A life-threatening, life-altering emergency, sepsis can have catastrophic effects. When the condition progresses undetected, it can lead to multiple organ dysfunction syndrome and death. Mortality ranges from 9% to 35% and rises sharply with each passing hour that sepsis goes unidentified.
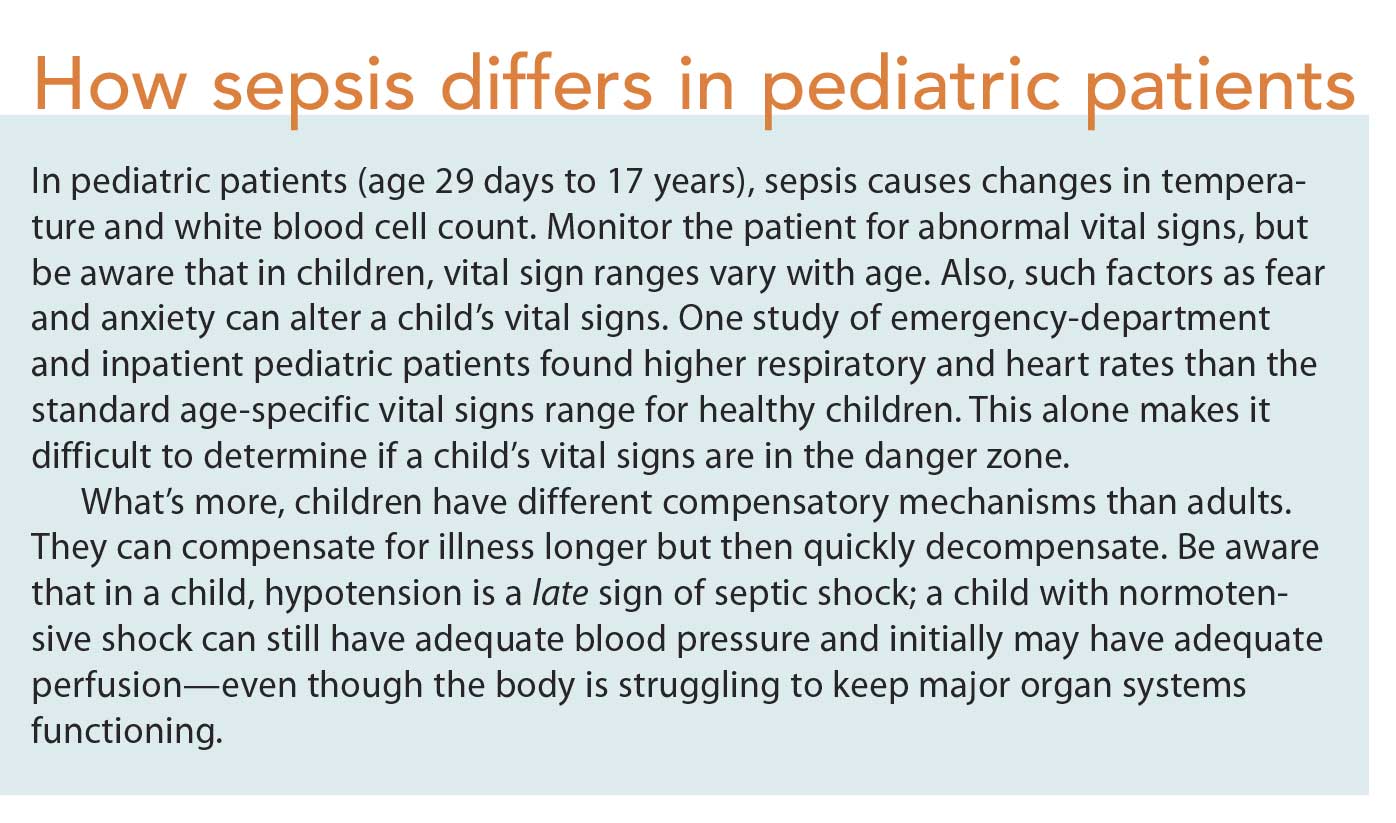
In the United States alone, an estimated 20,000 to 40,000 children are diagnosed with septic shock annually—and the number is increasing. Prompt recognition and treatment can improve survival odds. Unfortunately, sepsis is harder to recognize in children than adults. (See How sepsis differs in pediatric patients.) Although most children with sepsis don’t arrive at the hospital in full septic shock, they can deteriorate quickly as the condition progresses.
Sepsis can develop in both the community and the hospital. So all nurses—not just those working in emergency departments, intensive care units, and transport teams—must know how to assess for and identify early warning signs of sepsis in children.
