
Treatment for this rare disorder may require repeat surgeries.
Takeaways:
- Recurrent respiratory papillomatosis (RRP) is disease, but it’s progressive and can effect quality of life and even be life threatening.
- HPV vaccination is a promising measure to prevent RRP occurrence in children.
By Caitlin Volz Winn, MSN, RN, CPN
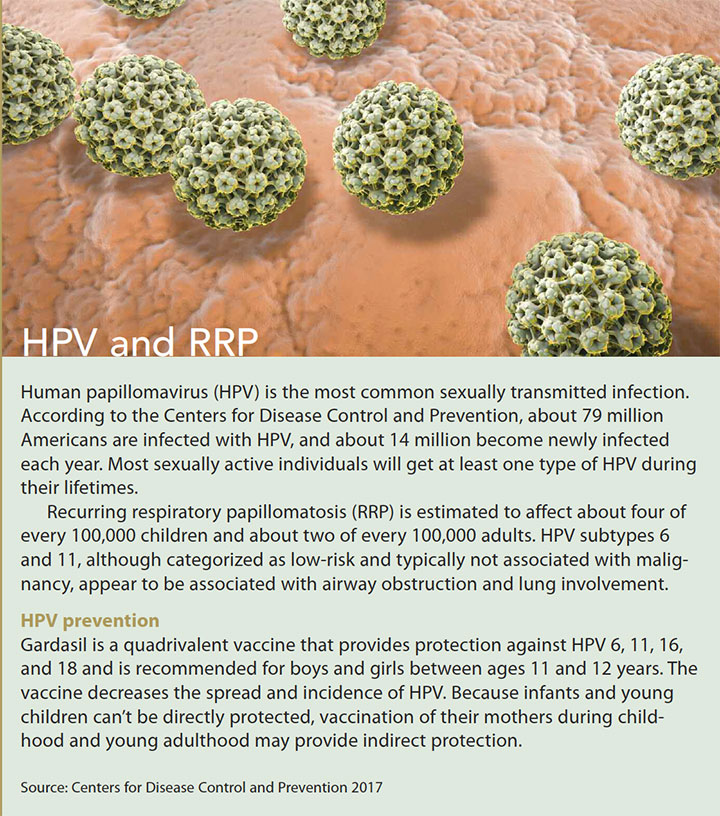
Recurrent respiratory papillomatosis (RRP) is a rare disorder caused by the growth of wartlike, noncancerous tumors (papillomas) in the respiratory tract. Papillomas can develop anywhere along the respiratory tract but most often affect the larynx and the vocal cords. Less often, the tumors appear in the mouth, trachea, and bronchi. Only in rare cases do these growths spread to the lungs. RRP can affect children or adults and is caused by human papillomavirus (HPV). (See HPV and RRP.)
Children who develop the disease earlier in life frequently have worse prognoses. They may have more papilloma growths, require more frequent surgical interventions, and need a tracheotomy because of tracheal and pulmonary disease. Juvenile-onset RRP is typically more aggressive than adult-onset, most likely because of children’s smaller airway anatomy.
Papillomas tend to grow back after they’ve been removed, requiring repeated surgeries. These multiple procedures may negatively affect the quality of life of children and their families. Although benign, papillomas can cause severe, even life-threatening airway obstruction and respiratory complications.
Transmission
Those at the greatest risk for developing juvenile-onset RRP include firstborn children delivered vaginally to mothers under 20 years old with active condyloma (genital warts) during pregnancy. Adult-onset RRP is thought to be associated with sexual transmission. No evidence exists to show that RRP is transmitted through casual contact. It can’t be passed from child to child through playing or utensil sharing. Some research estimates that, over time, new cases of RRP will be prevented with the use of HPV vaccination.
Beyond the noted risk factors, little is known about why certain individuals develop RRP and others don’t. Approximately 5% of the U.S. population may have HPV in their respiratory tract, but fewer than one in 1,000 of those infected ever develop RRP. This is most likely related to a subtle immunologic deficiency affecting the respiratory tracts of those who develop the condition. Juvenile-onset RRP, which occurs in both boys and girls, is typically diagnosed by age 5.
 Presentation
Presentation
 Presentation
PresentationThe most common symptoms of RRP include chronic voice weakness, strain, hoarseness, decreased pitch, stridor, and respiratory distress. When lesions form near the vocal folds, hoarseness can occur quickly even with small lesions. Additional RRP symptoms—chronic cough, episodes of choking, recurrent pneumonia, failure to thrive, shortness of breath, difficulty swallowing, and snoring—may be mistaken for other conditions including croup, bronchitis, and vocal cord nodules. Young children often experience a weak cry, chronic cough, swallowing difficulties, and stridor. Stridor is a sign of an upper respiratory obstruction and warrants immediate attention by an ear, nose, and throat (ENT) specialist.
