Nurses’ role in prevention and management
- Urinary tract infection (UTI remains an epidemiologically important infection across all healthcare settings.
- Prevention of healthcare-associated UTI is a nursing-sensitive quality measure.
- Implementation of an evidence-based protocol helps to reduce the prevalence of catheter-associated UTIs.
Learning Objectives
- Explain urinary tract infection (UTI) pathophysiology and risk factors.
- Describe UTI diagnostic criteria, the catheter-associated urinary tract infection (CAUTI) prevention bundle, and treatments for UTI.
- Describe nursing implications related to UTI prevention for all patients.
The author, planners, and peer reviewers of this CNE activity have disclosed no relevant financial relationships with any commercial companies pertaining to this activity. See the last page of the article to learn how to earn CNE credit.
Expiration: 12/1/26
Sandra Long*, a 72-year-old woman, is admitted to the emergency department from a long-term care facility for fever, poor oral intake, new-onset confusion, foul-smelling urine, and incontinence. She has a history of type 2 diabetes, hypertension, coronary artery disease, and mild cognitive impairment.
Urinary tract infection (UTI) continues to attract clinical attention as one of the world’s most prevalent infections. UTI broadly describes several clinical conditions, including cystitis, pyelonephritis, and renal or perinephric abscess. UTIs are the fifth most common type of healthcare-associated infection (HAI) reported to the Centers for Disease Control and Prevention (CDC) for tracking. The National Healthcare Safety Network estimates that 75% of healthcare-associated UTIs are related to urinary catheterization. As a nursing-sensitive quality indicator, the prevention and management of healthcare-associated UTIs rely on evidence-based, high-quality nursing care. (See UTI risk factors.)
UTI risk factors
According to Medina and colleagues, urinary tract infection (UTI) is more common in women than in men, with up to 60% lifetime incidence and increasing prevalence with advancing age. Other risk factors include the following:
- Benign prostatic hyperplasia
- Congenital abnormalities of the urinary tract
- Diaphragm use for birth control
- Frailty
- Immunosuppression
- Incontinence
- Pregnancy
- Sexual activity
- Sexually transmitted infections
- Urinary calculi
- Urinary procedures such as a cystoscopy
Pathophysiology
Pathogens typically enter the bladder through the urethra. Urinary instrumentation presents high risk for introducing infectious agents into the urinary track. Sexual intercourse also may promote migration of genitourinary and bowel flora into the bladder. Shorter female urethras make it easier for infectious agents to gain a foothold in the bladder. More alkaline urine pH creates a more favorable environment for bacterial growth. In addition, adhesins on uropathogens allow them to attach to the uroepithelium.
Uncomplicated UTIs have localized symptoms of cystitis such as dysuria, urinary frequency, and urgency among nonpregnant persons. Patients with uncomplicated UTIs have no functional or anatomical abnormalities in the urinary tract, their kidney function is intact, and they have no risk for serious issues. Complicated UTIs (such as pyelonephritis) may be associated with resistant organisms. They have a higher risk of treatment failure and require a longer treatment course.
According to Medina and colleagues, Escherichia coli accounts for 75% of uncomplicated UTI and 65% of complicated UTI. Other infectious agents associated with UTI include Klebsiella pneumoniae, Staphylococcus saprophyticus, Enterococcus spp., Group B Streptococcus, Proteus mirabilis, Pseudomonas aeruginosa, Staphylococcus aureus, and Candida spp.
The typical incubation period for UTI is 3 to 8 days. The patient will experience at least one of the following symptoms: fever (>100.4°F [>38°C]), dysuria, urinary frequency, and urinary urgency. They also may experience suprapubic and costovertebral angle pain or tenderness with no other recognized etiology. Some patients may experience hematuria, nocturia, cloudy foul-smelling urine, and chills. Older adults with UTI may have vague symptoms such as low-grade fever, lethargy, and confusion, which also may indicate concurrent infections, such as pneumonia. Clinicians should consider nonpathogenic causes of altered mental status such as adverse reactions to medication, fluid and electrolyte imbalances, and neuroendocrine abnormalities.
Diagnostic markers
During an office visit, a dipstick urinalysis can provide rapid screening, but a negative result doesn’t rule out UTI. The provider also should consider clinical presentation, urinalysis, and urine culture and sensitivity. A urine sample positive for leukocyte esterase and nitrates provides evidence for a working diagnosis of UTI. Nitrites signal the presence of enzymes from gram-negative bacteria such as E. coli, which converts nitrates to nitrites. Urine turbidity, sediments, and odor don’t reliably correlate with the presence of infection, and aren’t in themselves symptoms of UTI.
