
Home and inpatient skills combine to provide hospital-level care at home.
- Hospitals aren’t always the best environment for care, especially among older frail adults at risk for hospital-associated complications.
- Acute nursing care in the home draws an skills sets from home health, inpatient, and telehealth medicine.
Hospital at home (HaH) provides hospital-level care in a patient’s home in lieu of traditional inpatient care. HaH developed out of recognition that hospitals frequently aren’t ideal care environments, especially for older frail adults susceptible to hospital-associated complications. Since the COVID-19 pandemic began, interest in avoiding hospital care has increased. Nursing plays an integral role in HaH care, drawing on skill sets from home health, inpatient, and telehealth medicine.
HaH History
In the 1990s, Bruce Leff, MD, introduced HaH to the United States at The Johns Hopkins Hospital. However, the model stalled due to the multi-payer system and the absence of an accepted payment model. Internationally, HaH has scaled in several countries, including Australia, France, and Spain. A few U.S. health systems have maintained HaH programs since the 1990s, most notably at Department of Veterans Affairs hospitals. Some programs have grown out of home-based primary care (traditional house calls), but are distinctive in patient acuity level (HaH treats acute conditions requiring inpatient care, whereas home-based primary care treats simple acute and chronic conditions).
Evidence suggests that, compared to traditional hospital care, HaH is associated with improved patient safety, reduced mortality, a better patient and family experience, enhanced quality, and reduced cost. Common HaH-qualifying conditions include exacerbations of chronic heart failure, chronic obstructive pulmonary disease and asthma, COVID-19 pneumonia, infections requiring I.V. antibiotics, and post-chemotherapy neutropenia. Eligible patients must live in a safe home environment suitable for HaH care.
In 2014, Mount Sinai Health System, in New York City, received a Centers for Medicare & Medicaid Innovation award to implement an HaH program, which so far has cared for more than 1,000 patients. Within the Mount Sinai program, acute care RNs (ACRNs) visit patients twice daily, and a physician or nurse practitioner (NP) sees the patient daily via in-person or telehealth visits. Patients have access to the care team 24 hours 7 days a week, including urgent evaluations by a community paramedic.
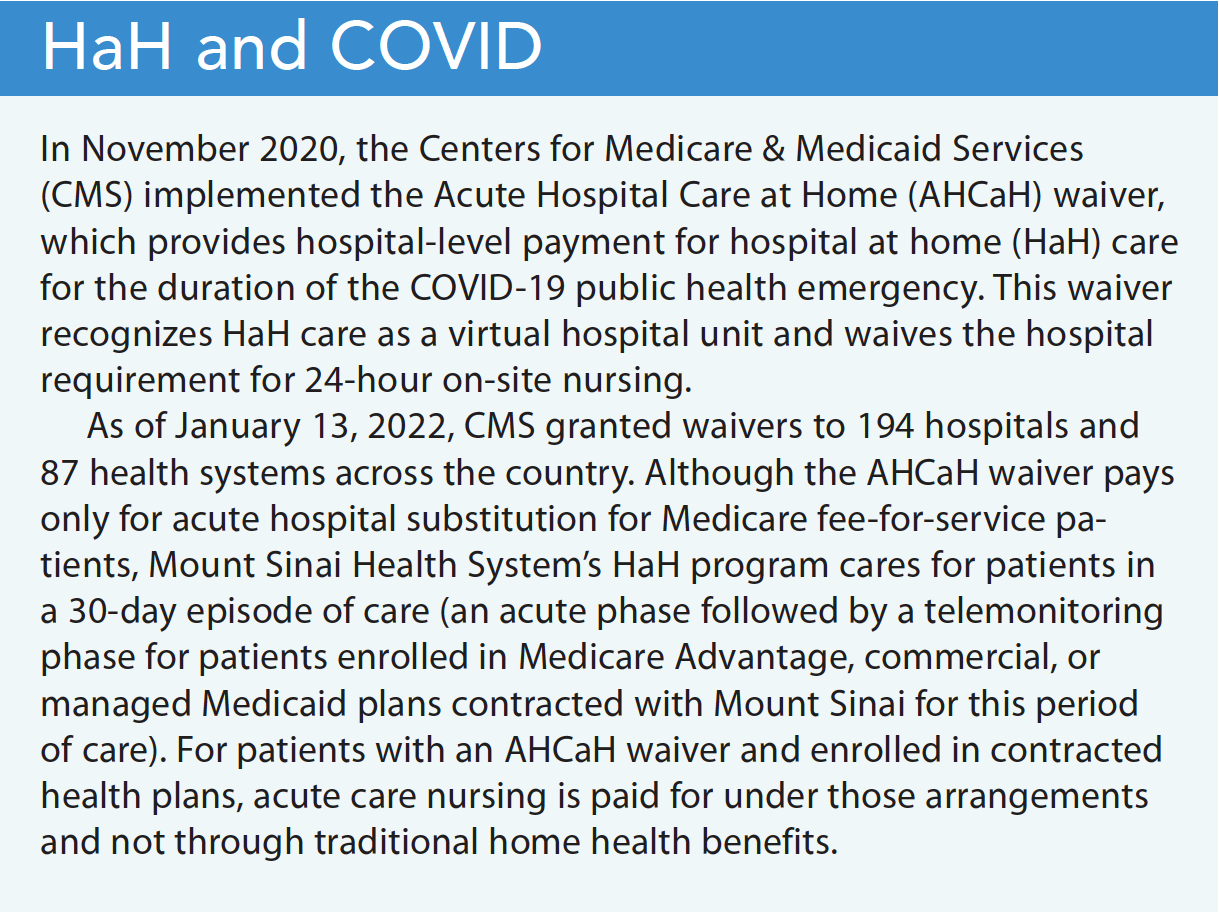
Before the COVID-19 pandemic, a shift to value-based care drove growing interest in HaH. Hospitals experiencing capacity issues considered HaH programs a solution to increasing traditional hospital capacity. As the initial waves of COVID-19 hit major cities, concerns about hospital capacity led several existing HaH programs to expand and adapt their models. (See HaH and COVID.)
HaH care delivery
The literature describes two main categories of HaH care delivery: substitution HaH and early discharge. Substitution HaH admits patients requiring hospital-level care directly to home, usually from the emergency department (ED). Less commonly, patients enrolled in managed and commercial health plans that contract with the HaH program can be admitted from an