RRP symptoms may develop gradually over months or even years in mild cases, but it may emerge in a matter of days in very aggressive cases. The average time from symptom onset to diagnosis ranges from 1 to 8 years.
Diagnosis
Diagnostic evaluation of RRP includes an examination of the larynx or vocal cords by an ENT specialist. Assessment techniques include mirror examination of the vocal cords; laryngoscopy and videostroboscopy provide more detailed visualization. The definitive RRP diagnostic tool is direct laryngoscopy with surgical removal of papilloma growths for biopsy and HPV testing. This procedure is performed in the operating room with general anesthesia.
Treatment
RRP treatment goals include papilloma reduction, airway patency restoration, symptom improvement, disease spread prevention, and decreased hospitalizations.
With no definitive curative treatment for RRP, surgery is the most used option. Typically, surgery is performed with lasers to debulk the lesions. However, complications such as respiratory tract burns, severe laryngeal scarring, and stenosis have occurred with laser therapy. Recently, a technique using microdebriders has been adopted. This technique more selectively suctions the affected tissue, allowing for more precise debridement and decreasing damage to underlying tissues.
Surgical removal must be done as often as necessary to ensure an unobstructed airway. Surgery may be required anywhere from twice a month to once every 1 to 2 years. Despite more advanced surgical equipment, patients may still experience significant airway complications and require further management, such as a tracheostomy. Tracheostomies are used to bypass the obstructions of aggressive papilloma growth. Although a tracheostomy may be unavoidable in severe cases, decannulation should be considered as early as possible. Tracheostomies provide an additional site for papilloma growth and serve as a channel for disease spread to the lungs.
When RRP continues to occur even after repeated surgical debridements, or when it spreads to the lungs, additional medication therapy may be needed. Unfortunately, no single treatment has been found to be effective in treating all patients; providers frequently try several different drugs before finding one that reduces disease severity. Medical therapy is an attractive treatment option for children with aggressive RRP, but limited data exist about optimal dosage, effectiveness, and adverse effects.
Collaboration and communication between individual patients and providers is essential to determine treatment goals, choose the best treatment options, and manage side effects. The goal of current medical therapies is to reduce or eliminate the need for future surgeries. (See Medical therapy options.)
Nursing Implications
The care provided to children with RRP is multidisciplinary, with nurses at the forefront. Nursing care begins with identifying key RRP assessment findings, such as chronic coughing, choking, voice weakness, strain, hoarseness, stridor, and respiratory distress. In addition, note any changes from the patient’s previous presentation. Accurate vital signs and a full respiratory assessment—including pulse oximetry, breath sounds, and rate and rhythm—are critical tools for monitoring and identifying respiratory distress. Monitor your patient’s nutritional goals and potential deficits based on growth parameters and intake. In addition, be aware of the potential psychosocial impact the diagnosis and treatments can have on the patient and family; determine whether you need to make a referral to a therapist, social worker, or community-based program.
Future promise
Current treatment for juvenile-onset RRP focuses on surgical removal of tumors, which may have to be repeated as often as twice a month. The effect on the young patients and their families can lead to diminished quality of life. Increased HPV vaccination may help to reduce the number of children who acquire RRP during birth, and other treatment strategies under investigation hold promise that improved therapies to treat or prevent RRP will be available in the future.
Caitlin Volz Winn is a clinical staff nurse in the day medicine unit at Children’s Hospital of Philadelphia in Philadelphia, Pennsylvania, and an adjunct clinical professor for West Chester University, West Chester, Pennsylvania.
Selected references
Carifi M, Napolitano D, Morandi M, Dall’Olio D. Recurrent respiratory papillomatosis: Current and future perspectives. Ther Clin Risk Manag. 2015;11:731-8.
Centers for Disease Control and Prevention. Manual for the surveillance of vaccine-preventable diseases: Chapter 5: Human papillomavirus (HPV). November 10, 2017.
Fusconi M, Grasso M, Greco A, et al. Recurrent respiratory papillomatosis by HPV: Review of the literature and update on the use of cidofovir. Acta Otorhinolaryngol Ital. 2014;34(6):375-81.
Maturo SC, Hartnick CJ. Juvenile-onset recurrent respiratory papillomatosis. Adv Otorhinolaryngol. 2012;73:105-8.
Rogers DJ, Ojha S, Maurer R, Hartnick CJ. Use of adjuvant intralesional bevacizumab for aggressive respiratory papillomatosis in children. JAMA Otolaryngol Head Neck Surg. 2013;139(5):496-501.
Wilcox LJ, Hull BP, Baldassari CM, Derkay CS. Diagnosis and management of recurrent respiratory papillomatosis. Pediatr Infect Dis J. 2014;33(12):1283-4.
Voice Foundation, The. Recurrent respiratory papillomatosis.
ant7-Respiratory Papillomatosis-618

















