
Prevent exacerbation and hospitalization.
- The rising incidence of heart failure in the United States carries a significant disease burden, has a high economic impact, and increases healthcare resource use.
- Palliative care can help reduce heart failure exacerbation and readmission.
- Nursing’s role in palliative care for patients with heart failure include symptom management in conjunction with patient education and interventions aimed at reducing disease exacerbation.
According to the World Health Organization (WHO), cardiovascular disease remains the number one cause of morbidity and mortality worldwide. Globally, heart failure (HF) affects more than 64 million people, and the increasing incidence in the United States carries a significant disease burden, has a high economic impact, and increases healthcare resource use. The individual annual costs of care for patients with HF in the United States is over $30,000, primarily a result of exacerbation that requires hospitalization. Estimates predict that the costs of HF, the primary diagnosis in hospitalized U.S. patients 65 years and older, will exceed $70 billion by 2030. (See HF by the numbers.)
HF by the numbers
In the United States, the incidence of heart failure (HF) continues to increase:
- HF accounts for over 11 million provider visits annually and is responsible for more hospitalizations than from all cancers combined.
- Despite an increased focus on decreasing HF-related readmission rates, few interventions have proven successful.
- Medicare beneficiaries with HF have higher hospital readmission rates than those with any medical condition.
- Of the 1 million hospitalizations annually, more than half of patients are readmitted as a result of exacerbation and 30% die within 1 year.
- According to the Centers for Disease Control and Prevention, 6.9 million Americans are living with HF, and this is expected to increase by 24% to nearly 8.5 million in 2030.
- Currently, over 870,000 new cases of HF are diagnosed annually.
- HF affects patients of all ages and occurs equally in men and women.
- HF among the Black population is 1.5 times more likely compared with the White population.
- Approximately 1.4 million patients diagnosed with HF are under 60 years of age.
- Patients newly diagnosed with HF can expect to live an average of 5 years.
- HF contributes to 695,000 deaths in the United States annually (1 in every 4 deaths).
- Sudden death can occur in patients with HF at a 6 to 9 times greater rate than the general population.
HF causes and risk factors
HF results from conditions, comorbidities, and risk factors that impair ventricular filling and the ejection of blood into systemic circulation.
- Arrythmia
- Cardiomyopathy
- Chronic obstructive pulmonary disease
- Coronary heart disease
- Diabetes
- Hypertension
- Obesity
- Sleep apnea
- Age ≥65 years
- Cocaine or illegal drugs
- Family history
- Heavy alcohol use
- Lack of physical activity
- Smoking
- Stress
- Unhealthy diet
*HF risk increases with one or more of these factors; list is not all inclusive.
Palliative care plays a role in reducing exacerbation and therefore readmission. Understanding HF, including its pathophysiology, its classifications, and how it develops can aid palliative treatment. Nurses play a critical role in this care.
Clinical overview
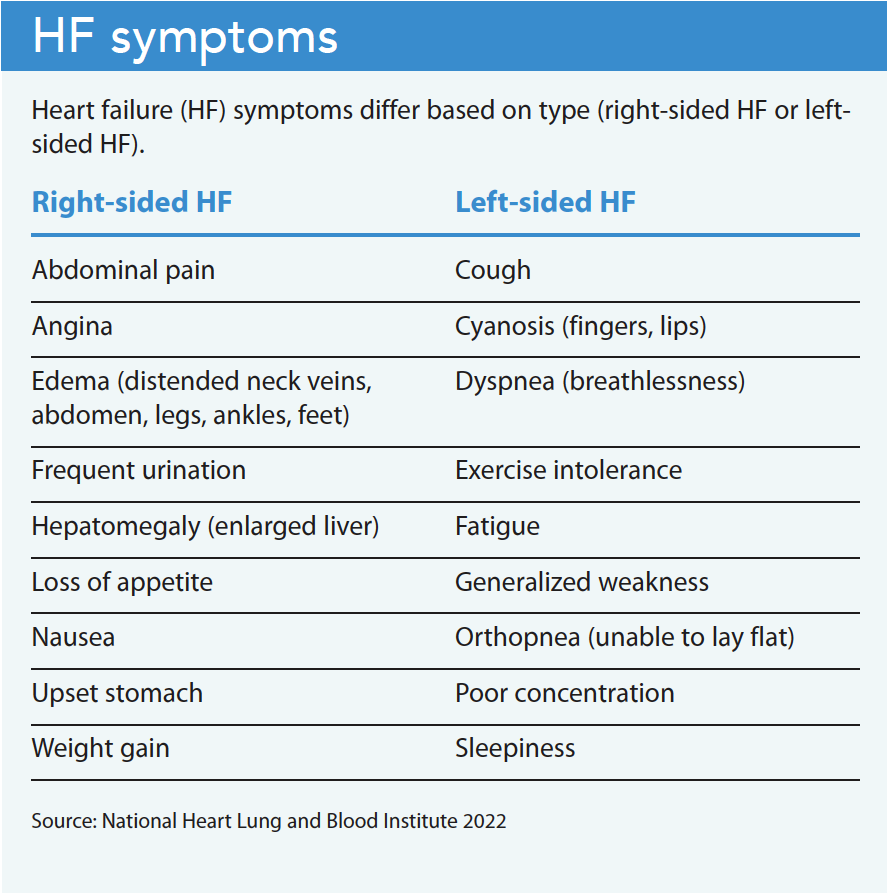
HF, which can affect one or both sides of the heart, prevents the heart from adequately filling with blood or pumping effectively to meet the metabolic demands of the body. It can occur acutely or over time from a chronic underlying condition. Left-sided HF, the most common type, prevents the heart from pumping enough oxygenated blood throughout the body. Right-sided HF prevents the heart from pumping enough blood into the lungs for oxygenation. Eventually, the heart becomes weakened, stiff, and thickened, and fluid can back-up into the lungs and peripheral body (legs, ankles, feet).