The provider also can make a UTI diagnosis if the patient has systemic or localized symptoms, pyuria, bacteriuria, and a positive urine culture. In the acute care setting, a clean-catch urinalysis sample is preferred for UTI diagnosis.
Initial treatment of uncomplicated UTI doesn’t require a urine culture. Older adults with UTI might have atypical presentations. New onset incontinence and acute mental status changes warrant closer evaluation.
Catheter-associated UTI
In the inpatient setting, catheter-associated UTI (CAUTI) can result from an indwelling urinary catheter (IUC) that’s been in place for more than 2 days. The day of insertion counts as Day 1. In the inpatient setting, if an IUC is in place for more than 2 consecutive days and then removed, the date of discontinuation or the day after is considered the date of event for the UTI to be considered a CAUTI. For patients admitted to a facility with an IUC already in place, the admission date counts as catheter Day 1.
In 2020, according to the CDC, 19,738 CAUTIs were reported. Hospitals report CAUTIs using the standardized infection ratio (SIR). An SIR >1.0 means that more CAUTIs were observed than predicted; an SIR <1.0 indicates that fewer CAUTIs were observed than predicted. In the United States, the number of CAUTIs decreased by 25% from 2015 to early 2020. However, the COVID-19 pandemic may have contributed to a notable increase in CAUTIs in the latter half of 2020. According to Weiner-Lastinger, compared with 2019 data (0.69 SIR), the SIR for CAUTI steadily increased throughout 2020, ranging from 0.59 to 0.82.
Risk factors associated with CAUTI include long hospital stays, multi-morbidities and higher acuity levels (for example, intensive care unit stays), and long catheter duration. Paraplegia, stroke, and female sex also are associated with increased risk for CAUTI.
Peng and colleagues reported that gram-negative bacteria are the most common pathogen (47.46%) for CAUTI in the ICU; Escherichia species account for 23.41% of cases. The same study found fungi caused 27.81% of cases and gram-positive bacteria caused 19.06%. CAUTI is the most common HAI. Frontline nurse vigilance can aid prompt diagnosis. (See Symptomatic CAUTI diagnostic criteria.)
Symptomatic CAUTI diagnostic criteria
Catheter-associated urinary tract infection (CAUTI) diagnosis requires that the following three elements be met:
Element 1
Patient had an indwelling urinary catheter (IUC) in place for more than 2 consecutive days in an inpatient location on the date of event AND was either
- Present for any portion of the calendar day on the date of event
OR
- Removed the day before the date of event
Element 2
Patient has at least one of the following signs or symptoms:
- Costovertebral angle pain or tenderness
- Dysuria*
- Fever (>38°C)
- Suprapubic tenderness
- Urinary frequency*
- Urinary urgency*
Element 3
Patient has a urine culture with no more than two species of organisms identified, at least one of which is a bacterium of ≥105 CFU/mL. (All elements of the symptomatic UTI criterion must occur during the infection window period.)
*An indwelling catheter can cause these symptoms, so they can’t be used for diagnostic purposes when it’s in place.
Source: 2023 National Healthcare Safety Network (NHSN) UTI Checklist cdc.gov/nhsn/pdfs/checklists/uti-checklist-508.pdf
CAUTI prevention bundle
For decades, the CAUTI prevention bundle has proven effective at reducing these HAIs. A large retrospective study by Gould and colleagues reported a greater than one-third reduction with CAUTI bundle implementation. Using evidence-based strategies such as the Comprehensive Unit-based Safety Program (ahrq.gov/hai/tools/cauti-hospitals/index.html), interprofessional teams can significantly aid CAUTI prevention. (See CAUTI bundle.)
CAUTI bundle
The catheter-associated urinary tract infection (CAUTI) bundle, developed by the Healthcare Infection Control Practices Advisory Committee, includes the following:
Appropriate catheter use
When developing the care plan, consider comorbid conditions, such as frailty and dementia.
- Insert catheters only for appropriate indications.
- Use the smallest bore catheter possible.
- Avoid using catheters to manage incontinence.
- Review catheter necessity daily (for example, audit by nurse manager).
- Remove the catheter as soon as possible postoperatively (within 24 hours) unless appropriate indications exist for continued use.
- Use external catheters as alternatives to indwelling urinary catheters.
