Lack of treatment response requires additional investigation.
Takeaways:
- Older adults seen by primary care nurse practitioners may have vague, atypical signs and symptoms.
- Looking beyond the obvious diagnosis when a patient doesn’t have the expected response to treatment may enhance positive outcomes.
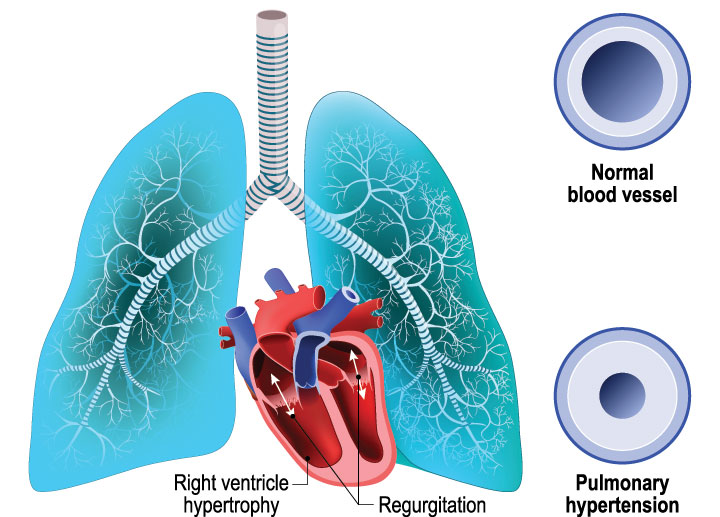
Older adults seen by primary care nurse practitioners (NPs) may have vague, atypical signs and symptoms. Looking beyond the obvious diagnosis (sometimes hoofbeats are zebras and not horses) when a patient doesn’t have the expected response to treatment may enhance positive outcomes. For example, shortness of breath, a common complaint, has many possible etiologies, including pulmonary hypertension. (See Uncovering an unexpected diagnosis.)
Uncovering an unexpected diagnosis
Isolated wheezing can be attributed to a reduction in airflow due to fluid, a space-occupying mass, or an airway constriction. Adventitious sounds (for example, fine and coarse crackles) that accompany wheezes may suggest conditions such as pulmonary edema, pulmonary fibrosis, pneumonia, heart failure, and late-onset asthma. Pulmonary hypertension, which typically isn’t on the list of differential diagnoses at symptom onset, shouldn’t be forgotten when a patient has predisposing conditions and doesn’t improve with standard care. Poor treatment response indicates the need for further investigation.
For instance, a critical component of quality healthcare for older adults includes a thorough reconciliation of all prescribed and over-the-counter medications and supplements. However, asking the patient how they take the medication can reveal opportunities for intervention and education. If used as a standard of best practice, medication reconciliation can yield information about possible adverse effects, contraindications, and psychosocial barriers to optimal care. In addition, asking about activities of daily living and functional limitations when bending down to retrieve objects from the floor or squatting to tie shoes may indicate hemodynamic changes suggestive of increased pulmonary vascular resistance.
This case study describes a clinical encounter with an older adult who presented with long-standing dyspnea, poor response to treatment, and the need for home oxygen. Poor treatment response and interview answers reveal possible missed opportunities for improved quality of life and care management.
Case report
Ms. Mary Hawthorne*, a 93-year-old white woman, returns with her daughter (her primary caregiver) to an academic outpatient geriatric primary care clinic for a 2-week follow-up related to chronic obstructive pulmonary disease (COPD). Ms. Hawthorne reports a poor response to nebulized ipratropium/albuterol prescribed at her pervious visit. She experiences daily symptoms that interfere with function, activities of daily living, and quality of life. Ms. Hawthorne continues to have shortness of breath and wheezing without relief from the appropriate use of medications. Her daughter believes her mother needs oxygen therapy.
Patient history
In addition to COPD, Ms. Hawthorne’s medical history includes coronary artery disease, heart failure (HF) with preserved ejection fraction, diverticulitis, esophageal hiatal hernia, gastroesophageal reflux disease, hemorrhoids, hypertension, osteoarthritis, and pseudogout of the knee. Her most recent hospitalization was 1 year ago for HF exacerbation and a transthoracic echocardiogram. Surgical and family history are noncontributory.
Ms. Hawthorne’s social history updates reveal exposure to secondhand smoke in the remote past but no inhaled tobacco or chemical products. She lives with her daughter, who’s closely involved with her mother’s care. A review of documented past discussions and goals of care indicate that Ms. Hawthorne and her daughter consistently defer discussion of palliative treatment and advanced directives because of a perceived independent level of function.
