
By Patricia C. Dykes, PhD, RN; Jason Adelman, MD; Lesley Adkison, PhD, RN; Michael Bogaisky, MD; Diane L. Carroll, PhD, RN; Eileen Carter, PhD, RN; Megan Duckworth, BA; Lisa Herlihy, MSN; Ann C. Hurley, DNSc, RN; Srijesa Khasnabish, BA; Susan Kurian, RN; Mary Ellen Lindros, PhD, RN;Kristen F.Marsh, MPA, RN; Thanyanee McNinney, BSN, RN; Virginia Ryan, MSN, RN; Maureen Scanlan, MSN, RN; Linda Spivack, PhD, RN; Alexa Shelley, RN, FNP; Shao Ping Yu, MPH
Engage patients and families in a three-step prevention process to reduce the risk of falls.
Takeaways:
- Falls occur in approximately 3% of hospitalized patients and most falls are preventable.
- Falls can be prevented by applying the three-step fall prevention process and universal precautions to all patients.
- Fall prevention “bundles” applied to all patients are ineffective; fall prevention interventions must be tailored to each individual patient’s fall risk factors.
The VIP treatment: A comprehensive post-fall assessment guideline
Autonomy and the patient’s right to choose falls prevention
Assessing your patients’ risk for falling
Ethan Larsen*, age 86, is admitted to the hospital for decompensated heart failure. He lives with his wife in senior housing and has a 3-year history of heart failure,which is treated with captopril and furosemide. He also has a history of type 2 diabetes, which has been controlled with metformin. On admission, Mr. Larsen’s nurse, Virginia (one of the authors of this article) completes a fall risk assessment. Mr. Larsen tells Virginia that he hasn’t had any recent falls, he’s independent at home, and if he has his walker he won’t need help getting to the bathroom in the hospital. Virginia assesses Mr. Larsen’s gait by asking him to walk across the room with his walker. She notes that his gait is unsteady and that he needs to stop several times to catch his breath.
Mr. Larsen’s wife tells Virginia that her husband is very weak and has fallen several times at home in the past month, most recently last night. She says that her husband frequently falls at night when getting up to go to the bathroom.
Based on the admission assessment, Virginia determines that Mr. Larsen is at high risk for physiological falls. In addition to universal fall precautions, which are applied to every patient, Mr. Larsen requires a tailored intervention plan to prevent falls related to his medical condition while he’s in the hospital.
Falls are the most common cause of accidental injury and death in older people. They’re common in hospital settings—about 3% of hospitalized patients fall and about 25% of patients who fall sustain an injury, which can range from minor bruises to serious injuries such as fractures and subdural hematomas.
Fall-related injuries lead to prolonged hospital stays for treatment (on average, 6 to 12 additional days in the hospital), surgery, and sometimes even death. Patients who aren’t physically injured from a fall may develop a fear of falling, leading to decreased mobility and increased fall risk. The risk for falls increases with age, and fall rates are highest on geriatric and geropsychiatric units.