- To reduce unnecessary catheterization, assess urine volume via a bladder scan.
Catheter insertion
- Perform hand hygiene immediately before and after catheter-related activities.
- Ensure proper training of personnel charged with inserting urinary catheters.
- Insert catheters using aseptic technique and sterile equipment.
- Secure catheters after insertion to prevent movement and urethral traction.
Catheter maintenance
- Maintain a closed drainage system.
- Keep the catheter and collecting tube free from kinking.
- Keep the collecting bag below the bladder.
- Do not rest the bag on the floor.
- Do not change the catheter or collection bag routinely.
- Do not irrigate the catheter unless an obstruction is anticipated.
Specimen collection
- After disinfecting the port, aspirate the urine from the needleless sampling port with a sterile syringe.
Source: Gould et al 2010
Nephrostomy tubes
Inserted into the renal pelvis under sterile condition, a nephrostomy tube helps to relieve obstruction, treat hydronephrosis, and create an alternative route for urine excretion. Normal drainage is similar to voided urine. Along with catheter malfunction, infection is among the most common complications of nephrostomy tubes.
Although asymptomatic bacteriuria is common, suspect infection in the presence of purulent and malodorous discharge, flank or back pain, leukocytosis, and fever. Nephrostomy tube infections are polymicrobial, with Pseudomonas, Enterococcus, and E. coli among the most common pathogens.
To collect a urine specimen, place a sterile specimen cup at the tip of the nephrostomy tube and allow urine to flow by gravity. Use your hospital’s protocol for dressing changes, application of topical antibiotics around the insertion site, routine emptying, and infection workup.
Suprapubic catheters
A provider may order a suprapubic catheterization (placement of a drainage tube directly into the urinary bladder, just above the pubic symphysis) in the event of urinary retention that precludes urethral catheterization (such as in severe benign prostatic hyperplasia), morbid obesity, urethral strictures, bladder neck contracture, and genital malignancy. For long-term use, these catheters can improve patient comfort, decrease bacteriuria, and reduce the need for re-catheterization.
The incidence of CAUTI is similar in patients with urethral or suprapubic catheters. A study by Gibson and colleagues reported that although nursing home residents with a suprapubic catheter are more likely to be colonized with a multidrug resistant organism, they have fewer CAUTIs, hospitalizations, and need for antibiotic use.
The CAUTI bundle should be applied in the care of patients with suprapubic catheters. Maintain a free-flowing, sterile closed drainage, perform infection surveillance, and monitor the insertion site for leakage.
Treatment
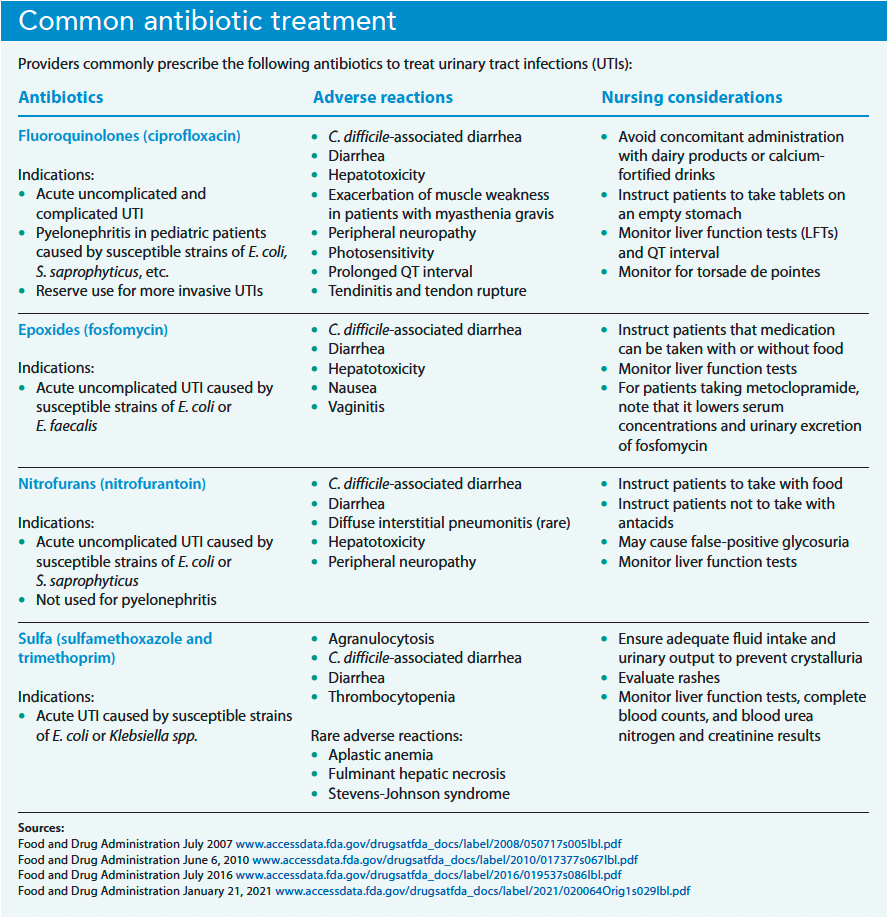
UTI is one of the most common reasons for antibiotic use. Consequently, uropathogenic antibiotic resistance has become an ongoing global issue. According to Gould and colleagues, an estimated one-quarter of E. coli and one-third of P. aeruginosa isolates from CAUTI cases were found to be fluoroquinolone-resistant. Grigoryan and colleagues note that immediate antibiotic therapy rather than delayed treatment has improved outcomes. Nurses should participate in individualized assessment of risk factors for antibiotic resistance and the patient’s response to treatment. (See Common antibiotic treatment).
