
Develop a plan to address the refusal and support staff.
Takeaways:
- Addressing the issue of patient refusal of a nurse assignment requires understanding three factors: the patient, the nurse, and the organization.
- When faced with patient refusal of a nurse assignment, nursing leadership and the organization must balance their obligations to the patient and the nurse.
- Organizations should develop policies and procedures with input from frontline nurses that supports nurses, and managers must be authentic allies of marginalized groups.
NEW: Our authors discuss patient refusal in this exclusive video!
Focus and attention on the current sociopolitical climate in our communities have led to a renewed reflection on healthcare’s inextricable link with the larger society. Although prioritizing patients’ needs remains the core value of healthcare, awareness of healthcare workers’ experiences with prejudice perpetrated by patients continues to increase. Media reports with titles such as “When the patient is racist” and “Hospital sued for letting patient refuse care from Black nurses” reflect public discourse.
For too long nursing has turned a blind eye to micro- and macro-aggressions committed by patients. The sociopolitical upheaval brought on by COVID-19 and an increased consciousness of health inequities have prompted the need for nuanced discussion of the prejudice healthcare workers experience.
Case exemplar
A 60-year-old White man arrives in the emergency department with shortness of breath caused by an asthma exacerbation. When he’s admitted to the telemetry unit, he’s greeted by a Black female staff member. The patient immediately asks if she’s the nurse’s aide. She responds, “No, I’m your assigned nurse.” The patient says he doesn’t want a Black nurse.
Insufficient research makes it hard to determine the prevalence of such scenarios, but the persistence of racial prejudice and bigotry, in spite of widespread public condemnation, remains one of the many imponderables in our society. To meaningfully address the issue requires an understanding of three factors: the patient, the nurse, and the organization. (See Groundwork for understanding.)
Groundwork for understanding
Addressing a situation in which a patient refuses to be cared for by a specific nurse requires clearly defined terminology related to inclusivity and discrimination. Although each incidence of refusal is unique, the terms below may be relevant.
- Implicit bias—An unconscious association between an individual’s qualities and their race, gender, physical characteristics, or membership in a social group.
Example: A person might associate lower educational status with people of color without being aware they have this bias.
- Microaggressions—Brief and commonplace verbal, behavioral, or environmental indignities, whether intentional or unintentional, that communicate oppressive ideology.
Example: A person might say, “Your English is really good,” to a non-white person who was born in the United States.
- Stereotype threat—Being at risk of confirming, as self-characteristic, a negative stereotype about one’s group.
Example: Emphasizing a staff member’s race at work might undermine their performance because they’re concerned about confirming a negative stereotype (for example, that minorities aren’t smart).
The patient
The Emergency Medical Treatment and Labor Act (EMTALA) requires Medicare-participating hospitals with emergency departments to screen and treat the emergency medical conditions of all patients, regardless of their ability to pay; their insurance status; or their national origin, race, creed, or color. One facet of informed consent is that patients have a right to refuse treatment without retaliation, including refusal of wanted treatment from an unwanted person. Providing care to a patient who refuses it can lead to legal issues such as battery or assault depending on the scenario. However, after a patient is admitted, the hospital’s obligation under EMTALA no longer applies because the mandate only requires providing stabilizing treatment in a medical emergency or offering a medical screening examination.
The nurse
Recognizing the patient’s autonomy and right to self-determination and decision-making is one of the key principles of the Code of Ethics for Nurses with Interpretive Statements. At the same time, nurses have the right to a safe work environment. Although federal and state laws make it illegal to discriminate against employees based on certain characteristics such as race, color, national origin, sex, and religion, it’s unclear how laws govern patient bigotry toward staff. Under Title VII of the Civil Rights Act, an employer “may not discriminate with regard to any term, condition, or privilege of employment.” For example, if a restaurant customer tells the manager they want to be served by a White server and not the Hispanic server, the restaurant would be violating the rights of the Hispanic server if that accommodation is made. Instead, the restaurant may opt to refuse service. In healthcare, a patient can refuse to receive care from a staff member, but the hospital can’t refuse to provide care to a medically unstable patient.
The organization
Hospitals have a duty to provide a safe work environment for nurses and at the same time provide appropriate care to patients. Creating a healthy work environment enables nurses to provide the highest standards of compassionate patient care while being fulfilled at work. Civility and mutual respect between patients and staff are minimum expectations.
Addressing the situation
A patient’s refusal of a nursing assignment opens up a host of questions. If hospital management accommodates the patient’s request, are they discriminating against the nurse? What guides the nurse manager’s or nursing leadership’s decision-making process? Frequently, the affected nurse is from an underrepresented group. How will that nurse feel? If the nursing assignment isn’t changed, is the hospital risking legal action from the patient? Do competent patients have the right to make what may be a bad decision for themselves?