Types of falls
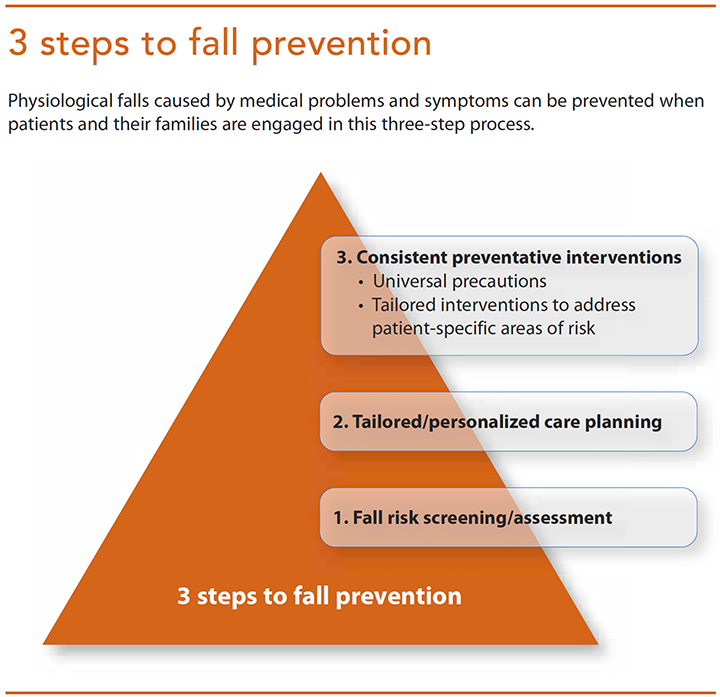
The three falls categories are accidental falls, anticipated physiological falls, and unanticipated physiological falls. Accidental falls are prevented through universal fall precautions that are applied to all patients: keep pathways clear, wipe up spills, make sure patients have access to their call light, and provide ambulatory patients with nonskid footwear. Anticipated physiological falls are caused by underlying medical problems or symptoms. They’re prevented by engaging the patient and family in the three-step fall prevention process. (See 3 steps to fall prevention.) Unanticipated physiological falls are caused by an underlying medical or physiological problem that hasn’t been diagnosed and so isn’t addressed by the fall prevention plan. An ex-ample would be a patient without a history of a seizure disorder who falls after she has her first seizure while walking down the hall with a nurse. Because the patient didn’t have a history of seizures, one could argue that this fall couldn’t have been prevented. However, the seizure disorder is now a known physiological problem in this patient, whose care plan is updated to prevent a similar fall. Any additional falls related to a seizure in this patient would be classified as anticipated physiological falls.
Risk factors
Most patient falls are caused by a combination of factors. The following fall risk factors for hospitalized patients are well established:
- Previous fall history: Patients who have fallen recently are more likely to fall again and under similar circumstances unless the factors that led to the fall are addressed.
- Gait instability and lower-limb weakness: Gait problems and lower-limb weakness can stem from physical illness, deconditioning from periods of inactivity, and age-related changes in gait and balance. Lack of access to walking aids, bedrest, and limited activity during hospitalization can exacerbate these problems.
- Urinary incontinence, frequency, and/or the need for toileting: Medications and V. fluids given during an acute hospitalization can increase urinary urgency and the need for frequent toileting. To avoid incontinence, patients may get up quickly or ambulate without a walking aid/assistance, resulting in a fall.
- Agitation, confusion, or impaired judgment: Patients who are agitated or confused are at risk of falling out of bed or getting up without assistance. However, even patients who are alert and oriented may overestimate their abilities, not realizing that they’re at risk for falls.
- Medications, especially sedative hypnotics: Hospitalized patients often receive medications that may be new or given in addition to the medications they take at home. Medication side effects may cause dizziness, unsteadiness, postural hypotension, and urinary urgency,increasing fall
Risk factors for fall-related injury
Many studies have identified the risk factors for falls in hospitalized patients and many fall prediction screening tools exist. However, relatively few studies have focused on developing tools to identify patients at risk for fall-related injury. Through its national Transforming Care at the Bedside (TCAB) program, which ran from 2003 to 2008, the Robert Wood Johnson Foundation, in collaboration with the Institute for Healthcare Improvement, supported nurses in developing, testing, and implementing changes to improve care on medical-surgical units. Through this effort, the ABCS Fall Injury Risk screening tool was developed to help bedside nurses screen for the following causes of fall-related injury:
- A = Age or frailty: Patients age 85 and older, especially those who are frail, are at increased risk for injury if they fall.
- B = Bones: Patients who have osteoporosis or have had a recent fracture are more likely to sustain a fracture if they fall.
- C = anti-Coagulation: Patients with a bleeding disorder or who are taking anticoagulants are more likely to sustain a bleeding injury if they fall.