ambulatory clinic or directly from home. In early discharge HaH, a patient receiving traditional hospital care and who has a continued need is assessed for eligibility and offered HaH. They’re brought home by medical transport, where they receive the same diagnostic and therapeutic services they would have received in the hospital—blood tests, x-rays, ultrasounds, respiratory treatments, and I.V. medications. HaH also includes many of the same integral staff roles necessary to provide hospital-level care, such as physical therapy, occupational therapy, speech therapy, social work, patient care assistants, phlebotomy, and nursing.
HaH skill set
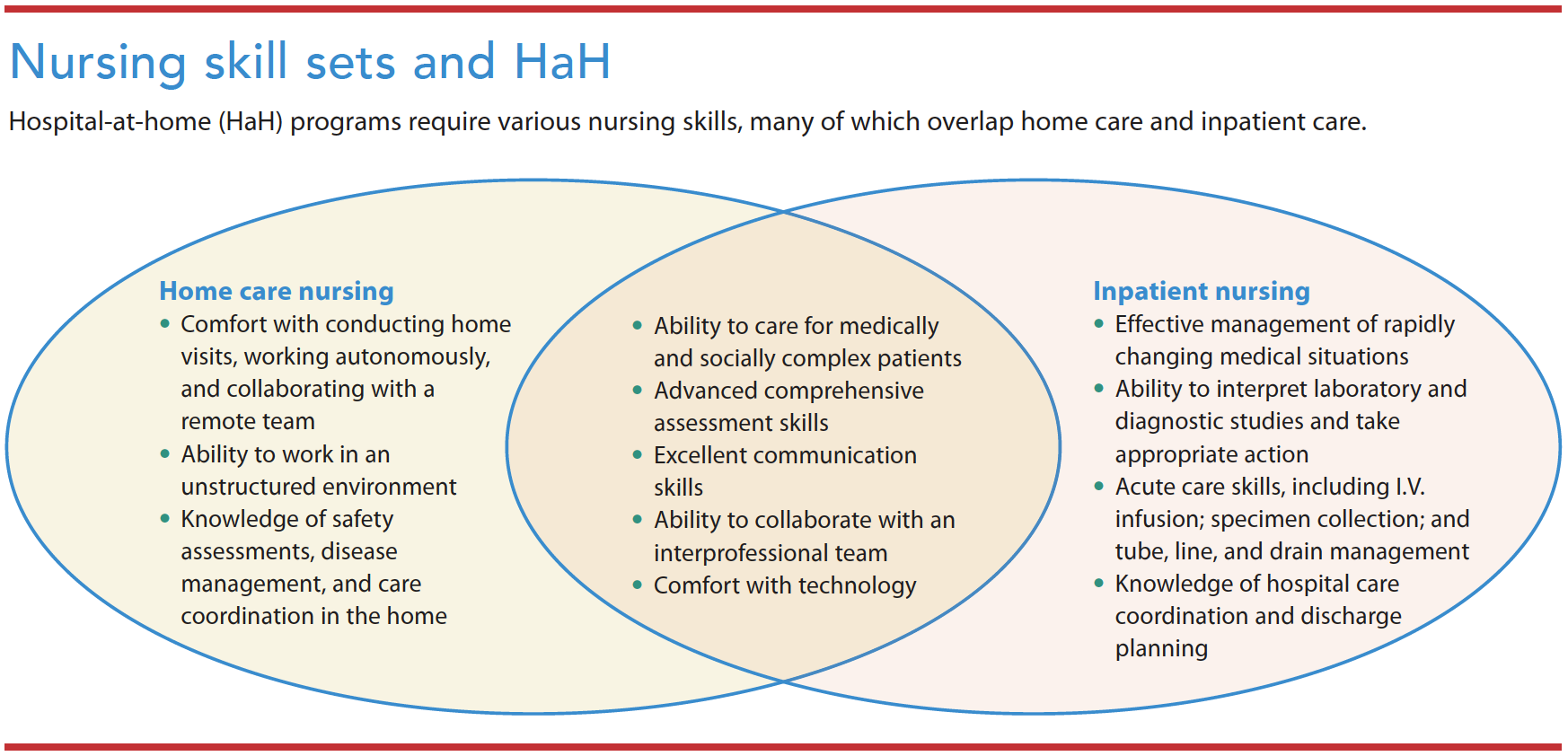
Whatever the program’s staffing structure, success requires strong clinical, technical, and communication skills. Because clinicians make independent home visits, team members must be flexible, adaptable, and comfortable working autonomously in unfamiliar environments. HaH programs’ application of telehealth modalities, remote patient monitoring, Bluetooth-enabled tools, and Wi-Fi or network-connected platforms requires that staff learn how to use and troubleshoot technology. Telehealth relies on HIPAA-compliant chat modalities for team communication, as well as electronic health records. Staff also may implement point-of-care laboratory diagnostics and mobile tech-enabled solutions to dispense medication and document its administration. In addition to communication with the patient, clinicians also must share information with caregivers who want to learn about the treatment plan, program details, and this new care model. (See Nursing skill sets and HaH.)
