Be aware of this often misdiagnosed and possibly deadly condition.
- Nurses should have a high level of suspicion for spontaneous coronary artery dissection (SCAD) when patients, especially young women, present with chest pain and other acute coronary syndrome symptoms, in the absence of or in the presence of few atherosclerotic risk factors.
- Pregnancy-associated SCAD is most likely to occur within the first week to month postpartum.
- Nurses are uniquely positioned to provide emotional support and education to patients and family members to help them understand SCAD risk factors, signs and symptoms, medications, and for follow-up for long-term monitoring and care.
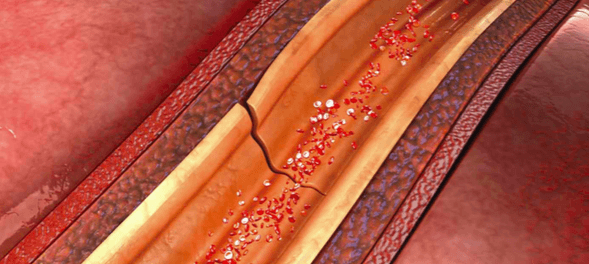
SPONTANEOUS coronary artery dissection (SCAD) is an uncommon, nonatherosclerotic cause of acute coronary syndromes (ACS), myocardial infarction (MI), and sudden death. It involves a spontaneous tear of the coronary artery’s inner wall, after which blood pools in the area of the tear, eventually forming a hematoma that reduces blood flow. The left anterior descending coronary artery is most frequently affected, but SCAD can be multi-vessel.
The true prevalence of SCAD remains unknown because of underdiagnosis and misdiagnosis (such as anxiety, gastric reflux, pericarditis, and Takotsubo cardiomyopathy), but it accounts for approximately 1% to 4% of all ACS. To aid in the prompt recognition and management of this life-threatening condition, nurses should understand the risk factors and associated conditions, signs and symptoms, diagnostic tests, and nursing implications.
Risk factors and associated conditions
SCAD is most common in middle-aged white women, although it also can occur in men and individuals of all racial and ethnic backgrounds. Other risk factors and associated conditions include fibromuscular dysplasia, pregnancy, extreme exertion, intense stress/emotion, misuse of illegal drugs (such as cocaine), exogenous hormone use, systemic inflammatory diseases (such as lupus, Crohn’s disease, and rheumatoid arthritis), and connective tissue disorders (such as Marfan syndrome and Ehler-Danlos syndrome).
Individuals who participate in vigorous aerobic activities and those experiencing severe emotional stress, such as a family member’s death, are at increased risk for SCAD. However, SCAD also can affect seemingly healthy women (and less commonly men), who don’t have traditional heart disease and MI risk factors (smoking, diabetes, physical inactivity, being overweight, family history of heart disease). This may contribute to the lack of recognition and initial misdiagnosis or underdiagnosis.
Signs and symptoms
Signs and symptoms of SCAD mimic those of ACS and MI, including chest pain or discomfort; extreme or unusual fatigue; nausea or vomiting; shortness of breath; pain in arms, back, shoulder, or jaw; lightheadedness; diaphoresis; and ventricular tachycardia or fibrillation. Approximately half of the patients who experience SCAD have ST-elevation MI (STEMI); the other half may have ST depression or a normal electrocardiograph.
Diagnosis
Prompt and accurate SCAD diagnosis is critical to save lives. However, when a patient who has no cardiovascular risk factors arrives in an emergency department (ED), he or she may be misdiagnosed and prematurely discharged. The first-line approach for diagnosing SCAD is coronary angiography because of its wide availability; a grading system helps with recognition and use in early invasive SCAD management. (See Grading SCAD.) Other imaging techniques include intravascular ultrasound and optical coherence tomography. These techniques aren’t widely available, and expertise in their use varies, but they provide a more detailed examination of the arterial wall (compared to coronary angiography) to help confirm a SCAD diagnosis.
Grading SCAD
Spontaneous coronary artery dissection (SCAD) diagnosis is based on coronary angiography findings and is graded as one of three types.
Type 1—classic appearance of the radiolucent intimal flap
Type 2—presence of diffuse stenosis of varying severity and length
- Variant 2a—diffuse narrowing bordered by normal segments proximal and distal to the intramural hematoma
- Variant 2b—diffuse narrowing that extends to the distal tip of the artery
Type 3—mimics atherosclerosis in the presence of focal or tubular stenosis
Sources: Saw 2014, Saw et al. 2016
Management
In the absence of randomized clinical trials of stent-based therapy to treat SCAD and because most dissections will heal spontaneously, a conservative management approach is preferred for stable patients. This approach consists of 3 to 5 days of inpatient monitoring for extension of dissection (which would require emergency revascularization) combined with medication therapy (dual-antiplatelet therapy, beta blockers, angiotensin-converting enzyme inhibitors, and angiotensin receptor blockers).
