
For decades, we’ve known preeclampsia is a high-risk diagnosis with potentially serious consequences for both mother and fetus during pregnancy. Now we know it can have cardiovascular effects on women 20 to 30 years after delivery—effects severe enough to increase the mortality rate in these women. Clearly, preeclampsia is no longer just an obstetrics (OB) concern. Any nurse who works with adult women in their 40s and beyond must become aware of its implications.
Affecting about 5% to 8% of deliveries in the United States, hypertensive disorders of pregnancy are among the three leading causes of maternal death (along with hemorrhage and infection). From 1991 to 1997, preeclampsia caused 16% of 3,201 pregnancy-related deaths. (See Maternal survival after preeclampsia.)
Maternal survival after preeclampsia
This graph shows cumulative estimates of maternal survival after preeclampsia.
“Preeclampsia, later normotensive” denotes women with preeclampsia who had at least one subsequent normotensive pregnancy. “Preeclampsia, later status unknown” refers to all other women with preeclampsia.
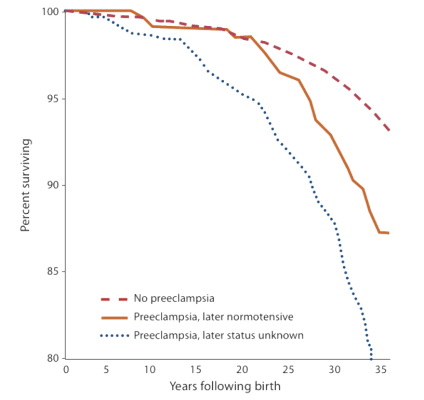
From Funai E, Friedlander Y, Paltiel 0, et al. Long-term mortality after preedampsia. Epidemiology. 2005;16:2()6..21 S. Used with petmission
Pathophysiology
The definitive cause of preeclampsia (formerly called toxemia or pregnancy-induced hypertension) remains unknown. However, the following conditions have been linked to its development:
• first pregnancy (first exposure to placental chorionic villi)
• exposure to unusually high levels of chorionic villi (as in multiple gestations or hydatidiform mole)
• preexisting vascular disease
• genetic predisposition to hypertension during pregnancy.
Besides affecting the placenta, preeclampsia may adversely affect every maternal body system. Fetal outcome depends on disease severity and gestational age at delivery. Fetal effects may include intrauterine growth restriction, preterm birth and its complications, stillbirth, and hypoxia or death secondary to abruptio placentae. The only true resolution of preeclampsia is delivery of the fetus and placenta.
Diagnostic criteria
Preeclampsia occurs when a previously normotensive pregnant woman has a systolic pressure of 140 mm Hg or higher and a diastolic pressure of 90 mm Hg or higher, along with a urine protein level exceeding 300 mg in a 24-hour specimen. Other laboratory findings may include abnormal liver enzyme levels and renal function test results and a low platelet count.In severe preeclampsia, clinical findings also may include oliguria, headache, altered mental status, cerebral and visual changes, right upper-quadrant or epigastric pain, hepatic impairment, thrombocytopenia, and fetal growth restriction. (See Ruling out similar disorders.)
Ruling out similar disorders
For an accurate diagnosis, preeclampsia must be differentiated from several other disorders.
- Chronic hypertension is high blood pressure before pregnancy-or, retrospectively, when blood pressure fails to normalize after delivery. A woman may have undiagnosed hypertension before conception.
- In gestational hypertension, blood pressure rises after the 20th week of gestation but proteinuria is absent.
- Eclampsia is diagnosed when a patient with preeclampsia has seizures that can’t be attributed to other causes. Seizures may occur during the antepartum, intrapartum, or postpartum period.
What about edema?
Edema commonly accompanies preeclampsia and used to be considered part of preeclampsia’s diagnostic triad (along with hypertension and proteinuria). However, in pregnant women with hypertension and proteinuria, preeclampsia now is diagnosed even when edema is absent.