HaH nursing roles
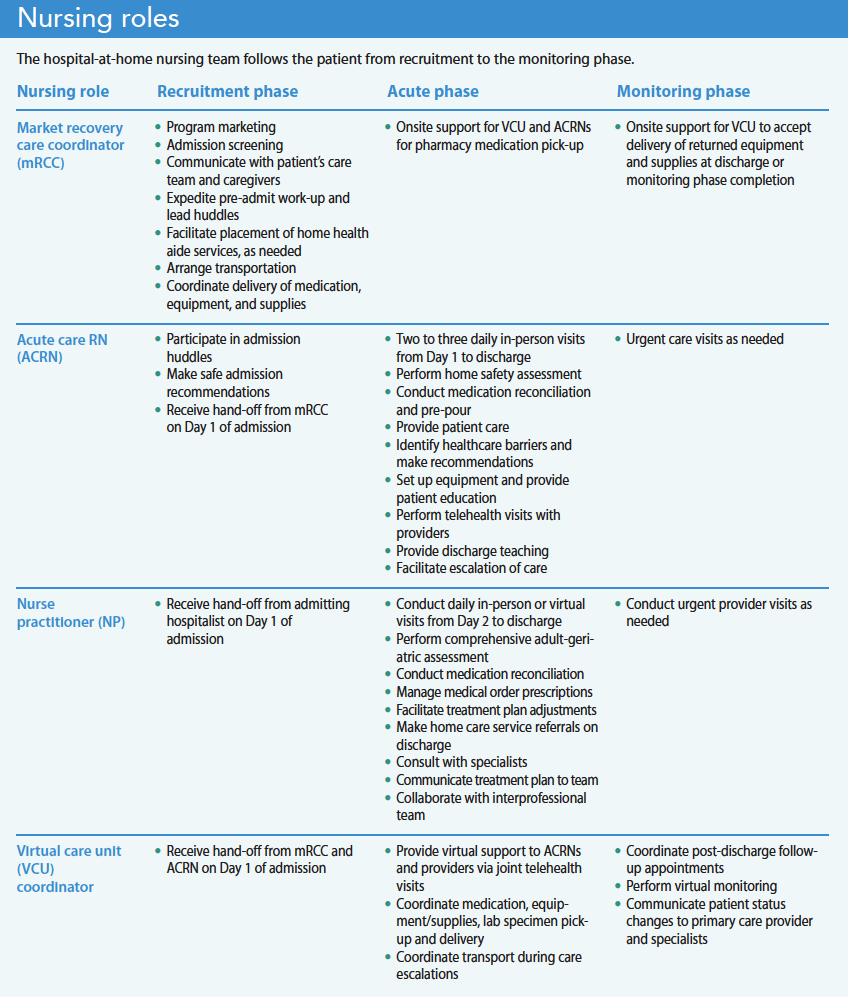
Many HaH nursing teams include market recovery care coordinators (mRCCs), ACRNs, virtual care unit (VCU) coordinators, NPs, and nurse managers with specialized skills and experience in medical-surgical, emergency care, critical care, home care, adult/geriatrics, palliative care, and case management. (Other healthcare organizations may have similar roles with different titles.) The team follows the patient throughout the HaH phases, from recruitment to the acute phase followed by discharge or a monitoring phase. (See Nursing roles.)
Market recovery care coordinators
At Mount Sinai, the mRCC screens and recruits eligible patients and organizes all aspects of the patient’s transfer from the ED or inpatient floor to home. They educate qualified patients, their caregivers, and the ED/inpatient care team about HaH services. Once an interested patient is deemed clinically appropriate, the mRCC collaborates with a care team of hospitalists, nurses, social workers, and case managers to start the HaH admission process. They screen patients at the bedside for home safety concerns using questionnaires and chart reviews, expedite the pre-admission work-up, and lead admission huddles between the ED/inpatient care team and the HaH team.
During the HaH admission process, the mRCC coordinates with hospital social workers and various vendors to facilitate patient care assistant placement, arrange transportation, and coordinate delivery of medication, telehealth equipment, and nursing supplies to the home. Throughout the course of the patient’s HaH stay, the mRCC supports ACRNs and the virtual care team by collecting additional medications and supplies from the hospital pharmacy for delivery to the patient’s home.
Acute care RNs
ACRNs are a group of contracted home health agency nurses specially trained and dedicated to caring for patients in HaH outside of a home health episode of care. At the start of the acute phase, the ACRN arrives at the home within 2 hours of the patient’s arrival to transform it into a hospital room. At this admission visit, the ACRN performs a clinical and safety assessment to ensure patient stability, identifies risk factors that may contribute to a decline in health (such as inadequate caregiver support or food insecurity), and performs a comprehensive medication reconciliation. The ACRN reports clinical changes, home safety concerns requiring escalation back to the traditional hospital, and medication discrepancies to the provider. They also perform patient and family education about the use of telehealth equipment and discharge planning.