- S = Surgery: Patients who have undergone recent surgery (during the current episode of care) are more likely to be injured if they fall.
Evidence-based fall prevention
Research suggests that patient and family engagement in the three-step fall prevention process is critical. Many hospitalized patients fall because they don’t believe that they’re at risk and they don’t follow their fall prevention plan. This is especially true for patients who are independent at home and don’t see themselves as vulnerable to a fall in the hospital. Involving the patient and family in completing the fall risk assessment helps them understand their personal risk factors; including patients in developing a personalized prevention plan makes them more likely to accept and follow it. In addition, informing patients of their risk for injury if they fall increases the likelihood that they’ll follow their plan.
Step 1: Fall risk screening and assessment
Fall risk screening should be done at every patient admission and with each status change, which in acute- care settings may require screening every day or even every shift. The original intent of most screening tools was to predict which patients are likely to fall due to physiological problems or symptoms. However, the tools’ predictive capacity is difficult to measure because once a patient is screened and fall risk factors are identified, not putting preventive interventions in place is unethical. Once interventions are implemented, if the patient doesn’t fall, knowing whether the screening tool was inaccurate or not used correctly, or whether the interventions were effective isn’t clear. The same is true if the patient does fall: Was the screening tool inaccurate or were the interventions ineffective or not followed?
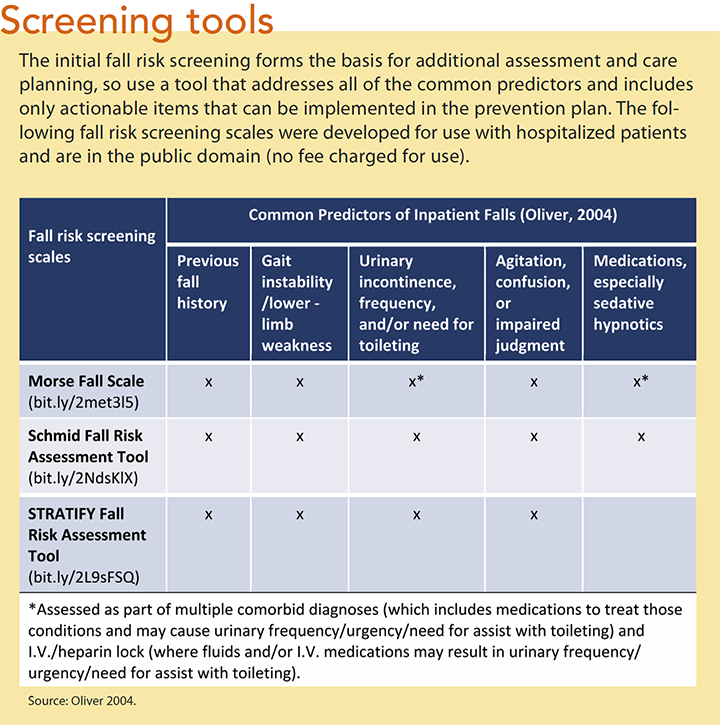
Dr. David Oliver, fall prevention expert and author of the STRATIFY fall risk assessment tool, has suggested that rather than using fall screening tools solely for prediction, they should be used as the basis for additional assessment and proactive fall prevention planning. Used this way, you can complete the screening on admission and then develop the initial fall prevention plan to address each area of identified risk. During the patient’s hospitalization, the nursing assessment is used to continuously refine the plan. Because a fall prevention plan should be implemented as soon as possible after patient ad- mission, a comprehensive risk screening tool that addresses all the common actionable risk factors for falls is needed. (See Screening tools.)