HF severely decreases functional capacity and increases mortality risk. Patients frequently experience fatigue, dyspnea, reduced exercise tolerance, and fluid retention (pulmonary and peripheral edema). HF also can damage the liver and kidneys. Other serious complications include pulmonary hypertension, cor pulmonale, arrythmia, heart valve disease, and sudden cardiac arrest. HF, an advanced condition, can’t be cured or reversed. Many patients experience disease exacerbation (uncontrolled symptoms), hospitalization, debility, and worsening of their underlying condition. (See HF symptoms.)
HF classification
In 2020, members of the Heart Failure Society of America, the Heart Failure Association of the European Society of Cardiology, and the Japanese Heart Failure Society, along with 14 countries and six continents authored and agreed on a consensus document, the Universal Definition and Classification of HF. This document provides a standardized understanding of HF as a clinical syndrome with associated symptoms caused by structural and functional cardiac abnormality. The document identifies four specific HF stages: At risk for HF (Stage A), pre‐HF (Stage B), symptomatic HF (Stage C), and advanced HF (Stage D).
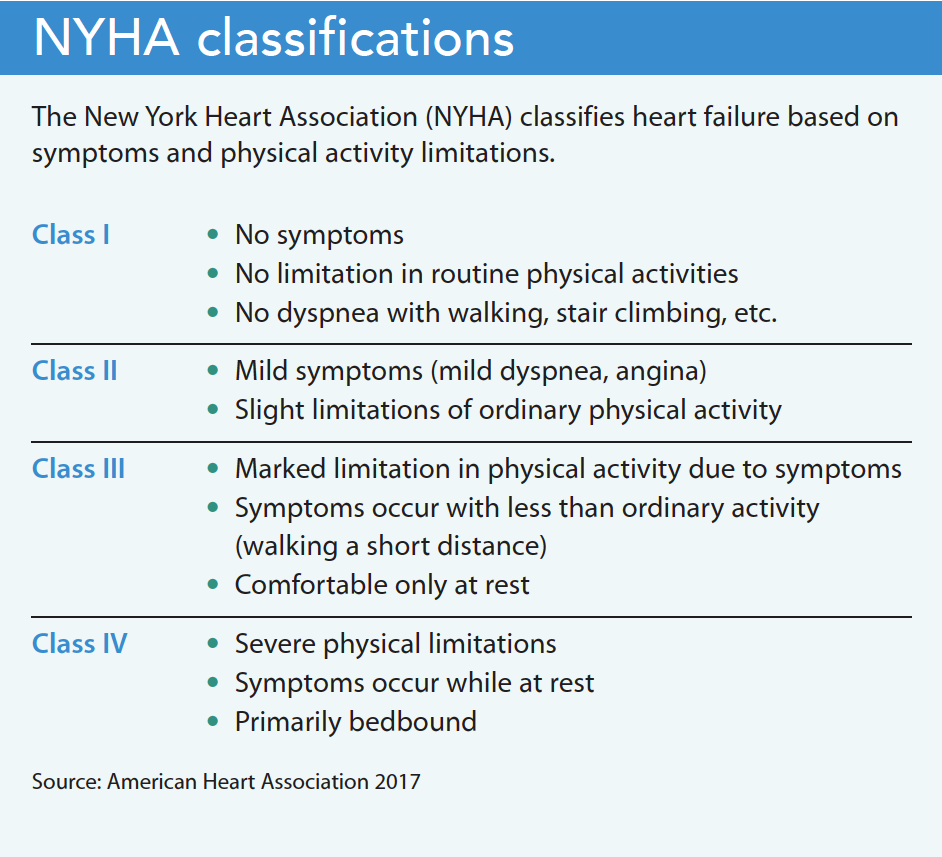
Many clinicians also use the New York Heart Association (NYHA) classification for HF. These two classification systems correlate with pre- and post-HF diagnosis and provide a prognostic indicator for initiating palliative interventions. (See NYHA classifications.)