The ACRN conducts twice-daily home visits throughout the acute phase to assess the patient’s clinical status, implement nursing orders, and provide ongoing education. Nursing interventions include pre-pouring medication; administrating oral, I.V., and injectable medications; and monitoring patient response to treatment. The ACRN also may manage oxygen, urinary catheters, chest tube drains, wounds, and I.V. access devices.
At follow-up visits, ACRNs arrange telehealth appointments with the patient, provider, and VCU coordinator. During these visits, the ACRN shares assessment findings and electronic stethoscope recordings with the provider to help guide the treatment plan. If a patient shows signs of clinical decompensation, the ACRN collaborates with the provider to schedule a third nursing visit per day, initiate community paramedic visits for advanced diagnostic testing and urgent treatments, or coordinate medical transport or activate 911 to escalate the patient back to the traditional hospital, as clinically appropriate.
During the discharge visit, the ACRN ensures patient readiness and implements discharge orders, including a review of medications, follow-up appointments, and community referrals. For patients eligible for the monitoring phase, ACRNs can conduct urgent visits with patients who can’t seek medical attention at their primary care clinic because of lack of appointment availability.
Virtual care unit coordinators
After acutely ill patients are admitted to HaH, VCU coordinators direct all care management activities. These specialized nursing coordinators offer virtual support to ACRNs and providers during joint telehealth visits, telephone encounters, and electronic communication, such as email and secure chat. Duties during the acute phase include scheduling medication deliveries and following up on orders for oxygen, durable medical equipment, and imaging and diagnostic testing (for example, ECGs and ultrasounds). The VCU coordinator expedites hospital-level consultations from social work and physical therapy, and follows up on patient care assistant placement.
After hours, the VCU coordinator triages urgent patient phone calls and collaborates with on-call physicians to deploy urgent community paramedic visits. In addition, the VCU coordinator, using phone and video visits, periodically follows patients who qualify for the monitoring phase to prevent hospital readmission.
Nurse practitioners
From Day 2 of admission to the HaH program until discharge, the NP manages the patient via in-person and telehealth visits. During the initial home visit, the NP performs a comprehensive adult/geriatric assessment to evaluate the patient’s physical health and identify potential problems that may impact recovery at home, including incontinence issues and cognitive, functional, and sensory impairment. The NP performs a medication reconciliation to evaluate adherence, determine barriers to medication management, and identify inappropriate medications that may lead to confusion, falls, and adverse events. The NP addresses medication discrepancies and updates the HaH treatment plan. The NP also handles caregiver and home safety concerns via orders for urgent durable medical equipment, rehabilitative services, a home health aide, and social work. In addition, the NP orders and reviews pertinent labs and imaging.
If the patient is stable, the NP conducts telehealth visits facilitated by the ACRN and VCU coordinator. For patients with a worsening clinical picture, the NP consults with the attending physician and other specialists, such as infectious disease or pharmacy, to optimize patient care. After patient visits, handoff to the on-call hospitalist occurs during daily clinical huddles where the NP presents pertinent findings along with the assessment and plan.
On discharge, the NP reconciles the outpatient medication list, completes discharge orders, and prescribes medications to the outpatient pharmacy. The NP also orders non-urgent durable medical equipment and home care services for patients with additional needs.
Nurse managers
All nursing teams require a nurse manager. Their responsibilities include recruitment, onboarding, supervision, and staff scheduling. They ensure staff and patient safety by implementing safe home care practices, ensuring adequate supply of personal protective equipment, and assigning patient caseloads according to nurse competency, patient acuity, geography, and visit type.
Responding to patient needs
The nursing team plays a key role in the HaH model and works together to respond to the patient’s acute care needs. The skill sets among coordinators and field clinicians overlap with traditional home health, inpatient nursing roles, and telehealth. As HaH continues to grow, nurses should become familiar with this care model. Hospitals interested in building an HaH program with a robust nursing team should consider participating in the HaH Users Group (hahusersgroup.org) as a helpful resource.