For high-risk patients (those who are hemodynamically unstable, have left main artery dissection, or have ongoing ischemia), percutaneous coronary intervention (PCI) or coronary artery bypass grafting may be considered. These approaches must be balanced with increased risk of adverse outcomes and complications.
All patients with SCAD should be referred for cardiac rehabilitation that includes conservative thresholds for blood pressure and weight and strength training. They should avoid the Valsalva maneuver, which places excessive stress on the heart. Patients with SCAD also should avoid prolonged high-intensity physical activities and exercising in extreme temperatures (for example, jogging in cold weather and hot yoga).
Because patients with SCAD are at risk for recurrence, MI, and heart failure, long-term management is recommended with annual visits that include an ECG and a comprehensive history and physical. More frequent visits are needed if health status changes occur (for example, pregnancy) or symptoms (for example, chest pain) return. Some patients may require repeat coronary angiograms to reimage the vessel and to look for ischemia and iatrogenic dissections.
In addition to having their physical health needs managed, patients also should be monitored for depression and anxiety. Mental health interventions include participating in organizational and peer support groups, getting family or marriage counseling, and receiving behavioral and pharmacologic therapy (such as antidepressants).
Genetic and reproductive counseling also is advised. Genetic counseling evaluates for genetic connective tissue disorders and vasculopathy. Reproductive counseling is recommended for all women of childbearing age. Pregnancy in women with SCAD is generally discouraged, but if the patient decides to pursue it, a multidisciplinary team (cardiologists, maternal-fetal medicine specialists, anesthesiologists, and nurses) should be involved in her care. (See Pregnancy and SCAD.)
Pregnancy and SCAD
 Pregnancy and the postpartum period are times of increased risk for spontaneous coronary artery dissection (SCAD), especially in women who’ve given birth four or more times. Although this increased risk is not fully understood, some researchers speculate it’s the result of hormone receptors in the coronary arteries that cause histological arterial wall abnormalities and weaken the walls. Pregnancy-associated SCAD may occur any time during pregnancy, but it’s most likely to occur late in pregnancy or within the first several weeks postpartum.
Pregnancy and the postpartum period are times of increased risk for spontaneous coronary artery dissection (SCAD), especially in women who’ve given birth four or more times. Although this increased risk is not fully understood, some researchers speculate it’s the result of hormone receptors in the coronary arteries that cause histological arterial wall abnormalities and weaken the walls. Pregnancy-associated SCAD may occur any time during pregnancy, but it’s most likely to occur late in pregnancy or within the first several weeks postpartum.
Prognosis and likely recurrence
Over the next 2 to 3 years after the initial SCAD event, death or recurrence of chest pain, depression, anxiety, and major adverse cardiovascular events (MI, heart failure, stroke) occur in 10% to 30% of patients. By 10 years, approximately half of SCAD patients will have another major cardiac event.
Nursing implications
All nurses, especially ED nurses, should have a high level of suspicion for SCAD when patients, particularly young women, present with chest pain or other ACS symptoms but have no or few atherosclerotic risk factors. Nurses can help facilitate coronary angiography as early as possible, especially in the case of STEMI.
Post-SCAD care includes vigilant assessment and monitoring for hemodynamic instability, cardiac arrhythmias, fluid overload, and signs and symptoms of ischemia (for example, chest pain or persistent ST elevation). Alert providers immediately if these occur to en- sure prompt medical intervention.
Postpartum care
During the immediate postpartum period for women with SCAD, monitor for signs and symptoms of bleeding in patients who receive percutaneous coronary intervention along with antiplatelet therapy and anticoagulation therapy. Monitor the number of perineal pads used, evaluate the quality and quantity of lochia, watch for perineum pain or swelling, and assess for hemodynamic instability (hypotension, tachycardia, dizziness, diaphoresis). In addition, ensure mothers make time to bond with their newborns. For patients with lifting restrictions, offer assistance by holding or helping to place the newborn close to the mother or in her arms.
Additional nursing considerations include consultation with the pharmacist (some cardiac medications may be contraindicated for women who breastfeed) and referral to a social worker (for assistance with family support services, if needed).
Emotional support and education
SCAD is a frightening, life-threatening experience for patients and family members. You can provide emotional support and education to help them understand SCAD risk factors, signs and symptoms, medications, and the need for cardiac rehabilitation and follow-up medical monitoring and care. In addition, counsel patients to engage in heart-healthy behaviors, such as smoking cessation, eating a heart-healthy diet, and exercising, as directed by the provider. (See Patient resources.)
