
Identify frequently unrecognized injuries.
- No standardized post-fall assessment exists for long-term care facilities, which leads to inefficiency and inaccuracy.
- A possible factor in inaccurate assessments may be a focus on external signs of trauma.
- This organization identified the issue and took steps to address it by creating a detailed post-fall assessment tool.
Falls, a prevalent health issue among older adults, are associated with high morbidity and mortality rates. In 2018, according to the Centers for Disease Control and Prevention (CDC), over 36 million falls occurred in the older adult population. Coutinho and colleagues found a 1-year cumulative mortality rate of 25% for individuals who sustained a serious injury from a fall. With the older adult population growth rate projected to increase significantly within the next decade, the CDC estimates that approximately 52 million falls will occur in 2030. To ensure appropriate care, nurses must perform accurate post-fall assessments to prevent complications in all settings, including in long-term care facilities (LTCFs).
Ineffective assessment and training
No readily available standardized post-fall assessment approach exists for LTCFs, and actual practices vary. This variance creates a wide spectrum of efficiency and accuracy in assessment results. A study by Chan and colleagues found that nurses may perform inadequate assessments in facilities where they don’t receive specific training.
Preventing falls in long-term care facilities
Even when a facility has well-established post-fall assessment policies, adherence may be poor. In an audit performed at the Royal Gwent Hospital in Newport, UK, Ali and colleagues found that 21% of patients who had experienced a fall hadn’t received a documented clinical assessment; of the patients who did, only 28% had an accurately documented 24-hour neurologic observation period. One might assume that most of the healthcare providers underperforming in clinical post-fall assessments are young and inexperienced. However, Baixinho and dos Anjos Dixe found no significant statistical difference between the provider’s age and length of clinical experience associated with post-fall incidence practices and behaviors.
One possible factor contributing to inaccurate physical assessments of older adults is a focus on external signs of trauma. Foster and colleagues concluded that external signs alone are insufficient for diagnosing significant findings of trauma in older adults who experience a ground-level fall. (See About ground-level falls.)
As awareness of the importance of accurate post-fall assessments continues to grow, many researchers have conducted studies to determine the effectiveness of post-fall assessment training to improve accuracy. Multiple studies indicate that implementing standardized protocols to assess older adults who have fallen aids training. Arendts and colleagues found that, after a hospital implemented a 12-month intervention using a standardized approach to post-fall assessments among patients arriving to the emergency department (ED) after a fall, the discharge rate increased from a 46% to 66% baseline for the 1,435 older adults involved in the study. In addition, the median length of hospital stay for patients who’d experienced a fall decreased from 6 days pre-intervention to 2 days post-intervention. These improvements were substantial, especially considering the relative ease and cost-efficiency of this strategy. Similar results have been obtained using this method in other facilities.
Although Arendts and colleagues specifically evaluated patients in the ED, a more formal and thorough evaluation of patients in LTCFs may result in better outcomes and earlier detection of significant injuries. For example, in the study by Ali and colleagues, after the hospital introduced a post-fall protocol, accurate assessments increased from 28% to 52%. These studies indicate that staff training may be an effective tool to reduce the incidence of inaccurate post-fall assessments, thereby decreasing the risk of missing potentially fatal injuries.
Need identified
The idea to pursue improvement in post-fall assessments at our hospital occurred following a sentinel case in which a nursing professor was with students at an LTCF about 24 hours after one of the residents had fallen. The professor noticed a significant change in the resident and asked what had occurred. He was told the patient had fallen the day before and had been placed on oxygen. When the professor asked what kind of injury assessment had been done, he learned that, although the patient had fallen onto the corner of a bedside table and experienced significant chest pain, no labs or physical exam had been documented and no x-rays had been ordered. When the patient experienced difficulty breathing, the provider ordered oxygen, but no other assessments had been completed.
After observing the post-fall events in this circumstance, it became evident that patients would benefit from a more streamlined assessment process. The professor determined that developing a post-fall assessment for patients in the LTCF would be a worthwhile project to undertake with undergraduate baccalaureate nursing students. In addition to two students, he invited another nursing faculty member to participate in the project. (See Research and nursing students.)