Xiomara M. Dorrejo is a nurse practitioner in the Mount Sinai Health System Hospitalization at Home Program in New York, New York. LaToya Sealy is a nurse practitioner in the Mount Sinai Health System Hospitalization at Home Program. Jennifer Shields is an acute care RN in the Mount Sinai Contessa Health/Amedisys Hospitalization at Home Program. Pamela Saenger is a lead provider in the Mount Sinai Health System Hospitalization at Home Program. Katherine A. Ornstein is the director of research at the Icahn School of Medicine at Mount Sinai. Linda V. DeCherrie is a professor in the department of geriatric and palliative medicine at the Icahn School of Medicine at Mount Sinai.
Key words
hospital at home, acute hospital care at home, acute care nursing, nursing roles
American Nurse Journal. 2022; 17(12). Doi: 10.51256/ANJ122216
References
American Nurses Association. Home Health Nursing: Scope and Standards of Practice. 2nd ed. Silver Spring, MD: American Nurses Association; 2014.
Brown CJ. After three decades of study, hospital-associated disability remains a common problem. J Am Geriatr Soc. 2020;68(3):465-6. doi:10.1111/jgs.16349
Caplan GA, Sulaiman NS, Mangin DA, Aimonino Ricauda N, Wilson AD, Barclay L. A meta-analysis of “hospital in the home.” Med J Aust. 2012;197(9):512-9. doi:10.5694/mja12.10480
Centers for Medicare & Medicaid Services. Acute hospital at home care at home resources. September 30, 2022. qualitynet.cms.gov/acute-hospital-care-at-home/resources
Federman AD, Soones T, DeCherrie LV, Leff B, Siu AL. Association of a bundled hospital-at-home and 30-day postacute transitional care program with clinical outcomes and patient experiences. JAMA Intern Med. 2018;178(8):1033-40. doi:10.1001/jamainternmed.2018.2562
Gonçalves-Bradley DC, Iliffe S, Doll HA, et al. Early discharge hospital at home. Cochrane Database Syst Rev. 2017;6(6):CD000356. doi:10.1002/14651858.CD000356.pub4
Hayashi JL, Leff B. Geriatric Home-Based Medical Care: Principles and Practice. New York, NY: Springer; 2016.
Heller DJ, Ornstein KA, DeCherrie LV, et al. Adapting a hospital-at-home care model to respond to New York City’s COVID-19 crisis. J Am Geriatr Soc. 2020;68(9):1915-6. doi:10.1111/jgs.16725
Hospital at Home Users Group. About the users group. hahusersgroup.org/about-the-users-group/
Leff B, Burton L, Guido S, Greenough WB, Steinwachs D, Burton JR. Home hospital program: A pilot study. J Am Geriatr Soc. 1999;47(6):697-702. doi:10.1111/j.1532-5415.1999.tb01592.x
Leff B, Burton L, Mader SL, et al. Hospital at home: Feasibility and outcomes of a program to provide hospital-level care at home for acutely ill older patients. Ann Intern Med. 2005;143(11):798-808. doi:10.7326/0003-4819-143-11-200512060-00008
Levine DM, Mitchell H, Rosario N, et al. Acute care at home during the COVID-19 pandemic surge in Boston. J Gen Intern Med. 2021;36(11):3644-6. doi:10.1007/s11606-021-07052-5
Levine DM, Ouchi K, Blanchfield B, et al. Hospital-level care at home for acutely ill adults: A randomized controlled trial. Ann Intern Med. 2020;172(2):77-85. doi:10.7326/M19-0600
Mooney K, Titchener K, Haaland B, et al. Evaluation of oncology hospital at home: Unplanned health care utilization and costs in the Huntsman at home real-world trial. J Clin Oncol. 2021;39(23):2586-93. doi:10.1200/jco.20.03609
Shepperd S, Iliffe S, Doll HA, et al. Admission avoidance hospital at home. Cochrane Database Syst Rev. 2016;9(9):CD007491. doi:10.1002/14651858.cd007491.pub2


















