
Follow the evidence to improve outcomes.
Takeaways:
- High quality healthcare is established using evidence-based practice in nursing protocols and procedures.
- To decrease pressure injury (PI) rates in long-term care facilities, evidence-based practice should include prevention education, interdisciplinary teams, standardized risk assessments, communication, documentation, and ongoing monitoring.
CNE
1.6 contact Hours
Learning Objectives
- Describe strategies for preventing pressure injuries (PIs) in long-term care (LTC).
- Discuss how to implement a project designed to prevent PIs in LTC.
The author and planners of this CNE activity have disclosed no relevant financial relationships with any commercial companies pertaining to this activity. See the last page of the article to learn how to earn CNE credit.
Expiration: 7/1/24
The Centers for Medicare and Medicaid Services report that pressure injuries (PIs) affect millions of patients each year, with incidence rates ranging from 2.2% to 23.9% in long-term care organizations. PIs occur as a result of intense or prolonged pressure in combination with shear and are affected by excessive heat and moisture, poor nutrition and blood circulation, chronic illness, and soft-tissue conditions (for example, an abrasion or sprain).
For 3 years, PI prevalence increased at a Texas long-term continuing care retirement community that provides independent living, assisted living, memory care, and skilled nursing. The organization faced several challenges, including the lack of a nurse educator and inconsistent continuing education for nursing staff.
To address these challenges, a PI quality improvement team, consisting of the director of nurses, an assistant director of nurses, an RN, a licensed practical nurse (LPN) and a certified nurse assistant (CNA), was created to develop an evidence-based practice (EBP) project of educational interventions and strategies for consistent PI prevention. The project was part of the author’s doctor of nursing practice (DNP) program.
First steps
The QI team started the project by using the PICOT (Patient, population, problem; Intervention; Comparison, control; Outcome, objective; Timeframe) mnemonic to develop this question:
P: In LPNs caring for older adult residents in nursing homes,
I: how will the implementation of a formal PI prevention program
C: compared to no formal program
O: affect PI incidence
T: over a 5-month period?
A systematic literature search was then completed across three databases (PubMed, CINAHL, and Cochrane Library). The search initially yielded more than 65,000 articles, but applying subject headings when possible and reviewing journal titles and abstracts narrowed the results to 51 articles. The inclusion criteria for those articles consisted of participants 18 years of age and older, articles published within 10 years, and those written or translated in English. Exclusion criteria included treatment options such as redistribution devices, wound care products, non-English items, and articles published before 2008. Applying these criteria and removing duplicate articles reduced the number to 20 studies: four Level I studies, four Level IV studies, two Level V studies, seven Level VI studies, and three Level VII studies from around the world. (See Hierarchy of evidence.)
Hierarchy of evidence
Different types of studies provide different levels of evidence.
- Level I—Systematic review or meta-analysis of all relevant randomized controlled trials (RCTs)
- Level II—Well-designed RCTs
- Level III—Well-designed controlled trials without randomization
- Level IV—Well-designed case control and cohort studies
- Level V—Systematic reviews of descriptive and qualitative studies
- Level VI—Single descriptive or qualitative studyLevel VII—Opinions of authorities,
- reports of expert committees
Source Mazurek Melnyk B, Fineout-Overholt E. Evidence-based Practice in Nursing & Healthcare: A Guide to Best Practice. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2018.
On the basis of a study analysis, the team found a body of evidence indicating that formal PI programs with consistent PI prevention education, interdisciplinary techniques, standardized PI risk assessments, increased communication, consistent documentation, and ongoing monitoring can help decrease PI incidence.
Building the project
Building the formal PI program required determining the stakeholders and establishing a timeline.
Stakeholders
Project stakeholders were the facility residents and their families, CNAs, staff RNs and LPNs, nursing administrators, and the organization’s leaders. The EBP project included all residents who were at risk for PIs, and all received prevention strategies.
Timeline
Preliminary discussions began in the fall of 2018 and concluded in the spring of 2019, when the project received approval by the university, the DNP program, and the long-term care organization (the project didn’t require institutional review board approval). By the end of 2019, QI team meetings were planned and support and resources were finalized.
A timeline with evidence-based interventions and outcomes organized, captured, and documented three project implementation phases: educational intervention, implementation, and sustainment and dissemination. Health information collected as part of the project was de-identified.
I used a logic model as the framework for my project. (See Logic model in action.)
Logic model in action
A logic model is a graphic tool for planning, describing, managing, communicating, and evaluating a program or intervention. It consists of two main sections: process (inputs, activities, and outputs) and outcomes (short-, medium-, and long-term goals). Frequently, assumptions and contextual or external factors also are included.
The author used the body of evidence and recommendations in the literature to create the model for the project described in the article. The process section helped guide implementation, and project outcomes were planned, outlined, and appraised throughout. External factors included the time it would take to complete training, and underlying assumptions included awareness of prevention strategies that will decrease PI risk.
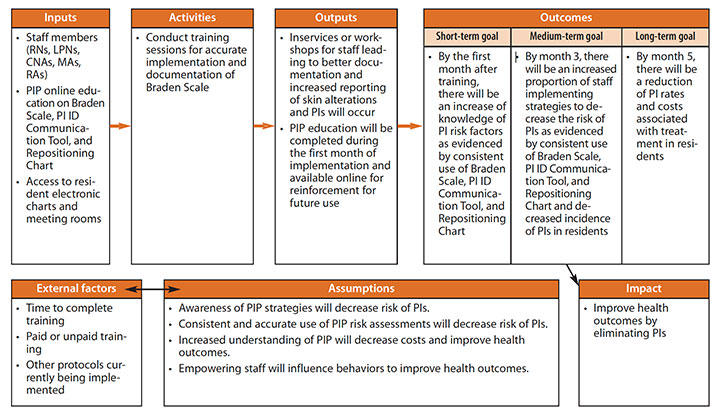
CNAs = certified nursing assistants, ID = identification, LPNs = licensed practical nurse, MAs = medication aids, PI = pressure injury, PIP = pressure injury prevention, RAs = restorative aids
Learn more about logic models at cdc.gov/dhdsp/docs/logic_model.pdf.
Launching the project
The EBP project launched on July 1, 2019, with self-paced online PI education, risk assessments (weekly and Braden Scale assessments), interdisciplinary teamwork strategies, PI prevention strategy communication, and documentation using PI identification communication tools and repositioning charts to increase reporting and encourage ongoing monitoring.
I led four staff development sessions on all shifts to introduce the EBP project to nursing staff. Participants completed a pretest (to gauge current PI knowledge) before the online education program and a post-test after.
Phase 1: Educational intervention
Phase one consisted of implementing three online, self-paced PI education modules from an outside vendor and developing the quality improvement team. The team’s responsibilities included increasing PI prevention communication, promoting an effective multidisciplinary team, discussing goals in staff meetings, monitoring progress, assisting with accurate documentation of PI prevention strategies, and promoting sustainability.
The 20-week nursing staff educational program focused on consistent use of PI risk assessment methods, effective interdisciplinary strategies, increased communication, and accurate documentation of PI prevention strategies. Integrated checklists served as reminders to consistently implement the change based on current protocols. For example, RNs completed monthly comprehensive skin assessments; LPNs completed quarterly and as-needed Braden Scale assessments; RNs and LPNs completed weekly skin assessments; and CNAs, restorative aids, and medication aids completed daily skin assessments during routine care.
Flyers posted in the breakroom, next to the time clock, and behind both nurses’ stations outlined the importance of implementing and documenting PI prevention. (See Promoting PI prevention.)
Promoting PI prevention
As part of the quality improvement team’s efforts to educate nursing staff about pressure injury (PI) prevention, they created a flyer to post throughout the organization. The flyer promoted staff empowerment through education and encouraged the use of a repositioning/skin inspection chart and a PI identification communication tool. At the end of each shift, completed charts and tools are submitted to the assistant director of nursing, who promptly reviews them to identify any new skin issues.
Repositioning/skin inspection chart
When developing the care plan, consider comorbid conditions, such as frailty and dementia.
- Change the patient’s position at least every 2 hours.
- Reposition patients sitting in chairs every hour.
- Inspect skin during activities of daily living.
- Document the patient’s position and skin inspection every shift.
(View a repositioning chart at myamericannurse.com/?p=258423.)
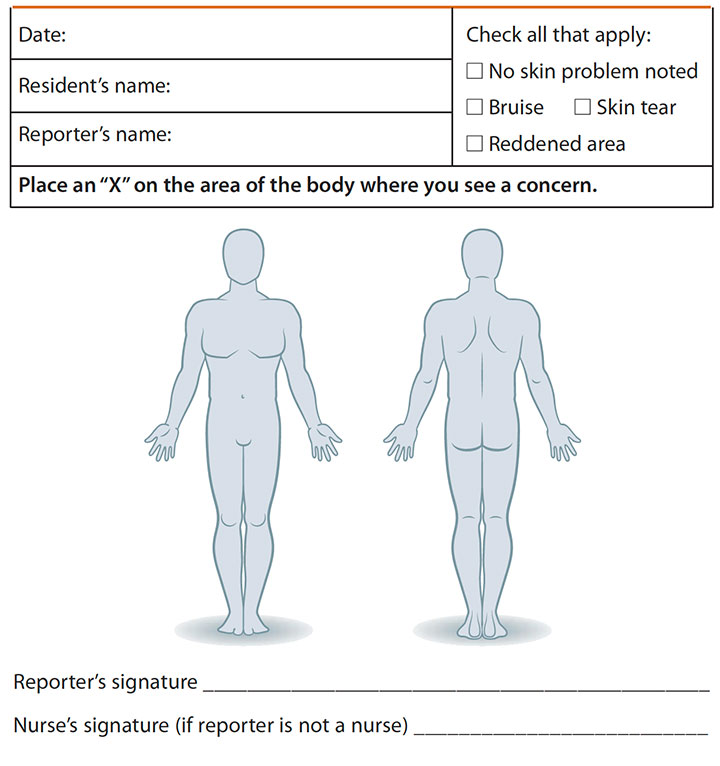
PI identification communication tool
- Complete on all residents daily during routine care every shift.
- If the skin inspection reveals an area of concern, note it on the tool below.
PI identification communication tool
Phase 2: Implementation
Phase two focused on PI prevention strategies, consistent use of the Braden Scale, and weekly skin assessments. Two project implementation forms (a PI identification communication tool and a repositioning chart) previously used within the organization were resurrected for this project. Daily skin checks were documented on the PI identification communication tool, and PI prevention strategies, such as turning residents on a schedule, were documented on repositioning charts.
Phase 3: Sustainment
Phase three consisted of sustaining the prevention strategies, conducting team meetings, developing a skin algorithm, and incorporating project implementation forms into the electronic health record.
Analyzing outcomes
Outcome analysis included educational intervention, PI prevention strategies, PI rates, and cost savings.
Educational intervention
The educational intervention yielded a 57% nursing staff completion rate. Knowledge change was calculated by analyzing staff pretest and post-test scores. In the pretest, 61.5% of nursing staff scored 80 on the PI assessments and 42% scored 100. In the post-test, 13% of staff scored 80 and 87% scored 100 (a more than 50% increase in 100 scores).
PI prevention strategies
In two-thirds of cases where CNAs had documented abnormal skin concerns on the PI identification communication tool, RNs and
LPNs responded by completing multiple Braden Scale assessments, even though there was no formal protocol requiring them to do so. The results confirmed the value of the tool.
Results also indicated the benefits of implementing multicomponent PI prevention initiatives, such as turning, repositioning, and mobilizing frequently, along with other interventions (such as completing the Braden Scale, skin assessments, special mattresses, topical products, heel protectors, pillows, nutritional assessments and interventions, hydration, PI reporting, and communication). Analysis of Braden Scale score averages and repositioning frequency percentages showed that patients with a high-risk Braden Scale score (between 10 and 12) had a 71% repositioning average; moderate risk (13 to 14) had a 59% repositioning average; at risk (15 to 18) had a 66% repositioning average. Inconsistent documentation affected the results, but repositioning averages were at or above 59% consistently.
PI rates
For 3 years, PI incidence rates at the organization had been rising steadily, from 0.67% in 2016 to 2.3% in 2017 and 5.3% in 2018. The national average was 7.2% to 7.3%. The EBP project achieved anticipated decreased PI rates. Between July and December 2019, four Stage II PIs were reported during the intervention (4% PI incidence rate in 2019), resulting in a 25% decrease in PI rates. Based on analysis, more consistent use of the PI identifiction communication tool with appropriate follow-up may have prevented more PIs.
Cost savings
According to the Agency for Healthcare Research and Quality, PIs in the United States cost between $9.1 and $11.6 billion per year. Costs associated with legal action resulting from facility-acquired PIs add to the economic burden. Based on the evidence, the EBP project was expected to reduce PI prevalence by at least 62%. This long-term care organization’s financial policies prohibited the discovery of direct costs, but because PI prevalence decreased by 25% between July and December of 2019, it’s safe to assume some savings occurred. In addition, it’s reasonable to conclude that decreased PI prevalence rates are viewed as desirable by potential residents, which could increase revenue from patient recruitment.
Sustaining the intervention
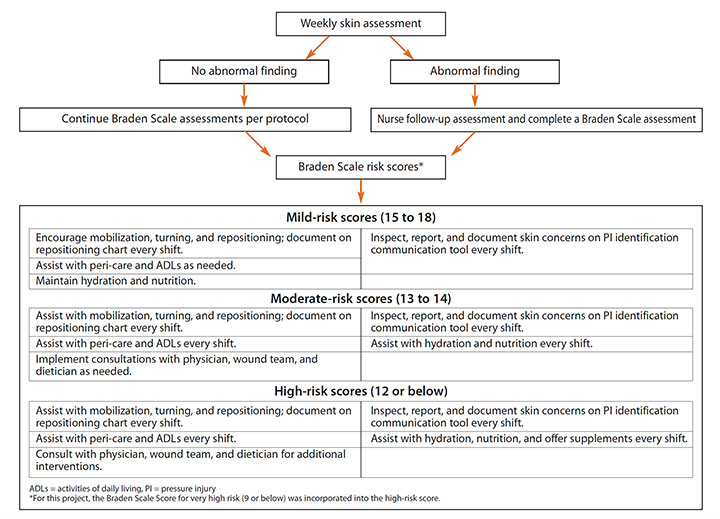
To support sustainability and continued use of evidence for data-driven changes, the QI team developed a skin integrity algorithm. (See Skin integrity algorithm.) The team also recommended to nursing leadership that the organization continue to use Braden Scale and weekly skin assessments. The EBP project prompted a culture change within the organization, enhancing PI awareness and continued use of the implementation forms by nursing staff after the EBP project ended.
Skin integrity algorithm
To ensure the pressure injury (PI) prevention evidence-based practice was sustained, the quality improvement team developed a skin integrity algorithm.
Closing the gap
This EBP project used evidence to close the gap between knowledge and action. Continued efforts include integrating implementation forms and the skin integrity algorithm into electronic formats for permanent use. Other recommendations are incorporating increased EBP into long-term care facilities for better outcomes and to increase the quality of care for all residents.
Melissa De Los Santos is a professor in the vocational nursing program at Austin Community College, Eastview Campus in Austin, Texas.
References
The Agency for Healthcare Research and Quality. Preventing pressure ulcers in hospitals. October 2014. ahrq.gov/professionals/systems/hospital/pressureulcertoolkit/index.html
Ayello EA. Predicting pressure injury risk. try this: Best Practices in Nursing Care to Older Adults. 2017;5.
Beal ME, Smith K. Inpatient pressure ulcer prevalence in an acute care hospital using evidence-based practice. Worldviews on Evid Based Nurs. 2016;13(2):112-7. doi:10.1111/wvn.12145.
Brown TL, Kitterman J. Developing a cost-effective pressure-ulcer prevention program in an acute-care setting. Wound Care Advisor. 2013;2(5)31-4.
Cano A, Anglade D, Stamp H, et al. Improving outcomes by implementing a pressure ulcer prevention program (PUPP): Going beyond the basics. Healthcare. 2015;3(3):574-85. doi:10.3390/healthcare3030574
Cavalcante T, Queiroz A, Carvalho Moura EC, Furtado LB. Updating PF the assistance protocol for pressure ulcer prevention: Evidence-based practice. J Nurs UFPE. 2016;10(suppl 3):1498-506. doi:10.5205/reuol.7057-60979-3-SM-1.1003sup201618
Centers for Medicare & Medicaid Services. MDS 3.0 frequency report. June 6, 2020. cms.gov/Research-Statistics-Data-and-Systems/Computer-Data-and-Systems/Minimum-Data-Set-3-0-Public-Reports/Minimum-Data-Set-3-0-Frequency-Report
Centers for Medicare & Medicaid Services. Nursing Home Data Compendium 2015 Edition.cms.gov/Medicare/Provider-Enrollment-and-Certification/CertificationandComplianc/Downloads/nursinghomedatacompendium_508-2015.pdf
Centers for Medicare & Medicaid Services. Nursing home datasets. 2021. data.medicare.gov/data/nursing-home-compare
Centers for Medicare & Medicaid Services. Quality measures. October 19, 2020. cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/NursingHomeQualityInits/NHQIQualityMeasures
Centers for Medicare & Medicaid Services. Skilled Nursing Facility Quality Reporting Program – Specifications for Percent of Residents or Patients with Pressure Ulcers that Are new or Worsened (NQF #0678). August 2016. cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/NursingHomeQualityInits/Downloads/SNF-QRP-Measure-Specifications_October-2016.pdf
Feng H, Li G, Xu C, Ju C. Educational campaign to increase knowledge of pressure ulcers. Br J Nurs. 2016;25(12):S30-5.
Hanna DR, Paraszczuk A, Duffy M, DiFiore L. Learning about turning: Report of a mailed survey of nurses’ work to reposition patients. MEDSURG Nurs. 2016;25(4):219-23.
Kaur S, Singh A, Tewari MK, Kaur T. Comparison of two intervention strategies on prevention of bedsores among the bedridden patients: A quasi experimental community-based trial. Indian J Palliat Care. 2018;24(1):28-34. doi:10.4103/IJPC.IJPC_60_17
Lima Benevides J, Coutinho JFV, Braga Gomes Tomé MA, et al. Nursing strategies for the prevention of pressure ulcers in intensive therapy: Integrative review. J Nurs UFPE. 2017;11(5):1943-52. doi.10.5205/1981-8963-v11i5a23344p1943-1952-2017
Mallah Z, Nassar N, Kurdahi Badr L. The effectiveness of a pressure ulcer intervention program on the prevalence of hospital acquired pressure ulcers: Controlled before and after study. Appl Nurs Res. 2015;28(2):106-13. doi:10.1016/j.apnr.2014.07.001
Marzurek Melnyk B, Gallagher-Ford L, Fineout-Overholt E. Implementing the Evidence-Based Practice (EBP) Competencies in Healthcare: A Practical Guide for Improving Quality, Safety, and Outcomes. Indianapolis, IN: Sigma Theta Tau International; 2016.
National Pressure Injury Advisory Panel. NPIAP pressure injury stages. 2016. npiap.com/page/PressureInjuryStages
Tayyib N, Coyer F. The effectiveness of pressure ulcer prevention strategies for adult patients in intensive care units: A systematic review. Worldviews Evid Based Nurs. 2016;13(6):432-44. doi:10.1111/wvn.12177
United States Census Bureau. Older people projected to outnumber children for first time in U.S. history. October 8, 2019. census.gov/newsroom/press-releases/2018/cb18-41-population-projections.html
U.S. Bureau of Labor Statistics. Occupational outlook handbook: Licensed practical and licensed vocational nurses. April 9, 2021. www.bls.gov/ooh/healthcare/licensed-practical-and-licensed-vocational-nurses.htm


















1 Comment.
Preparation for implementation of the project seems very thorough.