HF diagnosis
A combination of diagnostics, patient-reported symptoms, and findings from a comprehensive physical examination helps to establish HF type. The presence (or absence) of symptoms is considered fundamental in characterizing disease progression and severity. Diagnostics comprise laboratory analysis, radiologic findings, and heart conduction evaluation.
Laboratory analysis
Common laboratory analysis plays an important role in risk assessment, diagnosis, prognosis, and monitoring. It includes complete blood count, comprehensive metabolic panel, and a thyroid panel. Natriuretic peptide tests (brain natriuretic peptides [BNP] and N-terminal-proBNP) also can aid diagnosis, with elevated findings supporting an HF finding. However, controversy exists over the specificity of natriuretic peptides due to medication sensitivity. For example, beta blockers, diuretics, angiotensin-converting enzyme inhibitors (ACEI), and angiotensin II receptor blockers can decrease natriuretic peptide levels, as can obesity. Providers also may test cardiac troponins in patients with suspected acute or chronic HF.
Radiologic analysis
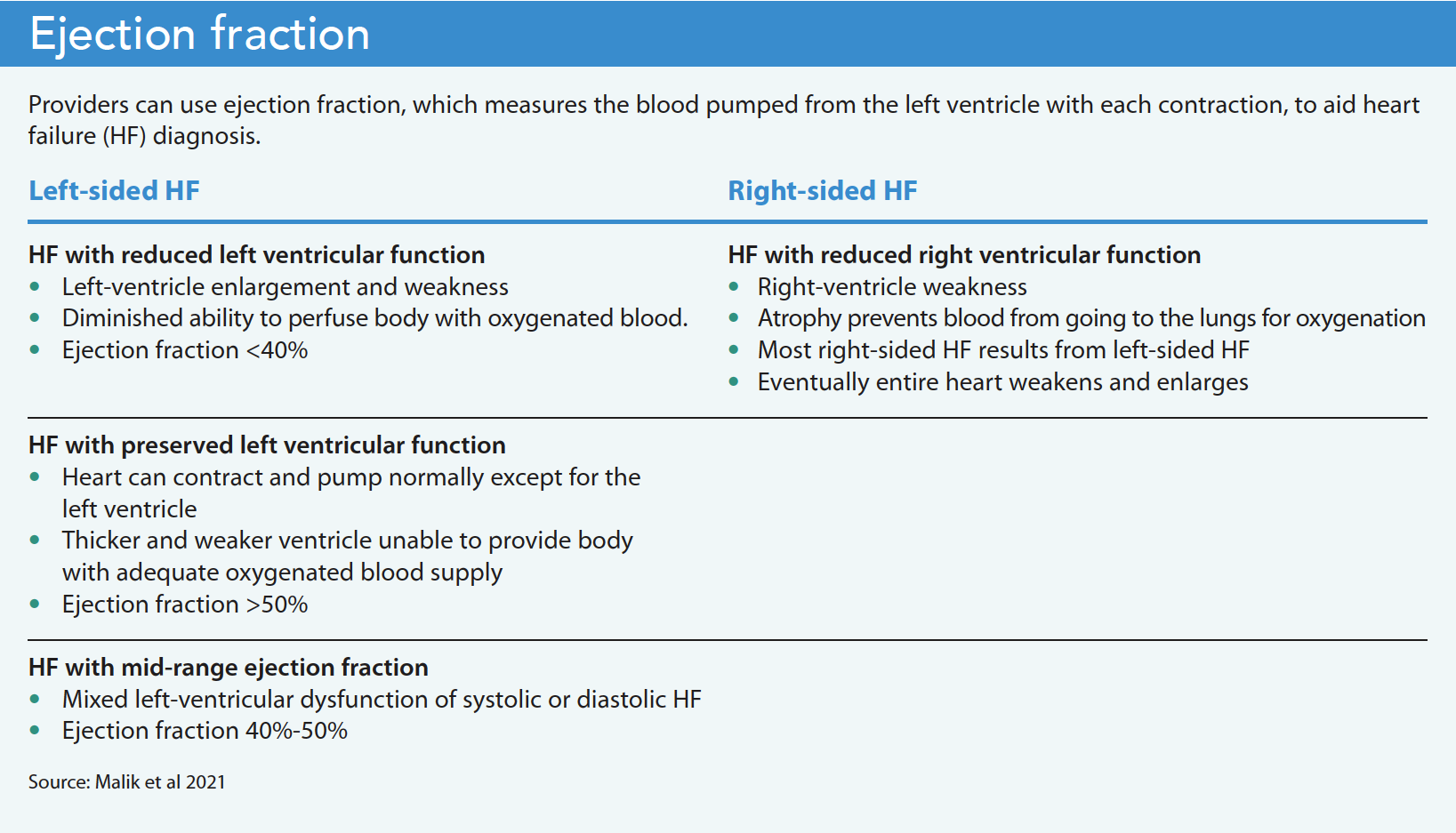
A joint report by the American College of Radiology and the American College of Cardiology Foundation makes the strongest recommendation for the use of two-dimensional doppler electrocardiography to confirm a new diagnosis of HF. Electrocardiography helps to determine the systolic and diastolic performance of the left ventricle (LV), cardiac output (ejection fraction [EF]), and pulmonary artery and ventricular filling pressures. EF measures the percentage of blood pumped from the left ventricle with each contraction. Normal EF is between 50% and 70%. An EF under 40% indicates left ventricular HF. This simple and noninvasive imaging is inadequate in 8% to 10% of cases and difficult to evaluate in patients with lung disease. (See Ejection fraction.)
Chest radiographs can help evaluate heart size and reveal pulmonary hypertension or pleural effusions. In some cases, multichannel computed tomography scanning can reveal pulmonary edema or valvular abnormalities. Magnetic resonance imaging provides similar information.
Additional diagnostics include electrocardiogram to evaluate heart conduction and angiography (catheterization).
Palliative care and HF
Each escalation in HF symptoms that results in an exacerbation and hospitalization can lead to reduced cardiac capacity, increased debility, and progressively worsened quality of life. Implementing symptom management or palliative care (PC) at the onset of a new diagnosis of HF as a non-curable chronic condition (Stage C, NYHA Class III) can help manage symptoms to reduce disease exacerbation and hospitalization.