Patient resources
Refer patients with spontaneous coronary artery dissection (SCAD) to these online resources.
American Heart Association. Coronary artery dissection: Not just a heart attack
bit.ly/2V3h3SP
This page gives patients an overview of SCAD and includes a video interview with a patient who experienced SCAD about 10 days after the birth of her fourth child.
American Heart Association. Hands-only CPR
bit.ly/2U2uKRC
Patients can access this site to get information about cardiopulmonary resuscitation training.
Mayo Clinic. Centers and programs: Spontaneous coronary artery dissection
mayocl.in/2EgT39h
This site includes social media and online support as well as information about research trials.
The National Coalition for Women with Heart Disease
womenheart.org
This organization is dedicated to supporting women with heart disease.
SCAD Alliance
scadalliance.org/resources
The SCAD Alliance website includes information for medical professionals and patients, including links to support groups and research.
Index of suspicion
SCAD is a life-threatening cause of ACS that affects predominately young seemingly healthy women without traditional cardiovascular risk factors. Consider SCAD in these patients to avoid misdiagnosis and lethal outcomes.
Cynthia Arslanian-Engoren is an associate professor and associate dean of faculty affairs and faculty development at University of Michigan school of nursing in Ann Arbor.
Selected references
Alfonso F, Bastante T, Garcia-Guimaraes M, et al. Spontaneous coronary artery dissection: New insights into diagnosis and treatment. Coron Artery Dis. 2016;27(8):696-706.
Hayes SN, Kim ESH, Saw J, et al. Spontaneous coronary artery dissection: Current state of the science: A scientific statement from the American Heart Association. Circulation. 2018;137(19):e523-57.
Hickox BC, Mikshowsky JA. Spontaneous coronary artery dissection: Recognition, triage, and management in the emergency department. J Emerg Nurs. 2016;42(4):301-5.
Jeejeebhoy FM, Zelop CM, Lipman S, et al. Cardiac arrest in pregnancy: A scientific statement from the American Heart Association. Circulation. 2015;132(18):1747-73.
Levine GN, Bates ER, Blankenship JC, et al. 2015 ACC/AHA/SCAI focused update on primary percutaneous coronary intervention for patients with ST-elevation myocardial infarction: An update of the 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention and the 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation. 2016;133(11):1135-47.
Luong C, Starovoytov A, Heydari M, Sedlak T, Aymong E, Saw J. Clinical presentation of patients with spontaneous coronary artery dissection. Catheter Cardiovasc Interv. 2017;89(7):1149-54.
Macaya F, Salinas P, Gonzalo N, Fernández-Ortiz A, Macaya C, Escaned J. Spontaneous coronary artery dissection: Contemporary aspects of diagnosis and patient management. BMJ Journals. 2018. openheart.bmj.com/content/5/2/e000884
Mahmoud AN, Taduru SS, Mentias A, et al. Trends of incidence, clinical presentation, and in-hospital mortality among women with acute myocardial infarction with or without spontaneous coronary artery dissection: A population-based analysis. JACC Cardiovasc Interv. 2018;11(1):80-90.
Martinez LG. Spontaneous coronary artery dissection: A rare threat to young women. Crit Care Nurse. 2012;32(4):e19-26.
Mehta LS, Beckie TM, DeVon HA, et al. Acute myocardial infarction in women: A scientific statement from the American Heart Association. Circulation. 2016;133(9):916-47.
O’Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127(4):e362-425.
Saw J. Coronary angiogram classification of spontaneous coronary artery dissection. Catheter Cardiovasc Interv. 2014;84(7):1115-22.
Saw J, Mancini GBJ, Humphries KH. Contemporary review on spontaneous coronary artery dissection. J Am Coll Cardiol. 2016;68(3):297-312.
Tweet MS, Gulati R, Hayes SN. What clinicians should know about spontaneous coronary artery dissection. Mayo Clin Proc. 2015;90(8):1125-30.
Tweet MS, Kok SN, Hayes SN. Spontaneous coronary artery dissection in women: What is known and what is yet to be understood. Clin Cardiol. 2018;41(2):203-10.
Wagers TP, Stevens CJ, Ross KV, Leon KK, Masters KS. Spontaneous coronary artery dissection (SCAD): Female survivors’ experiences of stress and support. J Cardiopulm Rehabil Prev. 2018;38(6):374-9.
Wilbur J, Braun LT, Arslanian-Engoren C, Lauver DR, Halloway S. Assessing and addressing cardiovascular risk in young women. Nurs Outlook. 2018;66(3):325-8.
Yip A, Saw J. Spontaneous coronary artery dissection—A review. Cardiovasc Diagn Ther. 2015;5(1):37-48.

















