team will contact the onscreen neurologist to receive and implement orders immediately.
The MSU RN communicates the patient report and an estimated time of arrival to the receiving ED charge nurse. On the way to the hospital and after receiving thrombolytic treatment, Mr. Harrison shows significant improvement, including increased right upper and lower extremity strength, decreased aphasia, and absence of dysarthria. When Mr. Harrison and the crew arrive at the ED, his NIHSS has improved with a repeat score of 5: 2 each for right arm and right leg (some effort with gravity) and 1 for best language (mild-to-moderate aphasia).
Additional benefits
According to American Stroke Association guidelines, patients who meet inclusion criteria for administration of thrombolytic therapy should receive I.V. thrombolytics even if mechanical thrombectomy is still being considered. Not only have MSUs demonstrated faster treatment times with I.V. thrombolytics, when compared to standard ED care, they also have demonstrated faster treatment times for patients requiring urgent thrombectomy.
A study by Czap and colleagues found that patients presented for endovascular thrombectomy 53.5 minutes faster when the MSU team performed a CTA compared to waiting to arrive at the ED. In addition, the diagnosis of large vessel occlusion in the field prompted appropriate triage to a thrombectomy-capable facility and direct admission to a thrombectomy suite. A study by Reimer and colleagues also noted significant cost savings when transferring patients directly to comprehensive stroke centers compared to unnecessary secondary interhospital transfers and ED admissions.
In addition to diagnosing and treating ischemic strokes, MSUs also have benefited patients experiencing hemorrhagic strokes and status epilepticus. The benefits of an MSU for these patients include early recognition and diagnosis, coagulation reversal with specialized medications (PCC and vitamin K), anti-epileptic drug administration, and advanced airway management. Cooley and colleagues demonstrated that early recognition of hemorrhagic strokes on MSUs leads to rapid triage and transport to comprehensive stroke centers for early surgical intervention.
Changing lives
Achieving the best possible outcomes for patients experiencing acute ischemic strokes requires treatment soon after symptom onset. MSUs reduce door-to-treatment and door-to-thrombectomy time by bringing specialized healthcare providers, CT imaging, and thrombolytic therapy to the patient and ensuring transfer to appropriate facilities, including comprehensive stroke centers for additional neurologic care. When every second counts, MSUs can dramatically change the course of a patient’s life.
*Name is fictitious.
Learn more
To learn more about treatment of acute ischemic stroke, access the following resources from the American Heart Association and American Stroke Association:
- Acute ischemic stroke: Current treatment approaches for acute ischemic stroke (bit.ly/3ZdNNdc): This PowerPoint presentation provides a quick overview of each step in the care of patients experiencing an acute ischemic stroke—from identification and emergency services transport to inclusion and exclusion criteria for treatment of acute ischemic stroke with I.V. thrombolysis.
- Acute ischemic stroke resources (bit.ly/3EB3Mdh): This page offers access to many resources, including case studies, a stroke simulation toolkit, and patient tools.
- Guidelines for the early management of patients with acute ischemic stroke (bit.ly/3EwXETi): comprehensive guideline for addressing acute ischemic stroke management from acute symptom onset in the prehospital phase through two weeks post-acute stroke.
Rachel Bradley is a critical care transport nurse at the Cleveland Clinic in Cleveland, Ohio.
American Nurse Journal. 2023; 18(4). Doi: 10.51256/ANJ042354
References
Ashcraft S, Wilson SE, Nyström KV, et al. Care of the patient with acute ischemic stroke (prehospital and acute phase of care): Update to the 2009 Comprehensive Nursing Care Scientific Statement: A Scientific Statement from the American Heart Association. Stroke. 2021;52(5):e164-78. doi:10.1161/STR.0000000000000356
Cooley SR, Zhao H, Campbell BCV, et al. Mobile stroke units facilitate prehospital management of intracerebral hemorrhage. Stroke. 2021;52(10):3163-6. doi:10.1161/STROKEAHA.121.034592
Czap AL, Singh N, Bowry R, et al. Mobile stroke unit computed tomography angiography substantially shortens door-to-puncture time. Stroke. 2020;51(5):1613-5. doi:10.1161/STROKEAHA.119.028626
Genentech. Activase (alteplase) prescribing information. September 2022. gene.com/download/pdf/activase_prescribing.pdf
Grotta JC. Fifty years of acute ischemic stroke treatment: A personal history. Cerebrovasc Dis. 2021;50(6):666-80. doi:10.1159/000519843
Grotta JC, Yamal JM, Parker SA, et al. Prospective, multicenter, controlled trial of mobile stroke units. N Engl J Med. 2021;385(11):971-81. doi:10.1056/NEJMoa2103879
National Institute of Neurological Disorders and Stroke. Stroke scales and related information. November 20, 2019. ninds.nih.gov/stroke-scales-and-related-information
Reimer AP, Zafar A, Hustey FM, et al. Cost-consequence analysis of mobile stroke units vs. standard prehospital care and transport. Front Neurol. 2020;10:1422. doi:10.3389/fneur.2019.01422
Röther J, Ford GA, Thijs VNS. Thrombolytics in acute ischaemic stroke: Historical perspective and future opportunities. Cerebrovasc Dis. 2013;35(4):313-9. doi:10.1159/000348705
Taqui A, Cerejo R, Itrat A, et al. Reduction in time to treatment in prehospital telemedicine evaluation and thrombolysis. Neurology. 2017;88(14):1305-12. doi:10.1212/WNL.0000000000003786
UpToDate. Eligibility criteria for the treatment of acute ischemic stroke with intravenous thrombolysis (recombinant tissue plasminogen activator or tPA). 2023. uptodate.com/contents/image?imageKey=NEURO%2F71462
Virani SS, Alonso A, Benjamin EJ, et al. Heart disease and stroke statistics – 2020 update: A report from the American Heart Association. Circulation. 2020;141(9):e139-596. doi:10.1161/CIR.0000000000000757
Key words: mobile stroke unit, stroke, thrombolytics


