A review of echocardiogram findings in the patient’s medical record indicates mildly dilated left and right atriums; mild-to-moderate aortic sclerosis; mild-to-moderate tricuspid, mitral, aortic, and pulmonic valve regurgitation; an estimated right ventricular systolic pressure (RVSP) of 55 to 60 mmHg (>40 mmHg in older adults suggests pulmonary hypertension), and a normal left ventricular ejection fraction of 65% to 70%.
Ms. Hawthorne’s current medications include amlodipine 10 mg daily, aspirin 81 mg daily, citalopram 30 mg daily, diclofenac sodium gel 1% as needed, doxepin 50 mg every night, inhaled fluticasone propionate-salmeterol 250/50 mcg twice daily, furosemide 160 mg daily, gabapentin 100 mg daily, hydrocodone–acetaminophen 5/325 mg every 6 hours as needed, inhaled ipratropium–albuterol 0.5 mg/2.5 mg/3 mL lidocaine patch 4% daily, loratadine 10 mg daily, losartan 50 mg daily, montelukast 10 mg daily, omeprazole 20 mg daily, and simvastatin 20 mg daily.
Pertinent positive findings for the review of systems (ROS) include ongoing shortness of breath on exertion, audible wheezing, persistent bilateral lower extremity edema that’s worse in the afternoons, and a nonpruritic petechial rash on the patient’s legs. Ms. Hawthorne’s weight is stable and she reports no cough, heartburn, nausea, chest pain, paroxysmal nocturnal dyspnea, and orthopnea.
Clinical exam
Ms. Hawthorne has no apparent distress, is oriented, well-groomed, and well-nourished. Her vital signs are oral temperature 97.6° F (35.9° C), heart rate 70 beats per minute, blood pressure 119/65 mmHg, respiratory rate 18 breaths per minute, oxygen saturation 87% (on room air) when at rest and when walking, weight 74 kg, and body mass index 33. The physical exam reveals an established II/VI systolic murmur in the aortic area, rales in the bilateral posterior lungs, expiratory wheezes, no increase in respiratory effort, no evidence of consolidation with percussion of posterior lung fields, and 2+ bilateral lower extremity edema (reported as worse) extending to the knees. Ms. Hawthorne’s knee-high hosiery has a constricting top band.
Diagnostics
The patient’s chest x-ray shows right ventricular hypertrophy and enlargement of the central pulmonary arteries. Electrolytes, renal function, and fluid volume status results include sodium 142 mEq/L, potassium 4.7 mEq/L, chloride 106 mEq/L, carbon dioxide 31 mEq/L, glucose 127 mg/dL, blood urea nitrogen 21 mg/dL, creatinine 1.22 mg/dL, estimated glomerular filtration rate 50 mL/min/1.732, brain natriuretic peptide 118 pg/mL, and thyroid stimulating hormone 3.7 mU/L. A 5-minute walk test shows an oxygen saturation of 96% on 2L/min of oxygen via nasal cannula with only mild dyspnea. The patient’s history, poor response to treatment, shortness of breath, results of the walk-test, and lab work collectively support the reconsideration of pulmonary hypertension as a primary diagnosis.
Plan of care
Given Ms. Hawthorne’s dyspnea and objective assessment findings, the NP changes furosemide to bumetanide 1 mg twice daily for palliative management of dyspnea and worsening edema. The patient’s poor prognosis, the current plan of care, and echocardiogram findings indicate the need for referral to pulmonology for further evaluation and possible management of primary pulmonary hypertension. The NP initiates continuous home oxygen therapy at 2 L/min per nasal cannula.
At the 2-week follow-up visit, Ms. Hawthorne reports improved dyspnea and exertional fatigue. Her daughter shares that the pulmonologist advised against treatment because of the patient’s advanced age and comorbid conditions. Ms. Hawthorne and her daughter are now ready to discuss goals of care and advance directives. Based on their care goals, the NP completes a do-not-resuscitate order and an anticipatory plan using the Medical Order for Scope of Treatment to document the patient’s expressed wishes for her preferred setting, timing, and treatment. The NP orders a hospice evaluation.