Literature review
During a literature review focused on existing post-fall assessment protocols, we identified two approaches. The first, in 2008 by Fenton, focused on the evaluation of older adults living in community rehabilitation hospitals in Europe. This approach included a post-fall assessment algorithm focused on evaluating for possible bleeding and injuries of the head, neck, trunk, and extremities. It used the mnemonic “Assess, Look, and Feel” to guide staff.
The second assessment, published by the Agency for Healthcare Research and Quality (AHRQ), focused on evaluating the patient’s airway, breathing, and circulation, as well as the head and neck after a ground-level fall. If head and neck injuries are ruled out, providers move to checking vital signs, providing wound and pain management, informing the medical provider, and performing additional tests, such as labs and x-rays. If a concern for head or neck injuries exists, the patient is immobilized and the provider is contacted immediately.
We also reviewed the Advanced Trauma Life Support (ATLS) algorithm developed by the American College of Surgeons Committee on Trauma. This algorithm, considered the gold standard of trauma care throughout the United States, provides a consistent approach to evaluating and managing trauma victims.
VIP treatment
We determined that ATLS provided the best approach for falls in LTCFs. One of the nursing faculty on the team had extensive experience using ATLS when he worked as a nurse practitioner in a Level 1 trauma center. With his help, we created a flowchart to provide a standardized protocol for post-fall assessments using ATLS methods, which teaches a systematic, concise approach to caring for trauma patients. We streamlined the algorithm to fit the skill levels of licensed practical nurses and RNs working in LTCFs. We called the new approach the VIP Treatment (Visualize, Palpate for Injuries, Proceed with Care).
To aid instruction and implementation, we developed teaching materials, which included a PowerPoint presentation, an instructional training video, a flowchart outlining the assessment steps, a head-to-toe assessment checklist, scheduled recheck guidelines, and a documentation guide. We hired a professional actor to make the training video as realistic as possible.
Visualize