Sepsis terminology update
In 2016, a task force of the Society of Critical Care Medicine and the European Society of Intensive Care Medicine issued new consensus definitions and criteria (called Sepsis-3) for sepsis and septic shock. Sepsis-3 updated the terminology for sepsis and related conditions and moved away from the model of sepsis as a continuum. It defines sepsis as a life-threatening organ dysfunction caused by a dysregulated host response to infection and defines septic shock as a subset of sepsis with profound circulatory, cellular, and metabolic dysfunction linked to a higher mortality risk than sepsis alone.
In addition, Sepsis-3 concluded that criteria for systemic inflammatory response system (SIRS) lack the sensitivity and specificity to detect sepsis in its early stages. (None theless, the SIRS criteria may still be useful in helping clinicians determine if the patient has an ongoing infectious process.) Sepsis-3 recommends use of a secondary screening tool, the quick Sepsis-Related Organ Failure Assessment (qSOFA), in patients with an identified or suspected infection to evaluate risk for clinical deterioration. In adults, two of three qSOFA elements—altered mental status, respiratory rate of 22 breaths/minute or higher, or systolic pressure of 100mm Hg or lower—predict poor clinical odds. These patients should be evaluated for possible organ dysfunction.
Although the Sepsis-3 task force focused on adults, it recognized the need for research to adapt qSOFA criteria for use in pediatric patients. Currently, Sepsis-3 doesn’t consider pediatric pathophysiology and age-dependent vital signs, and it lacks supporting evidence in the pediatric population. In children, increased respiratory and heart rates alone aren’t clinically definitive for sepsis. Also, not only do children’s compensatory mechanisms differ from those of adults, but children with sepsis may have adequate blood pressure, with hypotension developing only as a late sign of septic shock. Without an evidence-based (EB) adaptive screening tool specifically for children, clinicians must be extra vigilant in assessing patients to recognize subtle changes.
Risk factors
In children, sepsis risk factors include:
• infancy (less than 8 weeks old)
• compromised immune system
• concurrent illness
• wounds or injuries (including burns)
• invasive medical devices (including indwelling catheters)
• hemoglobin SS disease (the most common type of sickle cell disease), which carries a 400-fold higher risk of sepsis
• congenital heart disease
• current hospitalization.
To help identify sepsis risk factors, obtain a concise history from family members, including the patient’s symptoms and their onset and severity. Also find out if the patient recently was exposed to sick family members or classmates.
Assessment
Perform a thorough head-to-toe assessment to help identify signs of sepsis. Stay alert for vital-sign changes, such as increased temperature, faster heart or respiratory rates, altered skin perfusion, and subtle mental-status changes.
For instance, a toddler may become more difficult to console or seem “extra sleepy” since the last assessment. If you detect such changes, alert the practitioner right away. Monitor vital signs closely, correlating them with the child’s age.
A child with sepsis may experience the signs and symptoms listed next. But be aware that independently, these aren’t definitive diagnostic indicators of sepsis.
• core temperature above 101.3° F (38.5° C) or below 96.8 F° (36° C)
• tachycardia; or in children younger than 1 year, bradycardia
• tachypnea
• above- or below-normal white blood cell (WBC) count or an immature neutrophil count above 10%
• bounding peripheral pulses or decreased peripheral pulses (compared to central pulses)
• narrow pulse pressure with cold shock or a wide pulse pressure with warm shock
• pale, mottled, or cool extremities with vasoconstriction (cold shock)
• warm, flushed peripheral extremities (warm shock)
• capillary refill longer than 3 seconds
• dry mucous membranes
• sunken eyes
• decreased urine output
• bradypnea or apnea
• hypotension (can be a late sign)
• altered level of consciousness or mental status, such as irritability, anxiety, confusion, or lethargy
• petechial or purpuric rash (a late indicator of septic shock).
While elevated temperatures and WBC counts can signify the body’s normal healthy response to infection, clinicians must recognize when these normal responses have become compromised and dysfunctional, impairing organ function. As sepsis worsens or septic shock develops, tissue perfusion drops dramatically.