Alarming research findings
Researchers recently have linked preeclampsia to maternal illness and death long after the postpartal period—even in women who regained normal blood pressure after delivery. Although a 1976 study found that a history of preeclampsia didn’t increase the risk of cardiovascular disease (CVD), more recent research shows the disorder does raise the risk of later hypertension, CVD, and death.In a 2005 retrospective study by Funai et al, researchers found that in women who’d regained normal blood pressure after delivery, CVD mortality didn’t rise until 30 to 40 years after the preeclamptic pregnancy. This study divided subjects into three groups:
• group 1: those who hadn’t experienced preeclampsia (35,991 subjects)
• group 2: those who’d experienced preeclampsia but were later normotensive (479 subjects)
• group 3: those who’d experienced preeclampsia with a subsequent pregnancy or who hadn’t had a subsequent pregnancy (591 subjects).
About 2 years after delivery, women in group 3 had a higher cardiovascular mortality—and the rate rose progressively over the years. By 30 years after the preeclamptic pregnancy, it was 9.5%, compared to 3.6% in women who’d never had preeclampsia. Researchers theorize that these women probably developed hypertension at some point after delivery, raising their subsequent CVD risk.
For women in group 2, mortality rates were the same for 20 years after the preeclamptic pregnancy as in women who’d never had preeclampsia. These findings were consistent with previous research, which originally found no increased mortality in women who weren’t hypertensive after their preeclamptic pregnancies. But the new data show that after 30 to 40 years, group 2 mortality paralleled that of group 3. In group 2 women, increased mortality began only after 20 years, and continued for the next 15 years.
What explains the 20-year latency? Researchers speculate that endothelial damage occurring during preeclampsia may promote or hasten vascular disease or trigger a series of events leading to CVD or death. Another theory holds that women at cardiovascular risk also may be at risk for preeclampsia, and that preeclampsia may be an early warning sign of future CVD.
Implications for nursing care
CVD has become the number-one killer of women, and women account for 51% of CVD deaths. Now that preeclampsia has been identified as a CVD risk factor, nurses need to take an active role by identifying at-risk women. Teach preeclamptic patients about their increased risk of future hypertension and its possible consequences. Inform them they’re at higher risk for CVD and increased mortality in their 40s and 50s, whether or not their blood pressure returns to normal after delivery.Even if you work in a non-OB setting, inform any patient with a history of preeclampsia that she’s at high risk for CVD and increased mortality, even if her blood pressure dropped to within normal limits after delivery. Assess her for additional risk factors and urge her to make follow-up appointments for regular assessment. Teach her about signs and symptoms of CVD—especially those specific to women. As appropriate, recommend dietary changes, weight loss or control, exercise, smoking cessation, and stress reduction. Encourage her to get screened for thrombophilia, insulin resistance, hyperlipidemia, and hypercholesterolemia.
To address the CVD risk in all women, healthcare providers must implement cost-effective preventive strategies, including health education and timely assessment. Be aware that the American Heart Association has published evidenced-based guidelines to reduce CVD in women. Become familiar with these—because, as the research shows, preeclampsia isn’t just an OB problem any more.
Selected references
American College of Obstetricians and Gynecologists. Diagnosis and management of preeclampsia and eclampsia. ACOG Practice Bulletin. No. 33, January 9, 2002.
American Heart Association/American Stroke Association. Heart disease and stroke statistics—2006 update. www.americanheart.org/downloadable/heart/1136308648540Statupdate2006.pdf. Accessed December 21, 2007
Berg C, Chang J, Callaghan W. Pregnancy-related mortality in the United States 1991-1997. J Obstet Gynecol. 2003;101:289-296.
Chesley L. Recognition of the long-term sequelae of eclampsia. Am J Obstet Gynecol. 2000;182:249-250.
Funai E, Friedlander Y, Paltiel O, et al. Long-term mortality after preeclampsia. Epidemiology. 2005;16:206-215.

