PC, initially established as the interprofessional care and management of patients with cancer, has expanded to include patients without cancer but who have other advanced chronic conditions. However, limited evidence exists related to the effectiveness of PC in patients with HF. Most PC models in the United States and the Medicare hospice benefit were designed for cancer patients, whose prognosis is more specific (a short decline in physical function until death) than patients with HF. The disease trajectory for HF tends toward a gradual decline in physical function with intermittent serious episodes of exacerbation and recovery.
In addition, palliative medications frequently used to manage symptoms in patients with cancer aren’t always appropriate for managing HF symptoms. For example, patients with HF are sensitive to opioids and benzodiazepines because of compromised heart, lung, and kidney function that interferes with metabolism and excretion. In 2016, the Food and Drug Administration (FDA) issued a black box warning for this drug combination. Providers should use caution in patients with HF who have a prognosis greater than 6 months.
Nursing implications
Cardiac symptom management or PC initiated at the onset of a new HF diagnosis and implemented throughout the disease trajectory can reduce exacerbation. A recent systematic review evaluated 75 clinical trials representing 95,444 patients with HF and reduced EF. Researchers found an aggregate combination of ACEI, BB, mineralocorticoid receptor agonists, and sodium glucose cotransporter-2 inhibitors as most effective at reducing hospital admission.
Medication adherence requires nurses to participate in shared decision making with the patient and family. Palliative interventions that can help prevent disease exacerbation include ongoing assessments and evaluations of fluid retention, lung sounds, weight, blood pressure, heart rate, and the patient’s ability to perform activities of daily living without fatigue or dyspnea.
Engaging the patient, family, and caregiver in self-management practices can aid prompt identification of early signs and symptoms of an exacerbation. The nurse who recognizes escalating symptoms or cardiac abnormalities can proactively recruit interprofessional support to prevent escalation and hospitalization.
Kim Kuebler is the director and founder of Multiple Chronic Conditions Resource Center in Darien, Georgia.