Step 2: Tailored fall prevention care planning
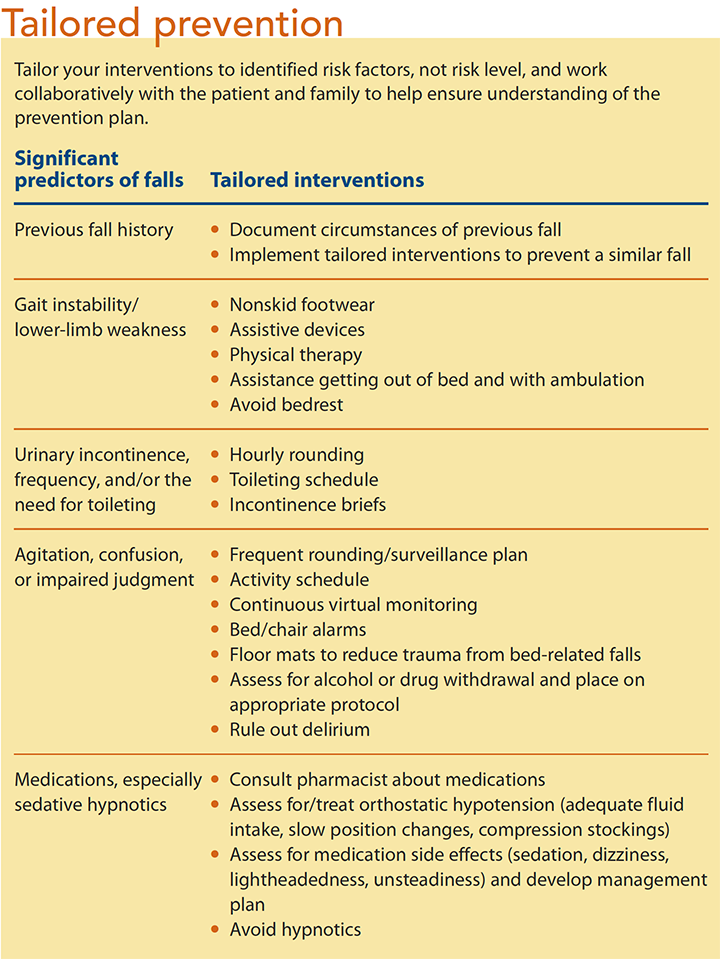
After completing the fall risk screening, collaborate with the patient and family to develop a personalized plan to address each identified risk factor. (See Tailored prevention.) A common mistake is prescribing interventions based on a patient’s level of fall risk (low, medium, or high), rather than tailoring interventions based on patient-specific risk factors. For example, patients who are at risk for falls because of a gait disturbance require different interventions than patients who have a cognitive impairment.
Note that bed and chair alarms should be used only for patients who are confused or who will not reliably call for help. Research indicates that alarms are ineffective at preventing falls in patients who don’t have a positive mental status risk factor and serve only to contribute noise to the environment.
Step 3: Consistently carrying out the fall prevention plan
Consistent implementation of the fall prevention plan requires communicating the patient’s risk factors and plan to the healthcare team (including the patient and family). Direct-care team members, such as nurses and patient care assistants, reinforce the plan with the patient and notify you of any change in the patient’s risk status. You then reassess the patient and update the plan as needed.
Strategies and tools to integrate the patient’s fall prevention plan into the workflow at the bedside improve the likelihood that the plan will be followed. The Fall TIPS (Tailoring Interventions for Patient Safety) Toolkit developed by the Fall TIPS Collaborative can be used to engage patients and family members in the three-step fall prevention process and communicate and reinforce the fall prevention plan at the bedside. (See The Fall TIPS Collaborative.)
