
Nursing skills and implications.
Takeaways:
- Suicide is a preventable and growing public health risk, and nurses are in a prime position to provide assessment and follow-up care.
- Many nurses lack sufficient education to assess suicide, but a growing body of information is available.
- Nurses’ role in suicide prevention includes assessment, safety plan creation, and continually monitoring.
According to the Centers for Disease Control and Prevention (CDC), U.S. suicide rates between 1999 and 2017 rose to 47,511 deaths. Currently the 10th leading cause of death, a suicide occurs every 11 minutes. These numbers represent only a snapshot of those affected by suicide. In 2017, another 1.4 million attempted suicide, 3.2 million made a plan for suicide, and 10.6 million had serious thoughts of suicide. According to the American Foundation for Suicide Prevention, suicide and suicide attempts cost roughly $70 billion per year in lifetime medical and work-loss costs. This loss of life and financial burden is preventable.
As the primary providers of hospital-based and long-term care, nurses hold a prime position to act as change agents in the suicide epidemic. In a survey by the Substance Abuse and Mental Health Service Administration, only half of healthcare professionals reported receiving education on suicide assessment and follow-up care, and only a third felt strongly that they had the knowledge and comfort in using those skills. Yet The Joint Commission’s updated National Patient Safety Goal addressing suicide prevention emphasizes the need for suicide assessment and follow-up education. This article provides an overview of these skills that nurses can apply to their practice.
Patients at risk
According to the CDC, middle-aged white men have the highest suicide risk, with firearms the most common method used. However, all patients should be assessed because suicide affects all ages, races, ethnicities, and genders. Risk factors include a history of suicide attempts, family or friend suicide, or mental health or substance use disorders; isolation; hopelessness; physical illness; recent loss; and access to a lethal means. Protective factors include support, effective clinical care, access to healthcare, and healthy coping skills.
Assessment
The ability to connect and build rapport is essential to the suicide assessment process. Use a caring and nonjudgmental approach to allow the patient to feel emotionally supported and safe. Educate the patient about suicide and validate their feelings, while also conveying hope for the future. People who are suicidal don’t fit a set stereotype, so treat them as individuals with unique backgrounds and needs. Collaboration provides the foundation of an accurate assessment and follow-up. A common myth persists that assessing for suicide will put the idea of suicide in the patient’s head. However, the only way to detect suicide risk is by talking about it.
Assessment tools
Many assessment tools can measure various aspects of suicide, but most haven’t been adequately tested in subsets of patients. Therefore, rather than read directly from the tool, use it to develop a line of questioning during a patient assessment. (See Suicide assessment tools.)
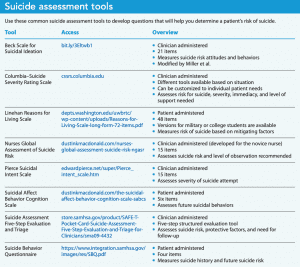
The Columbia–Suicide Severity Rating Scale’s free clinician-administered protocol can assess risk, severity, immediacy, and level of support needed. Although it may look daunting, this comprehensive tool guides nurses through questions and actions. The Suicide Assessment Five-Stop Evaluation, another free tool, provides guidance rather than a specific list of questions to assess for risk, protective factors, and need for follow-up.
For a fee, the more structured 21-item clinician-administered Beck Scale for Suicidal Ideations measures suicidal thoughts and behaviors. The Nurses Global Assessment of Suicide Risk, a similar tool designed specifically for nurses, assesses suicide risk and level of observation recommended but has not been empirically tested for validity and reliability.
Brief tools include the 6-item Suicidal Affect Behavior Cognition Scale and the 4-item Suicide Behavioral Questionnaire. These self-report tools can help assess future suicidal behaviors
The Linehan Reasons for Living Scale doesn’t assess for suicide, but it can be used to measure risk of suicide based on mitigating factors, such as purpose for living, family obligations, and fear of death. The patient self-administers this 48-item tool. Versions of the Linehan scale are available for college students and military personnel. For patients who have attempted suicide, the 15-item Pierce Suicide Intent Scale, a clinician-administered tool, assesses suicide attempt severity.
Because depression and hopelessness are linked to suicidality, assessment tools designed to measure them can help you more fully understand suicide risk. Common assessment tools for depression include the Beck Depression Inventory, the Hamilton Depression Rating Scale, and the Patient Health Questionnaire. The Beck Hopelessness Scale assesses hopelessness.
Risk level
Your suicide assessment should include direct questions about plans, risk factors, protective factors, triggers, and warning signs. When suicidal ideation is present, ask direct questions, such as “Have you tried to kill yourself in the past?” “If you were going to kill yourself, how would you do it?” “What helps you when you’re having thoughts of suicide?”
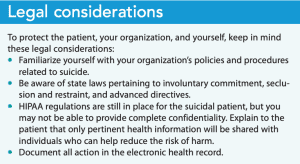
Gathering information from a family member or friend can be helpful. The Health Insurance Portability and Accountability Act (HIPAA) permits a provider to release private health information with patient permission or if contacting a resource (friend, family member, care provider, or emergency services) will reduce the risk of patient harm. Depending on the setting, share this information with other healthcare team members, such as the provider, nursing supervisor, or social worker.
Consider the short- and long-term risk that a patient will attempt or complete suicide. Ask detailed questions about the suicide plan and accessibility to means. For example, a patient who verbalizes a plan to overdose on their diabetic medications would be more at risk if they use an insulin pump compared to a patient who takes metformin. In addition, a patient might not have an intent or plan in the hospital but may have one for after discharge. Asking concrete questions (“Do you have access to a gun or medication at home?” “Do you have a plan for killing yourself in the hospital?” “How about after discharge?”) will help you assess the risk level.