The absence of clinical symptoms of UTI and the presence of bacteria in the urine (with or without pyuria) is called asymptomatic bacteriuria (ASB)—not a UTI. ASB doesn’t warrant antibiotic treatment.
Nursing implications
Initial and ongoing care of UTI, particularly among vulnerable older adults, requires high-quality nursing care. Typically, UTI symptoms improve within 2 to 3 days of starting antibiotics. Urine cultures must be collected before the first dose of antibiotics. During patient education, emphasize the importance of completing the full antibiotic course.
Nurses also should have an active role in interprofessional antibiotic stewardship. Advocate for prompt removal of catheters when they’re no longer clinically appropriate.
For patients with bowel and urinary incontinence, clean the patient promptly (wiping from front to back). If not contraindicated, encourage the patient to increase fluid intake. In addition, teach patients about proper hand hygiene and remind them not to manipulate the catheter.
For patients at risk for catheter self-extraction, the entire team should review the indication for continued catheterization, verify proper catheter placement, secure the catheter to the thigh, and assign a sitter to the patient. In some cases, applying a mitten to the patient’s hand can help prevent self-extraction.
For symptomatic relief of dysuria and urgency, the provider may prescribe phenazopyridine, a urinary antispasmodic. Explain to the patient that the medication causes red-orange urine discoloration that might stain fabric; it also can discolor or stain contact lenses.
To rule out antibiotic resistance, alert the provider to any UTI symptoms that don’t improve within the expected timeframe. Nurse managers should track and audit IUCs using established protocols.
Ms. Logan’s urinalysis shows leukocyte esterase, pyuria, nitrites, and large amounts of red blood cells. Pending culture and sensitivity results, the provider orders empiric treatment with sulfamethoxazole and trimethoprim. The plan of care includes monitoring for delirium, hydration, completion of antibiotics, and prevention of cascade iatrogenesis.
Significant contribution
UTI remains an epidemiologically significant infection across all healthcare settings, especially related to growing concerns about antibiotic resistance. The Centers for Medicare & Medicaid Services doesn’t reimburse costs associated with healthcare-associated CAUTI, so prevention has financial implications. Nurses contribute significantly to the evidence-based care of patients with UTI and in prevention efforts.
*Name is fictitious.
Fidelindo Lim is a clinical associate professor at New York University Rory Meyers College of Nursing in New York City.