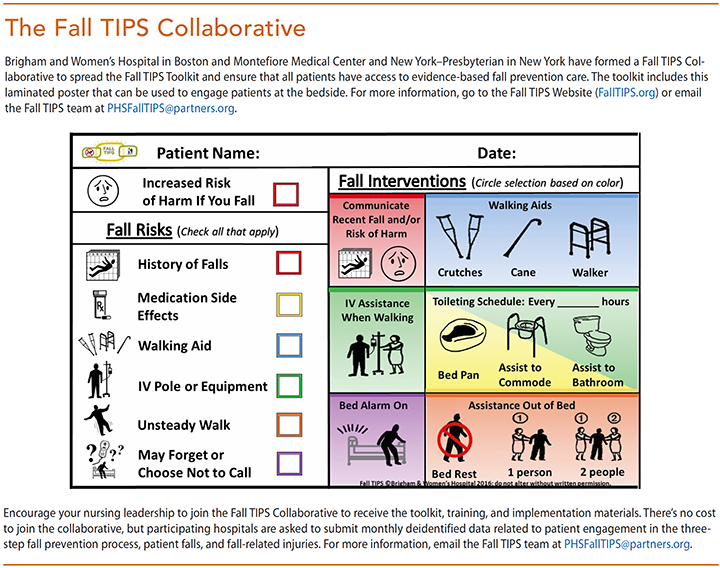
Mr. Larsen is hospitalized at Brigham and Women’s Hospital in Boston, where the Fall TIPS Toolkit is used to engage patients and families in the three-step fall prevention process. While Mrs. Larsen is visiting, Virginia brings the laminated Fall TIPS poster to the bedside. On the left-hand side is the Morse Fall Scale risk assessment translated with icons; on the right are validated interventions, also reinforced with icons. The color provides clinical decision support that links each area of risk to the corresponding evidence-based interventions. While discussing his recent falls with Virginia and his wife, Mr. Larsen says that his legs sometimes get weak when he’s walking to the bathroom at night and then “give out.” Virginia explains that patients who have a history of falls are muchmorelikelyto fall again unless a prevention plan is developed. They agree that Mr. Larsen should call for help to get out of bed and to use the bathroom. They also agree to keep the bed alarm on to remind Mr. Larsen to call before getting up because he overestimates his abilities and will likely not call for assistance.
They also discuss that the furosemide Mr. Larsonis taking for his heart failure will make him urinate frequently. Mr. Larsen and Virginiaagree that she or someone from the team will assist himto the bathroom every hour. Virginia explains to Mr. Larsen that she’s noticed that his walk is unsteady and that he should always use his walker (along with staff assistance) when getting outof bed.
Virginia reinforces Mr. Larsen’s personal fall risk factors and the prevention plan and explains that because of Mr. Larsen’s age he’s at high risk for injury if he does fall.
She then hangs the Fall TIPS Toolkit laminated poster on the wall next to his bed and explains that the poster will remind Mr. Larsen, his family, and all hospital staff about his fall risk factors and his personal fall prevention plan to help ensure that he doesn’t fall while he’s in the hospital.
Nurses’ role in fall prevention
Most nurses routinely complete the fall risk assessment and develop a fall prevention plan for all patients, but engaging patients and families in the three-step process represents a practice change for many nurses. Supporting nurses in this practice change requires education about the evidence behind patient engagement, ongoing monitoring to evaluate the practice change, peer- to-peer feedback and coaching, and leadership backing.
*Patient names are fictitious.
Patricia C. Dykes is a senior nurse scientist and pro- gram director for research at Brigham and Women’s Hospital Center for Patient Safety Research and Practice and an associate professor at Harvard MedicalSchool in Boston. Jason Adelman is the chief patient safety office, associate chief quality officer, and director of patient safety research at New York–Presbyterian Hospital/Columbia University Medical Cen- terin New York. Lesley Adkison is the nursing practice innovation leader at Newton–Wellesley Hospital in Newton, Massachusetts. Michael Bogaisky is a hospitalist, clinical educator, and assistant professor at Montefiore Medical Center in Bronx, New York. Diane L. Carroll is nurse specialist in the Yvonne L. Munn Center for Nursing Research at Massachusetts General Hospital in Boston. Eileen Carter is a nurse researcher at New York–Presbyterian Hospital and assistant professor of nursing at Columbia University Medical Center in NewYork. Megan Duckworth is a research assistantat Brigham and Women’s Hospital. Lisa Herlihy is a senior nurse scientist at Brigham and Women’s Hospital. Ann C.Hurley is a nurse scientist at Brigham and Women’s Hospital. Srijesa Khasnabish is a research assistant Brigham and Women’s Hospital. Susan Kurian is assistant director of nursing quality at Montefiore Medical Center. Mary Ellen Lindros is the director of professional practice and nursing quality officer at Montefiore Medical Center and The University Hospital for the Albert Einstein College of Medicine. Kristen F. Marsh is a patient care director at New York–Presbyterian Medical Center. Thanyanee McNinney is a senior staff nurse at NewYork–Presbyterian Medical Center on the Bone Marrow and Stem Cell Transplant Unit. Virginia Ryan is a clinical nurse at Brigham and Women’s Faulkner Hospital in Boston. Maureen Scanlan is vice president of nursing and patient care services for Montefiore Health System. Linda Spivack is assistant vice president/clinical director of nursing at Montefiore Medical Center. Alexa Shelley is a clinical project coordinator at New York Presbyterian Medical Center. Shao Ping Yu is quality and patient safety project manager at New York–Presbyterian Hospital.