You’ll also need to distinguish between acute and chronic suicidal ideations and determine whether self-harm includes the intent to die. For instance, a patient with a physical health issue and pain may say they want to go to sleep and never wake up but have no suicidal intent or plan, and many patients who self-harm by cutting aren’t suicidal.
Environmental assessment
Make an ongoing assessment of the environment and determine any need for modifications for patient safety. Environmental hazards in a healthcare setting include ligature points or objects that could be used for binding tightly (such as open plumbing, doorknobs, and bed rails) and self-harming objects (such as items in a sharps container, dining ware, or hard plastics that can be broken). Personal hazards include shoelaces, belts, home medications, or other sharp objects. Watch for patient hoarding and unnecessary items in their room, such as extra towels or linens that pose a strangulation risk. Some items can be removed, but many cannot. Consider whether an elevated level of supervision would ensure safety.
Develop a nursing plan
Address the patient’s need for safety in the least restrictive method possible. Develop your written plan of care (including a safety plan) in collaboration with the patient, healthcare team, and patient support system. According to the Suicide Prevention Resource Center, a suicide plan of care should include warning signs, coping strategies, social contacts, family and friend support, professional help, and environmental safety. Consider coordinating with other service providers, such as a psychiatric nurse practitioner.
Your plan also should include logistics for an active rescue, such as access to blunt-tip scissors to cut a ligature, advanced airway management for someone who has airway obstruction, and compression materials for someone who has severely cut themselves.
Continually collaborate with the patient to discuss internal and external barriers to adhering to the nursing plan. Support the patient, encourage them to discuss emotions, and help them practice coping skills. At the same time, establish boundaries of care for yourself and other healthcare providers. You’re not a substitute for a therapist.
Before patient discharge, advocate for collaboration with an outpatient therapist or psychiatric provider. Discuss follow-up appointments with the patient, offer support, and check for clarity and feasibility. Provide appointment dates, times, locations, and contact information to the patient and members of their personal support system, as well as discharge paperwork they should take to the appointment. Also share information about community engagement programs, such as support groups, suicide hotlines, crisis intervention centers, and local emergency departments. (See Legal considerations.)
Self-care for nurses
Working with a suicidal patient is stressful, so ongoing self-care is essential. Prioritize self-care activities at work—including taking a lunch break, using sick and vacation days, and minimizing overtime—and access workplace support from supervisors and mentors, as well as via debriefings. At home, implement physical, emotional, and spiritual activities. Nurses aren’t immune from suicidal thoughts, so be aware that you also may need to access suicide prevention resources.
Self-care resources include the Well-Being Initiative (nursingworld.org/practice-policy/work-environment/health-safety/disaster-preparedness/coronavirus/what-you-need-to-know/the-well-being-initiative/) and Healthy Nurse, Healthy Nation™ (healthynursehealthynation.org).
Be a change agent
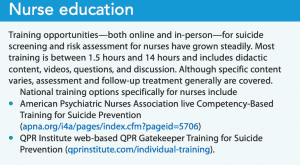
Suicide remains a growing but preventable cause of death. Nurses can serve as change agents, but we need education and tools to effectively assess patient risk and provide appropriate follow-up care. And remember that you can’t pour from an empty cup. Make self-care a priority, and take advantage of workplace and other support services. (See Nurse education.)
If you have thoughts of suicide or self-harm, call the National Suicide Prevention Lifeline at 1 800-273-TALK. If you believe someone is at imminent risk of harming themselves and is refusing help or you have reason to believe someone has harmed themselves, call 911.
Brittany Haskell is an instructor of nursing at Vanderbilt University in Nashville, Tennessee.
References
American Foundation for Suicide Prevention. Suicide statistics. March 1, 2020. afsp.org/suicide-statistics
American Psychiatric Association. Practice Guideline for the Assessment and Treatment of Patients with Suicidal Behaviors. November 2003. psychiatryonline.org/pb/assets/raw/sitewide/practice_guidelines/guidelines/suicide.pdf
American Psychiatric Nurses Association. Psychiatric-mental health nurse essential competencies for assessment and management of individuals at risk for suicide. February 27, 2015. apna.org/resources/suicide-competencies
Bolster C, Holliday C, Oneal G, Shaw M. Suicide assessment and nurses: What does the evidence show? Online J Issues Nurs. 2015;20(1):2.
Centers for Disease Control and Prevention. WISQARS leading cause of death reports. 2017. wisqars.cdc.gov/fatal-leading
Department of Health and Human Services. HIPAA Helps Caregiving Connections. hhs.gov/sites/default/files/hipaa-helps-prevent-harm.pdf
The Joint Commission. National Patient Safety Goal for Suicide Prevention. November 20, 2019. jointcommission.org/-/media/tjc/documents/standards/r3-reports/r3_18_suicide_prevention_hap_bhc_cah_11_4_19_final1.pdf
Smiley RA, Lauer P, Bienemy C, Shireman E, Reneau KA, Alexander M. The 2017 national nursing workforce survey. J Nurs Regul. 2018;9(3):S1-88.
Substance Abuse and Mental Health Service Administration. September 18, 2018. Assessing workforce readiness to provide comprehensive suicide care. bit.ly/3nNvQ3V
Suicide Prevention Resource Center. Safety Planning Guide. 2008. sprc.org/sites/default/files/SafetyPlanningGuide%20Quick%20Guide%20for%20Clinicians.pdf
U.S Bureau of Labor Statistics. Occupational outlook handbook: Registered nurses. September 28, 2021. www.bls.gov/ooh/healthcare/registered-nurses.htm
Key words: Suicide, Suicide assessment

