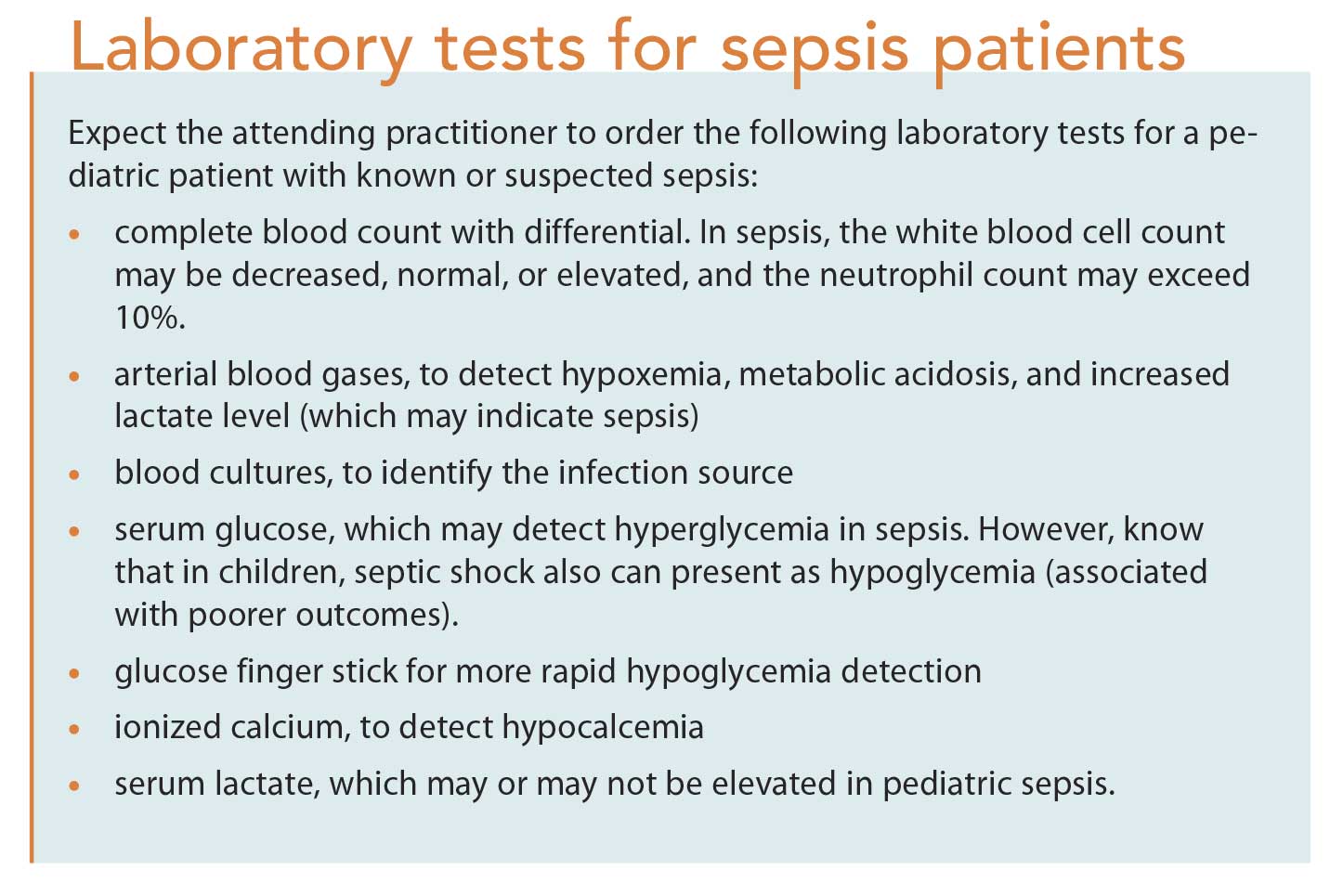
Further testing and laboratory results are needed to confirm organ dysfunction related to infection. (See Laboratory tests for sepsis patients.)
Management
If you suspect your patient has sepsis, immediately notify the attending practitioner and request available nurses to assist with this critical condition. The clock starts when sepsis is identified. Many hospital guidelines require clinicians to complete certain time-sensitive interventions at first recognition of sepsis. Use of the American Heart Association Pediatric Advanced Life Support’s sepsis shock algorithm and hospital-dependent bundles and guidelines for treating sepsis has improved outcomes and decreased hospital stays for patients with sepsis.
As ordered, begin oxygen administration via nonrebreather face mask at 15 L/minute, regardless of the patient’s blood oxygen saturation. Some patients may require high-flow nasal cannula, nasopharyngeal continuous positive airway pressure, or early intubation and mechanical ventilation.
Place the patient on a cardiac monitor with continuous pulse oximetry. As ordered, insert two large-bore I.V. lines (as large as the patient’s vein will support). After two failed I.V. insertion attempts, prepare for intraosseous access. In some cases, a central line may be placed.