The algorithm guides the nurse through the visualization process by asking questions such as, “Is the patient conscious?” and “Does the patient have noticeable bleeding?” The head-to-toe assessment prompts the nurse to look for visible bleeding or bruising of the head, neck, and abdomen, as well as any obvious musculoskeletal deformities and skin tears. Based on the assessment, the nurse either calls 911 or continues with the evaluation. This step-by-step process prevents any delay in treating serious injuries and provides the nurse with a prioritization framework. (See Give them the VIP treatment.)
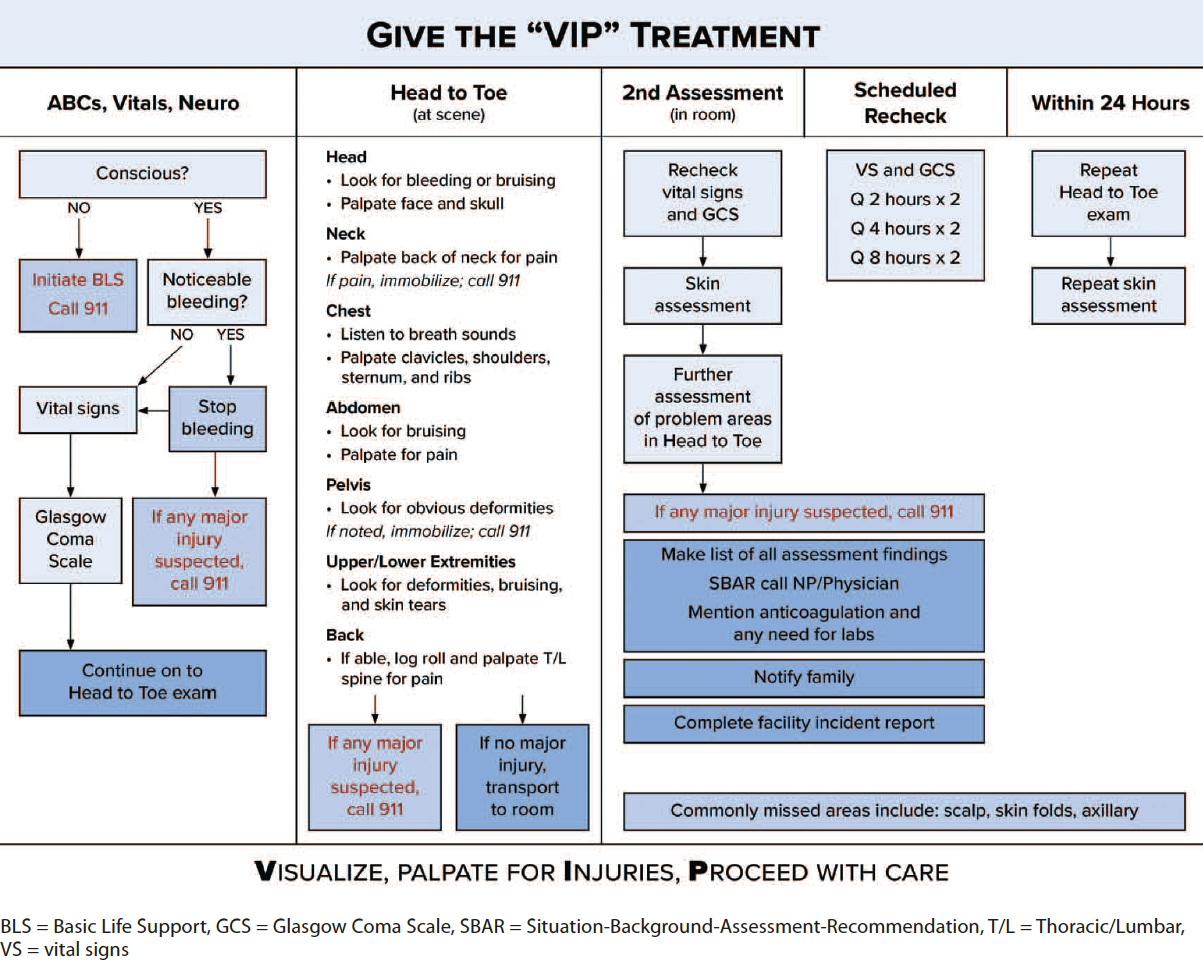
Palpate for injuries
Palpation aids identification of frequently missed internal injuries, which may prove fatal if not treated promptly. Similar to the initial assessment, the process moves from head to toe to ensure proper evaluation of the entire patient. For example, if the patient feels neck pain with palpation, the nurse immobilizes the patient and calls 911. This step-by-step process addresses the patient’s most important needs and avoids any further assessment that may cause additional harm.
Proceed with care
In some cases, the nurse may have difficulty determining if they should advance in a patient’s assessment or stop and call for help. The carefully prescribed actions in the “Proceed with care” step are integrated throughout the assessment process; as the nurse completes one as-sessment item, they’re prompted to use critical thinking skills and guided in evaluating the saf-est next step.
If the nurse determines that the patient isn’t in immediate danger from a finding, they’re prompted to proceed with care to the next assessment step. After addressing areas where ob-vious injuries may be suspected, the nurse assesses the patient’s vital signs and neurologic status using the Glasgow Coma Scale (GCS). At any point in the assessment, findings may prompt the nurse to stop and call 911.
This VIP process is repeated in a second head-to-toe assessment and in subsequently scheduled rechecks. After another check of the patient’s vital signs and a GCS, the nurse conducts a thorough skin assessment to identify any signs of wounds, bruising, or skin tears. If the nurse identifies any major injuries, they call 911. The nurse then makes a list of the findings and calls the patient’s primary care provider using the SBAR (Situation-Background-Assessment-Recommendation) format. Next, the nurse notifies the patient’s family of the fall and current condition and completes the facility’s incident report paperwork.