Key words:
Palliative care, heart failure, exacerbation prevention, medication adherence, patient education
American Nurse Journal. 2022; 17(12). Doi: 10.51256/ANJ122228
References
American Heart Association. Classes of heart failure. Updated May 31, 2017. heart.org/en/health-topics/heart-failure/what-is-heart-failure/classes-of-heart-failure
American Heart Association. Ejection fraction heart failure measurement. May 31, 2017. heart.org/en/health-topics/heart-failure/diagnosing-heart-failure/ejection-fraction-heart-failure-measurement
American Heart Association. Heart failure signs and symptoms. May 31, 2017. heart.org/en/health-topics/heart-failure/warning-signs-of-heart-failure
Centers for Disease Control and Prevention. Heart failure. Updated October 14, 2022. cdc.gov/heartdisease/heart_failure.htm
Chang YK, Kaplan H, Geng Y, et al. Referral to palliative care for patients with heart failure: A systematic review. Circ Heart Fail, 2020;13(9):e006881. doi:10.1161/CIRCHEARTFAILURE.120.006881
Food and Drug Administration. FDA warns about serious risks and death when combining opioid pain or cough medicines with benzodiazepines; requires its strongest warning. Updated January 19, 2022. https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-fda-warns-about-serious-risks-and-death-when-combining-opioid-pain-or
Genzen JR. Heart failure. ARUB Laboratories. January 2021. arupconsult.com/content/heart-failure
Gibson G, Blummer V, Mentz RJ, Lala A. Universal definition and classification of heart failure: A step in the right direction. American College of Cardiology. July 13, 2021. www.acc.org/latest-in-cardiology/articles/2021/07/12/12/31/universal-definition-and-classification-of-heart-failure
Malik A, Brito D, Vagar S, Chhabra L. Congestive heart failure. StatPearls. January 2022. pubmed.ncbi.nlm.nih.gov/28613623
Mayo Clinic. Heart failure. mayoclinic.org/diseases-conditions/heart-failure/symptoms-causes/syc-20373142?p=1
National Heart, Lung, and Blood Institute. What is heart failure? March 24, 2022. nhlbi.nih.gov/health/heart-failure
National Institute on Aging. What is heart failure? June 1, 2018. nia.nih.gov/health/what-heart-failure
Patel J. Heart failure population health considerations. Am J Manag Care. 2022;27(9 suppl):S191-5. doi:10.37765/ajmc.2021.88673
QuickStats. Age-adjusted death rates from heart disease among adults aged 45-64 years by urbanization level and sex—National Vital Statistics System, United States, 2019. MMWR Morb Mortal Wkly Rep. 2021;70(46):1621. doi:10.15585/mmwr.mm7046a8
Singh VN, Lin EC. Congestive heart failure imaging. Medscape. August 29, 2022. emedicine.medscape.com/article/354666-overview
Takaoka Y, Hamatani Y, Shibata T. et al. Quality indicators of palliative care for cardiovascular intensive care. J Intensive Care. 2022;10(1):15. doi:10.1186/s40560-022-00607-6
Teuteberg JJ, Teuteberg WG. Palliative care for patients with heart failure. American College of Cardiology. February 11, 2016. www.acc.org/latest-in-cardiology/articles/2016/02/11/08/02/palliative-care-for-patients-with-heart-failure
Tromp J, Ouwerkerk W, van Veldhuisen DJ, et al. Systematic review and network meta-analysis of pharmacological treatment of heart failure with reduced ejection fraction. JACC Heart Fail. 2022:10(2):73-84. doi:10.1016/j.jchf.2021.09.004
Urbich M, Globe G, Pantiri K. et al. A systematic review of medical costs associated with heart failure in the USA (2014-2020). Pharmacoeconomics. 2020;38(11):1219-36. doi:10.1007/s40273-020-00952-0
von Schwarz E, He M, Bharadwaj P. Palliative care issues for patients with heart failure. JAMA Network Open. 2020;3(2):e200011. doi:10.1001/jamanetworkopen.2020.0011
Wiskar K, Toma M, Rush B. Palliative care in heart failure. Trends Cardiovasc Med. 2018;28(7):445-50. doi:10.1016/j.tcm.2018.02.008
Woodruff Health Sciences Center. Emory’s heart failure toolbox. 2009. whsc.emory.edu/home/publications/health-sciences/emory-health/fall09/heart-failure-toolbox.html
Woods M, Kuebler K. Cardiovascular disease. In: Kuebler K, ed. Integration of Palliative Care in Chronic Conditions: An Interdisciplinary Approach. Pittsburgh, PA: Oncology Nursing Society; 2017; 125-40.
World Health Organization. Cardiovascular disease mortality rate (per 100 000 population). who.int/data/gho/indicator-metadata-registry/imr-details/3152


