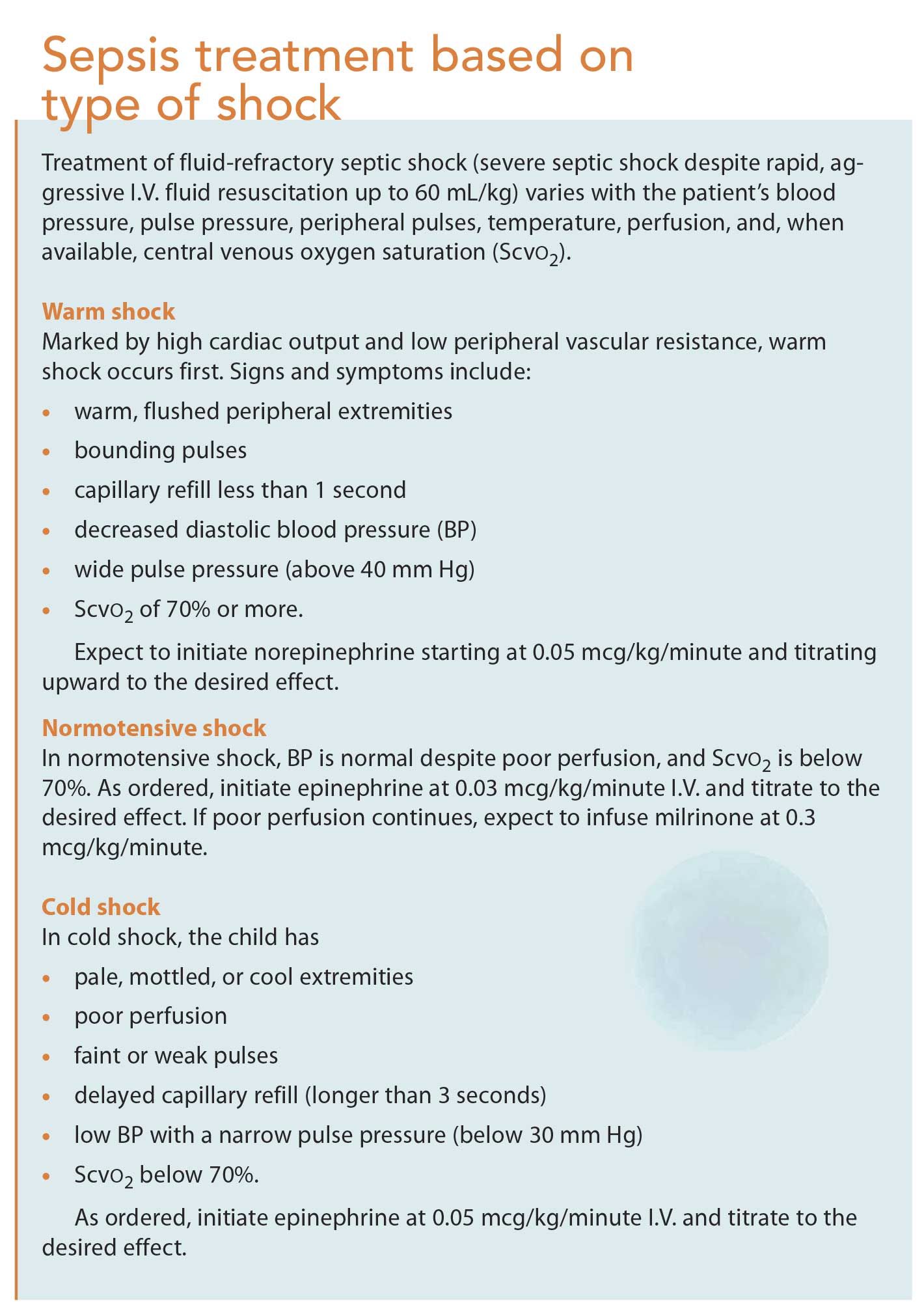
Expect the practitioner to order rapid resuscitation fluids (isotonic crystalloids—specifically Lactated Ringer’s or normal saline solution) administered by I.V. push at a rate of 20 mL/kg. As ordered, repeat boluses up to four times unless respiratory distress, crackles, or hepatomegaly develops. Fluid resuscitation should continue with vasopressors until blood pressure and peripheral perfusion improve. The type of shock (normotensive, warm, or cold) determines which drug is ordered. (See Sepsis treatment based on type of shock.)
Strict fluid intake and output documentation is crucial, so anticipate inserting an indwelling urinary catheter. As ordered, administer glucose to correct hypoglycemia and calcium chloride or calcium gluconate to correct hypocalcemia. For febrile patients, expect to give antipyretics as well.