Investigate to gain clarity
When a patient’s response to treatment is less optimal than expected, NPs should explore other differential diagnoses and causes to explain persistent symptoms. In this case, in-depth interviewing and a review of the medical record revealed findings indicative of pulmonary hypertension. This chronic, progressive disease has multiple etiologies, including pulmonary, cardiac, and nonthoracic conditions. If invasive diagnostic procedures are congruent with the patient’s goals of care and prognosis, pulmonary hypertension can be confirmed via cardiac catheterization. In patients with comorbidities, shortness of breath and wheezing may be misdiagnosed. A chest x-ray may show a narrowing of the pulmonary arteries and bilateral hilar and ventricular enlargement that indicate further investigation. If congruent with risk/benefit analysis and the patient’s care goals, cardiac catheterization may be considered for definitive diagnosis. (See Pulmonary hypertension facts.)
Pulmonary hypertension facts
Pulmonary hypertension is commonly misdiagnosed and underrecognized. The more you know about the condition, the more likely you are to identify it early.
- The World Health Organization recognizes five groups of pulmonary hypertension, categorized by pathogenesis or comorbidity:
- pulmonary arterial hypertension
- left-heart disease
- lung disease and hypoxia
- chronic thromboembolic disease
- miscellaneous.
- Symptoms include those congruent with underlying pulmonary or right or left heart failure or hypertrophic cardiomyopathy.
- Right heart failure is a prognostic indicator of end-stage disease.
- Extensive remodeling of the pulmonary circulation affects distal pulmonary circulation.
- Prevalence is increasing in older adults, with the most common causes in Groups 2 and 3.
- Early treatment can reduce symptoms and improve quality of life.
- This progressive condition has a high mortality rate in 1 year.
This case highlights the incongruencies that can occur among the medical record, treatment plan, and patient presentation. Investigating to gain clarity requires time that busy primary care practices may have difficulty accommodating, but taking an extra 15 minutes to review the medical record may make a difference in a patient’s life and care management. In addition, palliative management, which is appropriate across the spectrum of chronic disease, frequently is misunderstood by patients and families. Discussing this management model early can improve a patient’s symptom burden and quality of life.
The authors work at the University of Louisville School of Nursing in Louisville, Kentucky. Candace C. Harrington is an assistant professor and a gerontology nurse practitioner professor. Lynn P. Roser is an assistant professor.
*Name is fictitious.
References:
Dunlap B, Weyer G. Pulmonary hypertension: Diagnosis and treatment. Am Fam Physician. 2016;94(6):463-9.
Gerges M, Gerges C, Pistritto AM, et al. Pulmonary hypertension in heart failure: Epidemiology, right ventricular function, and survival. Am J Respir Crit Care Med. 2015;192(10):1234-46. doi:10.1164/room.201503-0529OC
Ginoux M, Turquier S, Chebib N, et al. Impact of comorbidities and delay in diagnosis in elderly patients with pulmonary hypertension. ERJ Open Res. 2018;4(4):00100-2018. doi:10.1183/23120541.00100-2018
Harrington CC. Heart failure. In: Kennedy-Malone L, Martin-Plank L, Duffy EG, eds. Advanced Practice Nursing in the Care of Older Adults. 2nd ed. Philadelphia: FA Davis; 2018; 152-214.
Jones S. Pulmonary hypertension patient navigation: Avoiding the perfect storm. Adv Pulm Hypertens. 2016;15(1):32-5. doi:10.21693/1933-088X.15.1.32
Klinger JR, Elliott CG, Levine DJ, et al. Therapy for pulmonary arterial hypertension in adults: Update of the CHEST guideline and expert panel report. Chest. 2019;155(3):P565-86. doi:10.1016/j.chest.2018.11.030
Park MH. Management of pulmonary hypertension. Cardiology Advisor. 2017.
Reuben DB, Herr KA, Pacala JT, Pollock, BG, Potter JF, Semla TP. Geriatrics at Your Fingertips 22nd ed. Washington, DC: American Geriatrics Society; 2020.
Stein PD, Matta F, Hughes PG. Scope of problem of pulmonary arterial hypertension. Am J Med. 2015;128(8):844-5. doi:10.1016/j.amjmed.2015.03.007
Stewart T, Burks M, Nolley SH, et al. Collaborative care: A defining characteristic for a pulmonary hypertension center. Pulm Ther. 2017;3:93-111. doi:10.1007/s41030-017-0039-1
Wijeratne DT, Lajkosz K, Brogly SB, et al. Increasing incidence and prevalence of World Health Organization groups 1 to 4 pulmonary hypertension: A population-based cohort study in Ontario, Canada. Circ Cardiovasc Qual Outcomes. 2018;11(2)e003973. doi:10.116/CIRCOUTCOMES.117.003973

