A vital first step in addressing a refusal is to assess the patient’s safety. If the patient’s life is in danger, all efforts must be made to stabilize them, even if a short-term accommodation is needed. After the patient is stabilized, the assigned nurse should feel empowered to ask the patient why they made the request, but this is easier said than done and will require support from the nurse manager, nursing leadership, and the organization.
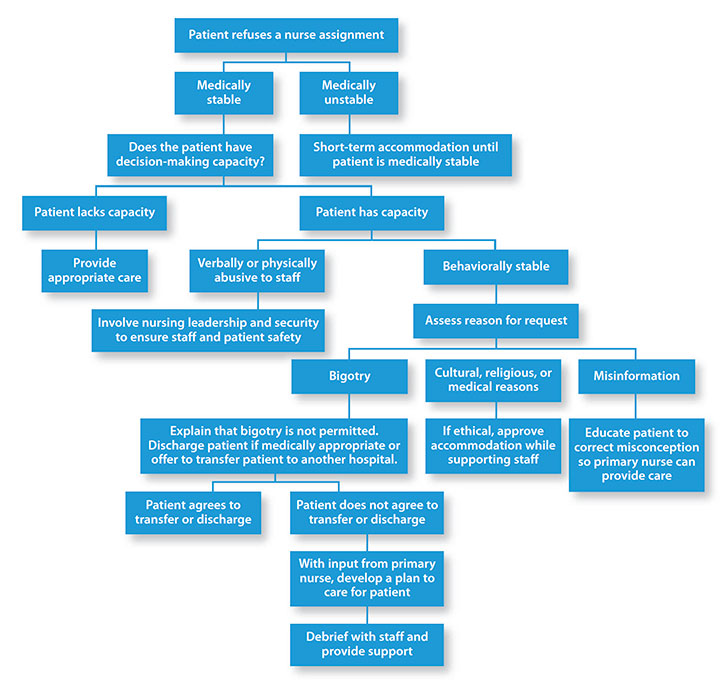
The situation will shake the morale and collective confidence of the team, so the nurse manager will need to provide guidance. Camelo developed an algorithm to guide decision-making in these emotionally charged situations. Staff input was essential to the algorithm’s development, and it will be modified based on ongoing staff feedback. (see Algorithm to address patient refusal.)
Algorithm to address patient refusal
This algorithm, developed by Camelo in collaboration with staff, provides guidance for nurses when patients refuse their care.
Understanding the patient requires nurses to be aware of their own implicit biases, including how their life experiences may impact how they’re interpreting what the patient says. Ask the patient open-ended questions such as, “Help me to understand why you’re requesting that I not care for you. What are your concerns?” If the patient identifies the reason as being because the nurse is in some way different from the patient, the nurse should acknowledge the difference. For example, the nurse can say “Yes, that’s correct. I’m Hispanic, and I’m here to help you get better.”
The nurse can redirect the conversation by letting the patient know that the staff is a diverse group of individuals who are qualified to fulfill a professional role. Politely reminding the patient that the hospital’s goal is the patient’s goal—safe, high-quality care—can help steer the conversation toward the patient with a focus on providing care.
If possible, the nurse should try to determine the reason for the patient’s behavior. It could be based on bigotry, mistrust of the healthcare system from historical disparities and injustice, cognitive impairment, misinformation, and cultural norms.
If derogatory language is being used, the nurse should remind the patient about behavioral expectations while in the hospital. The staff should communicate boundaries early and explain the organization’s zero-tolerance policy regarding abusive language toward staff.
Rearranging patient assignment
The nurse manager should be notified as soon as a patient refuses care so they can support the nurse and speak with the patient. If the request is due to misinformation, the nurse leader or nursing staff can educate the patient. For example, if a patient believes that nurses with accents are trained in inferior schools outside the United States, the nurse can explain that all nurses in the United States must pass the same licensure exam regardless of education origin.
If the reason for the request is due to a cultural norm, such as religious restrictions that prohibit a male staff member to touch a female patient, an accommodation should be made, but the nurse should be involved in the conversation. If the request is the result of bigotry and the patient is stable, the primary provider should discuss offering the patient the option of transferring to another hospital or being discharged. If the patient chooses to have care transferred to another facility, they would be responsible for finding a willing, accepting physician at another facility. The attending physician at the receiving hospital would ultimately need to agree to the transfer after discussing the case with the sending physician. The sending hospital must provide the receiving hospital with clinical documentation, a transfer summary, and comprehensive nursing handoff.
If the receiving hospital is unwilling to accept the patient after learning of the inappropriate behavior, the patient should remain at the current hospital but be informed of firm boundaries related to inappropriate behavior. In addition, staff should continue to receive support from hospital leadership to ensure psychosocial safety at work.
