Jim Murphy, age 70, is admitted to the medical unit. His renal function has declined over the last few months due to chronic hypertension. The nephrologist inserts a temporary dialysis catheter into his right subclavian vein and writes orders for a chest X-ray and dialysis.
History and assessment hints
On entering the room, you note Mr. Murphy seems anxious, restless, and in distress. He states he is having chest pain and difficulty breathing. You assess his vital signs at once: blood pressure 150/90 mm Hg, heart rate 120 beats/minute, respiratory rate 28 breaths/minute, and oxygen saturation 89%. He reports feeling a sudden stabbing pain in his right side, which worsens on inspiration.
A quick physical examination reveals decreased breath sounds on the right side, as well as decreased chest expansion on that side with hyperresonance on percussion. Suspecting a pneumothorax, you call the rapid response team (RRT). You support Mr. Murphy’s airway, breathing, and circulation; elevate the head of his bed; attach a portable electrocardiographic monitor; and start a peripheral I.V. line.
On the scene
When the RRT arrives, you summarize the patient’s history, vital signs, and recent dialysis catheter insertion. The team suspects a pneumothorax caused by the catheter insertion, and orders a STAT portable chest X-ray, 4 L oxygen by nasal cannula, and arterial blood gas (ABG) tests. Anticipating the need for immediate chest-tube insertion, they call the team physician.
A pneumothorax occurs when air enters the pleural space through a hole in the chest or pleura. This disrupts the normally negative pleural pressure inside the chest, causing partial or total lung collapse. In Mr. Murphy’s case, the most likely cause was a hole in the pleura resulting from dialysis catheter insertion.
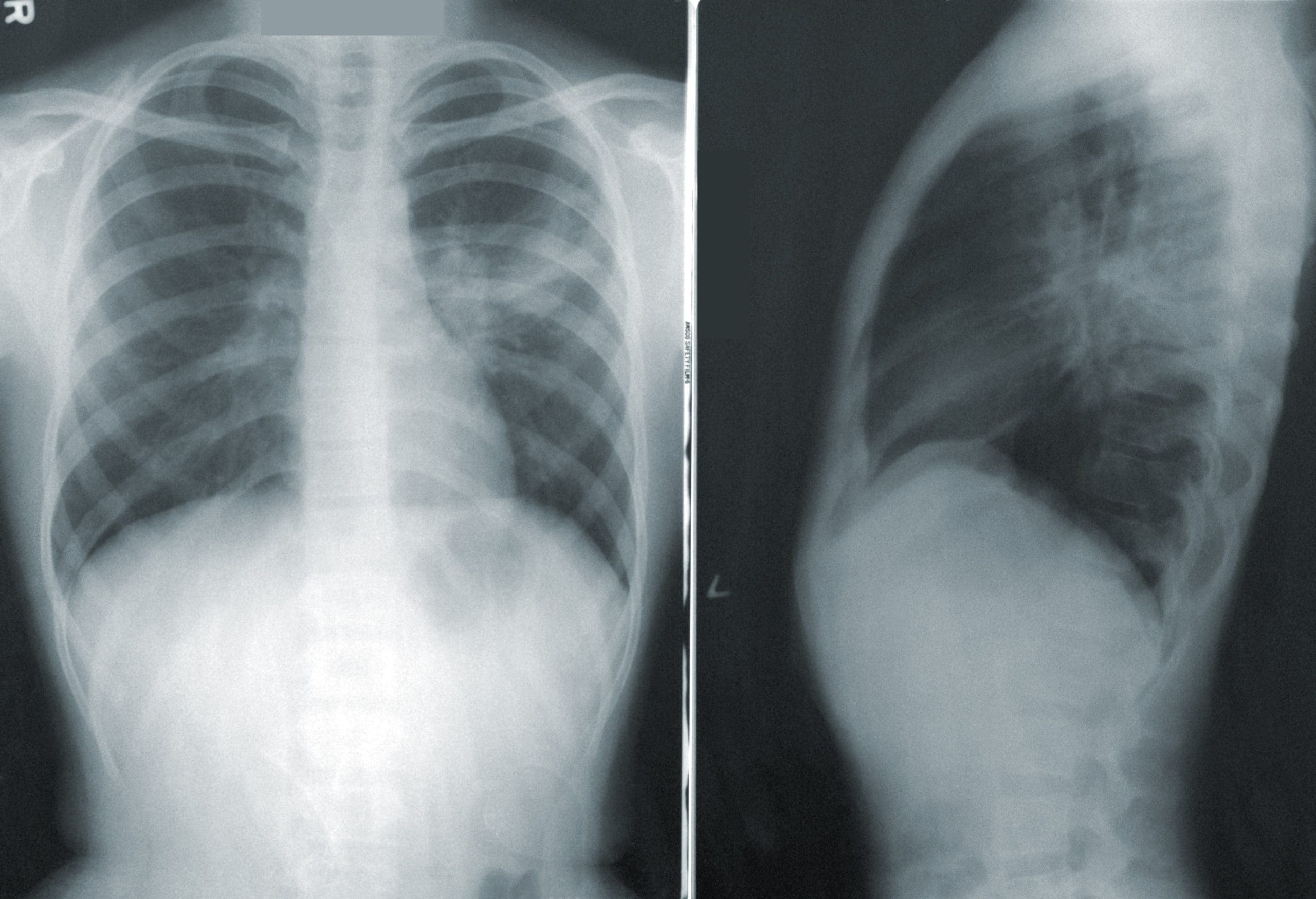
The X-ray reveals a 50% pneumothorax of the right lung. ABGs show respiratory alkalosis, reflecting decreased PaCO2 stemming from tachypnea and slight hypoxia. When the physician arrives, you and the RRT are ready for chest-tube insertion. You explain the procedure to Mr. Murphy, give analgesia, and offer support. Within a few minutes after tube insertion, his vital signs return to baseline, his oxygen saturation is 98%, and his breathing eases. A repeat X-ray shows the chest tube is placed correctly and the pneumothorax is resolving.
Outcome
You continue to monitor Mr. Murphy’s vital signs and breath sounds and maintain chest-tube patency. Because the tube was placed for a pneumothorax rather than fluid drainage, it’s set on water seal alone, using a Pleurovac closed-drainage system. This should help restore negative pressure and remove pleural-space air. You keep the drainage unit at least 1′ below the insertion site to maintain chest pressure higher than drainage system pressure; you also take steps to prevent tubing kinks and maintain the water seal. You encourage Mr. Murphy to take frequent deep breaths and notify you if he grows short of breath.
That evening, he is able to have his first dialysis treatment. The pneumothorax resolves fully within 2 days and the chest tube is removed. The day after removal, Mr. Murphy is discharged home.
Education and follow-up
Mr. Murphy’s respiratory distress stemmed from collapse of 50% of his lung. The incidence of pneumothorax associated with central venous catheter insertion is 2% to 16%. If a pneumothorax goes untreated, air can continue to accumulate in the lung, causing a rise in pleural pressure that can lead to a tension pneumothorax. This type of pneumothorax may reduce lung expansion, venous return, and cardiac output, which may lead to cardiac arrest.
Early recognition and treatment of a pneumothorax are essential to prevent its progression to a tension pneumothorax. For Mr. Murphy, quick detection and interventions averted a potentially catastrophe.
Visit www.AmericanNurseToday.com/Archives.aspx for a list of selected references.
Cindy Ruiz is a critical care clinical nurse specialist at Northwest Community Hospital in Arlington Heights, Illinois.

