The nurse rechecks the patient’s vital signs and the GCS every 2 hours twice, every 4 hours twice, and every 8 hours twice. Within the first 24 hours, the nurse repeats the head-to-toe exam and skin assessment. This marks the completion of the VIP Treatment protocol. The nurse then thoroughly and accurately documents the post-fall assessment using provided forms.
Spreading the word
We believe that many older adults could benefit from treatment facilities implementing the VIP Treatment protocol. Before the COVID-19 pandemic, our research team began contacting local LTCFs to present our research and teaching materials. At one facility, the team met with the care coordination team and director of nursing to discuss the prospect of implementing the protocol.
The information was well-received and we had planned to hold a follow-up meeting, but the process was cut short by the shutdown of our university and the LTCFs in our area during the pandemic. With the improving conditions, we hope to continue contacting facilities to implement our research and gather data on its effectiveness.
Simple and effective
The VIP Treatment protocol provides a simple and effective process to address the growing concern of unidentified injury after a fall. In addition, developing and implementing this protocol has provided a valuable learning opportunity for undergraduate nursing students. As nursing faculty within university settings seek to improve the discipline through their research, including undergraduate nursing students in these projects may prove beneficial and significant to their nursing education and careers.
The authors work at Brigham Young University in Provo, Utah. Blaine A. Winters is an associate professor. Tracy Dustin is an assistant professor. Abigail Fife and Allison Christenson are student nurses.
American Nurse Journal. 2023; 18(3). Doi: 10.51256/ANJ032342
Key words: Post-fall assessment, ground-level falls, injuries, older adults, elderly, long-term care
References
Agency for Healthcare Research and Quality. Preventing falls in hospitals: Tool 3N: Postfall assessment, clinical review. January 2013. ahrq.gov/patient-safety/settings/hospital/fall-prevention/toolkit/postfall-assessment.html
Ali M, Marsh R, Beasant E. Quality improvement project to standardise the immediate assessment of inpatients who fall within the Royal Gwent Hospital. Age Ageing. 2019;
48(Suppl 2):ii1-10. doi:10.1093/ageing/afz055.31
American College of Surgeons. Advanced trauma life support. facs.org/quality-programs/trauma/atls
Arendts G, Leyte N, Dumas S, et al. Efficiency gains from a standardised approach to older people presenting to the emergency department after a fall. Aust Health Rev. 2020;
44(4):576-81. doi:10.1071/AH19187
Baixinho CL, dos Anjos Dixe M. dos A. Practices and behaviors of professionals after falls in institutionalized elderly with and without cognitive decline. Dement Neuropsychol. 2020;14(1):62-8. doi:10.1590/1980-57642020dn14-010010
Centers for Disease Control and Prevention. Keep on your feet—Preventing older adult falls. December 16, 2020. cdc.gov/injury/features/older-adult-falls/index.html
Chan M, Tan CW, Mathew P. 60 Post Inpatient Fall Medical Assessment (PIFMA) performa quality improvement project. Age Ageing. 2020;49(Suppl 1):i18-20. doi:10.1093/ageing/afz187.01
Coutinho ESF, Bloch KV, Coeli CM. One-year mortality among elderly people after hospitalization due to fall-related fractures: Comparison with a control group of matched elderly. Cad Saúde Pública. 2012;28(4):801-5. doi:10.1590/S0102-311X2012000400019
Fenton W. Introducing a post-fall assessment algorithm into a community rehabilitation hospital for older adults. Nurs Older People. 2008:20(10):36-9. doi:10.7748/nop2008.10.36.c6870.
Foster SM, Muller A, Jones P, et al. External signs of trauma: A poor predictor of injury in found down and ground level falls. Am J Surg. 2020;220(5):1300-3. doi:10.1016/
j.amjsurg.2020.06.046
Khurrum M, Chehab M, Ditillo M, et al. Trends in geriatric ground-level falls: Report from the National Trauma Data Bank. J Surg Res. 2021;266:261-8. doi:10.1016/j.jss.2021.02.047


















