
What nurses need to know about social determinants of health and sleep.
Takeaways:
- Sleep is a necessary and complex physiological function.
- Social determinants of health can impact one’s ability to achieve appropriate quality and quantity of sleep.
- Inadequate sleep may contribute to developing or worsening of comorbid chronic conditions such as diabetes, cognitive deficits, and long-term neurodegeneration.
- Including sleep inquiry, evaluation, and treatment of sleep disorders in routine healthcare may have a positive and long-lasting effect on patients. Such inquiry can begin with the nursing assessment.
We all yearn to rest our weary minds from the day’s barrage of news, work, family, and social chaos. We want to sleep peacefully while our brain and body prepare for the next day. For some of us, restful slumber is a reality. We tuck ourselves in and say good night, a peaceful interlude. For millions of others, especially now, the reality is far from that.
The switch to working in the home or chaotic shifts for essential workers, children learning at home, and the danger of a pandemic have affected our ability to get the rest we need. Sleep becomes elusive when the environment is unsafe, economic instability persists, and illness strikes. Poor sleep contributes to mood changes, cognitive impairment, and disease risk. The complex interactions between our social environment, sleep, health, and well-being are significant but frequently are overlooked by healthcare providers.
In 1977, Engel challenged healthcare providers to incorporate more than just medical treatment in patient care. He proposed a bio-psycho-social model that includes behavioral health, environmental factors, and economic well-being in addition to traditional medical care. Since then, evidence has shown the efficacy of his approach, but the model hasn’t been widely implemented. Healthy People 2020 and Healthy People 2030 revived this approach with their Social Determinants of Health (SDoH) program. The five key determinants are: economic stability, education access and quality, social and community context, healthcare access and quality, and neighborhood and built environment.
Most healthcare providers know the importance of sleep because of their own experience with sleep deprivation, but they forget to include it in their health assessments. In addition, SDoH frequently aren’t addressed in clinical encounters, and many nurses are unaware of the inter-related and bi-directional aspects of SDoH and sleep. This article addresses four key questions: Does an adequate amount of sleep contribute to overall health? How do social determinants influence sleep? How can we recognize sleep disorders that are influenced by SDoH? What should we do about it?
Does an adequate amount of sleep contribute to overall health?
Many of us take good sleep for granted, only realizing it benefits when we don’t get enough. Inadequate sleep can impair our immune system, increase our risk for cardiovascular and endocrine disorders, and contribute to obesity.
Relationships have been found between sleep and health. In 2012, for example, the glymphatic pathway was discovered. This pathway provides a mechanism to clear the central nervous system of interstitial waste products that build up during the day and works primarily while we’re sleeping. Recent studies by Nedergaard and Nauen and Troncoso suggest a link between inadequate sleep and neurodegenerative disorders associated with the glymphatic pathway. Continuing research in this area may provide prevention and treatment targets.
The National Sleep Foundation recommends adequate sleep durations based on age (See Age and sleep.)
Age and sleep
The National Sleep Foundation recommends sleep durations based on age groups.
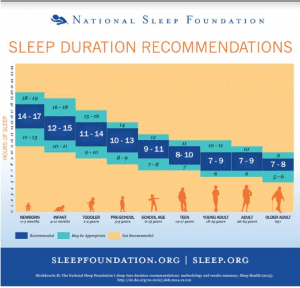
This copyrighted image is used with permission from the National Sleep Foundation.
However, according to the Centers for Disease Control and Prevention, approximately 35% of the U.S. adult population don’t achieve the recommended hours of sleep per night, with higher percentages for Blacks (45%) and Pacific Islanders (46%). Too much sleep also has been associated with cardiovascular issues, metabolic instability, and all-cause mortality. This is referred to as the U-shaped curve of sleep—too little (<6 hours) or too much (>9 hours) per sleep period has a negative impact on health.
The link between sleep–wake and circadian rhythms is well-known. When circadian rhythms are disrupted by shift work or irregular schedules, sleep is affected negatively and the restorative nature of sleep can’t be achieved. In addition to physical issues, inadequate sleep also can lead to emotional instability, impaired decision-making, and lack of moral judgment.
How do social determinants influence sleep?
According to Healthy People 2030, “Social determinants of health are conditions in the environments in which people are born, live, learn, work, play, worship, and age that affect a wide range of health, functioning, and quality-of-life outcomes and risks.” (See Daily life and health.)
Daily life and health
Many aspects of our daily lives directly impact our health.
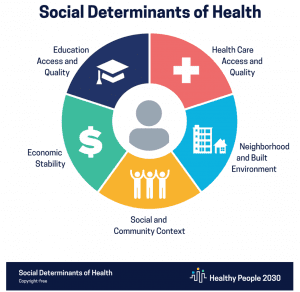
Environments that may contribute to health disparity include inadequate access to healthcare; communities without parks, sidewalks, and appropriate lighting; limited transportation; exposure to crime; language barriers; and low health literacy.
Chronic conditions, such as cardiovascular disease, diabetes, and obesity, also have been found to be higher in areas of lower socioeconomic status and areas of health disparity, with people of color and poorer individuals having worse health outcomes. Research by Ji and colleagues and a Canadian study by Singh and colleagues also found that these factors are associated with reduced sleep quantity and quality.
SDoH are not an all-or-none proposition. According to Hale and Hale, autonomy can be affected by social conditions that are out of a person’s control. For example, a person may have lost their job and still live in a relatively stable environment. For millions of people, their day-to-day lives are at odds with restorative sleep.
Sleep disorders and chronic conditions
Common sleep disorders, such as insomnia, and sleep-related disorders, such as obstructive sleep apnea (OSA), influence sleep quality and quantity. The burden of chronic conditions (obtaining prescriptions, healthcare access, and cost) may cause additional anxiety and worry. Patients diagnosed with OSA, for example, may face social and economic challenges when trying to obtain and maintain treatment, including continuous positive airway pressure devices or oral appliances.
As many as six out of ten adults have more than one chronic condition, which may increase the mental and economic burden of care. Many chronic conditions (including congestive heart failure, diabetes, and arthritis) have underlying issues, such as pain and depression, that also may negatively impact sleep.
How can we recognize sleep disorders that are influenced by SDoH?
Tools are available to assess patients for sleep disorders. One of the easiest techniques is to ask open-ended questions, such as “How is your sleep?” or “Do you snore?” If possible, asking a patient to keep a sleep log for 2 weeks before a clinic visit can provide data about the amount of sleep, time to fall asleep, and regularity of sleep pattern, which may be useful in patients with a primary complaint of insomnia. These data can contribute to the nurse’s knowledge about sleep onset problems, awakenings during the night, and early morning awakening. It also provides a baseline for evaluating treatment.
A commonly used tool to assess daytime sleepiness is the Epworth Sleepiness Scale (ESS), which consists of eight questions related to specific activities (for example, falling asleep in a car). Each question is scored on a scale of likelihood of falling asleep from zero to three. