
A 21-year-old woman arrives for a scheduled annual well-woman exam at the local family planning clinic where you work. She tells you that 2 nights ago, while at a party, she was sexually assaulted by a male acquaintance. The patient does not want to report the assault and declines a forensic examination, but requests that you check just to make sure that she is “OK.”
Survivors of sexual assault present for care in a variety of settings, including emergency departments (EDs), private practices, family planning centers, and urgent care clinics.
Physical assessment of injuries and psychological evaluation of emotional status with appropriate support for identified needs are essential first steps, followed by preventative treatment based on these assessments. This article will focus on preventing pregnancy and sexually transmitted diseases (STDs) in survivors of sexual assault.
Aftermath of sexual assault
Potential exposure to pregnancy and STDs are among the risks of sexual assault. Details of the assault guide the management plan. The health history is key in identifying details and determining preventative treatment.
Recounting details of the assault is an emotionally difficult process for the survivor. An explanation of why particular questions are asked may alleviate some of the discomfort. For example, when asking the survivor to describe the specific body parts and actions involved in the assault, explain that this is done to identify essential areas for assessment during the physical exam. If oral penetration occurred, but not genital or anal contact, the physical exam would then be limited to the oral cavity.
Reporting considerations
The young woman in the scenario above should be told that choosing to undergo a forensic examination won’t obligate her to involve law enforcement. Rather, the evidentiary collection process will preserve evidence should she later decide to pursue legal resolution. She also should be told that reporting the crime to law enforcement officials won’t obligate her to press charges against the perpetrator.
Sexual assaults rarely occur as single, isolated incidents. Often, an individual repeats patterns of behavior associated with the assault. Sharing details of the assault may help law enforcement officials identify patterns that could eventually help apprehend or convict a perpetrator. While survivors should be informed of this information, they should never feel pressured or coerced to undergo unwanted examinations.
Pregnancy prevention
If the health history reveals that the woman may become pregnant as a result of the assault, she should be offered emergency contraception. Existing or previous exposure to pregnancy should be assessed before prophylactic treatment. Previous exposure refers to consensual, unprotected sex within the past 72 to 96 hours. There are survivors who have had consensual, unprotected sex within that time frame and desire pregnancy with their partners. They are not pregnant but the potential for pregnancy exists.
The use of emergency contraception won’t disrupt an established pregnancy, but individuals may decline its use based on the potential for a pre-existing pregnancy. Others may decline emergency contraception because of personal or religious beliefs. As a nurse, you have an obligation to inform survivors of their choices. Equally important is the obligation to respect the choices our patients make.
Pregnancy prevention options
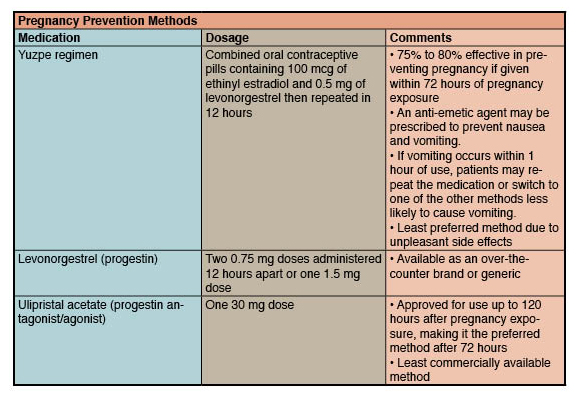
Pregnancy prevention can be provided through three different methods: Yuzpe regimen, levonorgestrel, and ulipristal acetate (UPA). (See Pregnancy prevention methods.) Patients who decline emergency contraception should be advised to take a pregnancy test 2 weeks after the assault.
Prevention of STD
Like the young woman in the introductory scenario, many patients will want to be checked and prophylactically treated for potential exposure to STDs. Some patients will want prophylactic treatment but may be reluctant or unwillingly to either undergo an exam or provide specimens for collection. Reassure patients that this will not preclude preventative treatment.
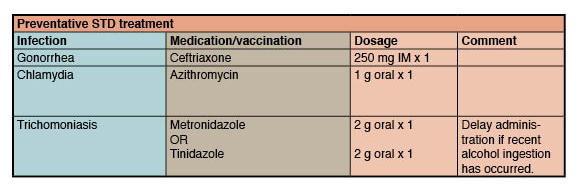
Preventative STD treatment includes ceftriaxone, azithromycin, and either 2 g of metronidazole or a single dose of tinidazole administered orally. This medication regimen provides prophylaxis for gonorrhea, chlamydia, and trichomoniasis exposure respectively. (See Preventative STD treatment.) If preventative treatment is declined, advise patients to return 1 to 2 weeks after the assault for infection screening.
Other STDs that should be addressed after sexual assault include infection with hepatitis B virus (HBV), human papilloma virus (HPV), or human immunodeficiency virus (HIV), although these are less common than infection with the bacterial infections of gonorrhea, chlamydia, and trichomoniasis.
The CDC recommends evaluation of risk status to determine the need for preventative treatment of HIV after a sexual assault. Due to the complexity of clinical management, the CDC advises collaboration with specialists.
Empiric treatment for STD prevention is warranted for all survivors of sexual assault. Whenever possible, use single-dose regimens that can be administered at the point of care because survivors have a low return rate for follow-up visits.
Making a difference
Providing comfort to survivors of sexual assault and ensuring they receive the preventative care they need will help avoid untoward effects of the experience, as well as missed opportunities for care.
Selected references
American College of Obstetricians and Gynecologists. Sexual assault. Committee Opinion No. 592. April 2014. www.acog.org/Resources-And-Publications/Committee-Opinions/Committee-on-Health-Care-for-Underserved-Women/Sexual-Assault.
Centers for Disease Control and Prevention. Sexual assault and abuse and STDs. June 4, 2015. http://www.cdc.gov/std/tg2015/sexual-assault.htm.
Centers for Disease Control and Prevention. U.S. selected practice recommendations for contraceptive use, 2013. June 14, 2013. http://www.cdc.gov/mmwr/pdf/rr/rr62e0614.pdf.
Jatlaoui TC, Riley H, Curtis KM. Safety data for levonorgestrel, ulipristal acetate and Yuzpe regimens for emergency contraception. Contraception. 2016;93(2):93-112.
Moore G. Sexual assault screening in the outpatient setting. Am Nurse Today. 2015;10(8). www.myamericannurse.com/sexual-assault-screening-outpatient-setting/.
Rape, Abuse & Incest National Network. Reporting. https://rainn.org/get-information/legal-information.
Ginny Moore is an assistant professor and WHNP Specialty Director at Vanderbilt University, Nashville, Tennessee.


















{kind=link}
{kind=link}
2 Comments.
Be aware that the decisions a patient makes are their decisions. They have already had enough trauma and have come to receive help not a morals and values experience. Be aware of where you work, the department you work in, and what the practices of that particular facility is with regards to “the morning after” treatments and availability, PLEASE! As a RN with ED experience and one that has been in a similar situation, where another RN asked that I take over care of the patient because the patient choice to receive “the morning after” treatment was a moral decision that the original RN was not comfortable with. This original RN should have asked prior to hire if placed in this situation or any other “moral compromising” position of their own belief system can they check themselves “personally out” when they walk into the ED world so that they can be unbiased in the care they administer to every single patient and their loved ones every time they swipe in as RN? There’s no room for prejudice, biases, or a delay, lack of care or inability to care, especially for those in crisis or in need of emergency care
You probably should address male sexual assault survivors as well. I think we are far enough into this subject nationally to know that women are not the only victims of SA!