Selected References
Boushon B, Nielsen G, Quigley P, et al. Transforming care at the bedside how-to guide: Reducing patient injuries from falls. Institute for Healthcare Improvement. 2012.
Bouldin EL, Andresen EM, Dunton NE, et al. Falls among adult patients hospitalized in the United States: Prevalence and trends. J Patient Saf. 2013;9(1):13-7.
Carroll DL, Dykes PC, Hurley AC. Patients’ perspectives of falling while in an acute care hospital and suggestions for prevention. Appl Nurs Res. 2010;23(4):238-41.
Chen LH, Warner M, Fingerhut L, Makuc D. Injury episodes and circumstances: National Health Interview Survey, 1997–2007. Vital Health Stat 10. 2009;241:1-55.
Dykes PC. Adding targeted multiple interventions to standard fall prevention interventions reduces falls in an acute care setting. Evid Based Nurs. 2012;15(4):109-10.
Dykes PC, Carroll DL, Hurley A, et al. Fall prevention in acute care hospitals: A randomized trial. JAMA. 2010;304(17):1912-8.
Dykes PC, Carroll DL, Hurley AC, Benoit A, Middleton B. Why do patients in acute care hospitals fall? Can falls be prevented? J Nurs Adm. 2009;39(6):299-304.
Dykes PC, Duckworth M, Cunningham S, et al. Pilot testing Fall TIPS (Tailoring Interventions for Patient Safety): A patient-centered fall prevention toolkit. Jt Comm J Qual Patient Saf. 2017;43(8):403-13.
Dykes PC, I-Ching EH, Soukup JR, Chang F, Lipsitz S. A case control study to improve accuracy of an electronic fall prevention toolkit. AMIA Annu Symp Proc. 2012;2012:170-9.
Evans D, Hodgkinson B, Lambert L, Wood J. Falls risk factors in the hospital setting: A systematic review. Int J Nurs Pract. 2001;7(1):38-45.
Joint Commission Center for Transforming Healthcare®. Facts about the Preventing Falls Project. 2015.
Oliver D, Daly F, Martin FC, McMurdo ME. Risk factors and risk assessment tools for falls in hospital in-patients. A systematic review. Age Ageing. 2004;33(2):122-30.
Shorr RI, Chandler AM, Mion LC, et al. Effects of an intervention to increase bed alarm use to prevent falls in hospitalized patients: A cluster randomized trial. Ann Intern Med. 2012;157(10):692-9.
ant9-CE Fall Tips-822
















3 Comments.
This is a fantastic article with a very thorough review of etiology and prevention of falls in the hospitalized elderly patient. Thank you very much for your hard work and expertise for us and our patients!
Gratefully,
Terri Spencer, MD, MPH
Excellent evidence-based content. Suitable for my quality improvement work. Thanks.
Have completed the test. Excellent material, appropriate to content.