If the patient is unwilling to transfer (or can’t be transferred), is not cognitively impaired, and continues to refuse specific nurses, rearranging the patient assignment should be done only as a last resort and only after conversations with staff members to ensure they feel supported and don’t feel as though the organization condones the request. As necessary, the security department should be notified if the situation escalates and the potential for patient or staff harm exists.
Supporting staff
During the refusal incident, the nurse manager should allow the primary nurse to take the lead in determining what type of support they need. Some nurses may want to handle the situation themselves, while others may require assistance from the manager.
A debriefing immediately after the incident should be open to all team members. The nurse manager can facilitate the discussion, giving staff an opportunity to voice their feelings and concerns. A patient refusal can have a long-lasting influence on a unit, so periodic debriefings should be held to allow staff to learn from the experience. Hospital protocol might require the nurse who was refused by the patient to file a report of the incident with the human resources office with a copy given to the nurse manager.
Patient rejection can be traumatizing and demeaning for the nurse involved and the staff who witness it. Empathy, active listening, and expressions of solidarity with the staff will enhance individual and team resiliency. How these situations are handled brings light to the culture of the unit and the organization as a whole.
Work in progress
Nurses are expected not only to be expert care providers but also competent in dealing with challenging patient behaviors, implicit bias, and microaggression. Unfortunately, the skills required to address these issues are rarely taught in nursing school. Ongoing education and training on inclusivity and practical skills to stop and deflect patients’ racist behaviors should be part of healthcare workers’ orientation and annual competency review.
Policies and procedures for managing a patient refusal of assigned nurses can be developed with input from frontline nurses, and nurse managers should be allies of marginalized groups. A unit practice council can enhance awareness of staff experiences with patient bigotry. Organizations must redouble their commitment to healthy workplace environments. Taking these steps will help ensure the future of nursing is one in which nurses remain advocates of safe patient care, free from prejudice. AN
Gary Sanin Camelo is the patient care director at New York Presbyterian Weill Cornell Hospital in New York City, New York. Fidelindo Lim is a clinical associate professor at New York University Meyers College of Nursing in New York City.
References
American Association of Critical-Care Nurses. Healthy work environments. aacn.org/nursing-excellence/healthy-work-environments
American Nurses Association. Code of Ethics for Nurses with Interpretive Statements. 2015. nursingworld.org/practice-policy/nursing-excellence/ethics/code-of-ethics-for-nurses/coe-view-only
Paul-Emile K, Smith AK, Lo B, Fernández A. Dealing with racist patients. N Engl J Med. 2016;374(8):708-11. doi:10.1056/NEJMp1514939
Sue DW, Alsaidi S, Awad MN, Glaeser E, Calle CZ, Mendez N. Disarming racial microaggressions: Microintervention strategies for targets, White allies, and bystanders. Am Psychol. 2019;74(1):128-42. doi:10.1037/amp0000296
O’Sullivan T, Dodd DR. The impact of EMTALA. In: Schlicher N, Haddock A, eds. Emergency Medicine Advocacy Handbook. 5th ed. Dallas, TX: EMRA; 2019:21-28.
U.S. Equal Employment Opportunity Commission. Title VII of the Civil Rights Act of 1964. eeoc.gov/statutes/title-vii-civil-rights-act-1964
Whitgob EE, Blankenburg RL, Bogetz AL. The discriminatory patient and family: Strategies to address discrimination towards trainees. Acad Med. 2016;91(11):S64-9. doi:10.1097/ACM.0000000000001357

















3 Comments.
Anytime is always a good time to educate the public about the qualification a nurse goes through to be granted the RN designation. When one of my surgical patients said something negative about my being his nurse (I am an immigrant nurse) I called my nurse manager and his surgeon. My nurse manager emphasize the fact that all surgical nurses in our hospital are qualified for their position and that in fact I am one of few who are certified surgical nurse. His surgeon also made him aware that he specifically chose me to be the nurse in most of his surgical cases because I was one of the most experienced and know how to anticipate anything he may need during the surgical procedure. He stress the fact that I can even function as his assistant without a resident physician, that he was lucky to have me. I was grateful for the endorsement and proceeded with his care.
Any job dealing with the “PUBLIC”, U will run into different injustice. These issues have to address for the employee can do their job.
I am curious how this will apply to the vaccination quandry. Does a patient have a right to request the staff caring for them are vaccinated? We have patients avoiding care, screenings d/t perceived risk. As we see the attempt to avoid vaccination hit the courts I wonder how this will affect patients avoidance if the nurses are allowed to decline