American Nurse Journal. 2023; 18(12). Doi: 10.51256/ANJ122306
References
Bono MJ, Leslie SW, Reygaert WC. Urinary tract infection. StatPearls 2022. ncbi.nlm.nih.gov/books/NBK470195
Centers for Disease Control and Prevention. Catheter-associated urinary tract Infections (CAUTI). cdc.gov/hai/ca_uti/uti.html
Centers for Disease Control and Prevention. The NHSN standardized infection ratio (SIR). April 2022. cdc.gov/nhsn/pdfs/ps-analysis-resources/nhsn-sir-guide.pdf
Chu CM, Lowder JL. Diagnosis and treatment of urinary tract infections across age groups. Am J Obstet Gynecol. 2018;219(1):40-51. doi:10.1016/j.ajog.2017.12.231
Corder CJ, LaGrange CA. Suprapubic bladder catheterization. StatPearls. November 7, 2022. ncbi.nlm.nih.gov/books/NBK482179
Davies PE, Daley MJ, Hecht J, et al. Effectiveness of a bundled approach to reduce urinary catheters and infection rates in trauma patients. Am J Infect Control. 2018;46(7):758-63. doi:10.1016/j.ajic.2017.11.032
Eckburg PB, Muir L, Critchley IA, et al. Oral tebipenem pivoxil hydrobromide in complicated urinary tract infection. N Engl J Med. 2022;386(14):1327-38. https://doi.org/10.1056/NEJMoa2105462
El Haddad H, Viola G, Jiang Y, Raad I, Rolston KV, Szvalb A. Percutaneous nephrostomy tube-related infections. Open Forum Infect Dis. 2017;4(suppl 1):S349. doi:10.1093/ofid/ofx163.840
Gibson KE, Neill S, Tuma E, Meddings J, Mody L. Indwelling urethral versus suprapubic catheters in nursing home residents: Determining the safest option for long-term use. J Hosp Infect. 2019;102(2):219-25. doi:10.1016/j.jhin.2018.07.027
Gould CV, Umscheid CA, Agarwal RK, Kuntz G, Pegues DA; Healthcare Infection Control Practices Advisory Committee. Guideline for prevention of catheter-associated urinary tract infections 2009. Infect Control Hosp Epidemiol. 2010;31(4):319-26. doi:10.1086/651091
Grigoryan L, Trautner BW, Gupta K. Diagnosis and management of urinary tract infections in the outpatient setting: A review. JAMA. 2014;312(16):1677-84. doi:10.1001/jama.2014.12842
Johnson JR, Russo TA. Acute pyelonephritis in adults [published correction appears in N Engl J Med. 2018 Mar 15;378(11):1069]. N Engl J Med. 2018;378(1):48-59. doi:10.1056/nejmcp1702758
Letica-Kriegel AS, Salmasian H, Vawdrey DK, et al. Identifying the risk factors for catheter-associated urinary tract infections: A large cross-sectional study of six hospitals. BMJ Open. 2019;9(2):e022137. doi:10.1136/bmjopen-2018-022137
Medina M, Castillo-Pino E. An introduction to the epidemiology and burden of urinary tract infections. Ther Adv Urol. 2019;11:1756287219832172. doi:10.1177/1756287219832172
Mitchell BG, Gardner A, Stone PW, Hall L, Pogorzelska-Maziarz M. Hospital staffing and health care-associated infections: A systematic review of the literature. Jt Comm J Qual Patient Saf. 2018;44(10):613-22. doi:10.1016/j.jcjq.2018.02.002
National Healthcare Safety Network. Urinary tract infection (catheter-associated urinary tract infection [CAUTI] and non-catheter-associated urinary tract infection [UTI]) events. January 2023. cdc.gov/nhsn/pdfs/pscmanual/7psccauticurrent.pdf
Peng D, Li X, Liu P, et al. Epidemiology of pathogens and antimicrobial resistance of catheter-associated urinary tract infections in intensive care units: A systematic review and meta-analysis. Am J Infect Control. 2018;46(12):e81-90. doi:10.1016/j.ajic.2018.07.012
Petty LA, Vaughn VM, Flanders SA, et al. Risk factors and outcomes associated with treatment of asymptomatic bacteriuria in hospitalized patients. JAMA Intern Med. 2019;179(11):1519-27. doi:10.1001/jamainternmed.2019.2871
Serlin DC, Heidelbaugh JJ, Stoffel JT. Urinary retention in adults: Evaluation and initial management. Am Fam Physician. 2018;98(8):496-503.
Weiner-Lastinger LM, Pattabiraman V, Konnor RY, et al. The impact of coronavirus disease 2019 (COVID-19) on healthcare-associated infections in 2020: A summary of data reported to the National Healthcare Safety Network. Infect Control Hosp Epidemiol. 2022;43(1):12-25. doi:10.1017/ice.2021.362
Yoo MJ, Bridwell RE, Inman BL, Henderson JD, Long B. Approach to nephrostomy tubes in the emergency department. Am J Emerg Med. 2021;50:592-6. doi:10.1016/j.ajem.2021.09.034
Key words: urinary tract infection, UTI, catheter-associated urinary tract infection, CAUTI, nephrostomy tube, suprapubic catheter

















2 Comments. Leave new
Very good continue
Very informative