Draw samples for a complete blood count with differential, arterial blood gases, blood cultures, serum glucose (or glucose finger stick), ionized calcium, and serum lactate. Notify the practitioner of critical laboratory values, and obtain blood culture specimens before antibiotic therapy begins. However, know that broad-spectrum antibiotics must be given within 1 hour of sepsis recognition and must not be delayed if blood specimens can’t be obtained.
Continue to monitor the patient’s vital signs frequently. Check for signs of fluid overload every 5 to 15 minutes; these include increased work of breathing, crackles on lung auscultation, an irregular gallop rhythm on heart auscultation, and an enlarged liver on palpation. The patient may need to be monitored in the pediatric intensive care unit (PICU). If your facility lacks PICU services, the patient may require transfer to a tertiary care center.
Applying the evidence
To improve early sepsis recognition, clinicians need to take active roles in creating policies and EB protocols specific to pediatric sepsis. Too often, we view pediatric care through the lens of adult care even when specialty care is crucial. Many state health departments, hospital associations, and policy makers have banded together to create legislation, regulations, and initiatives with common goals—to implement EB policies and processes and to educate staff to rapidly recognize and treat sepsis, collect data, identify gaps, and share sepsis prevention and best practices. The Surviving Sepsis Campaign encourages hospitals to initiate sepsis intervention bundles. Hospitals can customize these bundles to maximize benefits as long as they uphold the same standards.
Possible flaws in the EHR
Many hospitals use electronic health records (EHRs) to create order set sepsis bundles. Technology can extrapolate pertinent data entered into the EHR, such as vital signs and laboratory values, to generate sepsis-warning and best-practice notifications. If the patient meets sepsis criteria, a warning is generated, signaling the nurse to notify the attending practitioner. Practitioners receive similar notifications to initiate the order set. This system lets practitioners use their best clinical judgment; in some cases, the practitioner may conclude that although a particular patient appears to meet sepsis criteria, a different underlying cause explains the presence of these criteria.
Unfortunately, some EHRs lack age-specific vital signs and laboratory values to capture true sepsis in pediatric patients. As a result, false-positive warnings may occur, which can lead to warning fatigue and cause clinicians to ignore valid warnings.
EHRs must be fine-tuned to detect sepsis early in children. Along with continual education on pediatric sepsis for all healthcare providers, EHR improvements are crucial for saving the lives of children with sepsis.
Melanie L. Cardona is an administrative supervisor at Hackensack University Medical Center in Hackensack, New Jersey, and a clinical instructor at Ramapo College of New Jersey in Mahwah.
Selected references
American Heart Association. Pediatric Advanced Life Support: Provider Manual. Dallas, TX: Author; 2016.
Centers for Disease Control and Prevention. State policy approaches to sepsis prevention and early recognition.
Children’s Hospital of Philadelphia. ICU pathway for the evaluation/treatment of infants
> 28 days and children with severe sepsis/septic shock. Revised February 2016.
Cummings BM. Treatment of sepsis and septic shock in children. Updated January 7,
2016.
European Society of Intensive Care Medicine. Sepsis-3: International consensus definitions for sepsis and septic shock.
Goldstein B, Giroir B, Randolph A; International Consensus Conference on Pediatric Sepsis. International pediatric sepsis consensus conference: definitions for sepsis and organ dysfunction in pediatrics. Pediatr Crit Care Med. 2005;6(1):2-8.
Jeffery AD, Mutsch KS, Knapp L. Knowledge and recognition of SIRS and sepsis among pediatric nurses. Pediatr Nurs. 2014;40(6): 271-8.
Paul R, Neuman MI, Monuteaux MC, Melendez E. Adherence to PALS sepsis guidelines and hospital length of stay. Pediatrics. 2012; 130(2):e273-e80.
Santhanam S. Pediatric sepsis. Updated August 24, 2016.
Sepanski RJ, Godambe SA, Mangum CD, Bovat CS, Zaritsky AL, Shah SH. Designing a pediatric severe sepsis screening tool. Front Pediatr. 2014;2:56.
Seymour CW, Liu VX, Iwashyna TJ, et al. Assessment of clinical criteria for sepsis: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315(8):762-74.
Singer M, Deutschman CS, Seymour CW, etal. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315(8):801-10.
Society of Critical Care Medicine. Surviving Sepsis Campaign: Bundles. April 2015.
Weiss SL, Pomerantz WJ. Septic shock: rapid recognition and initial resuscitation in children. May 26, 2016.

















{kind=link}
{kind=link}
{kind=link}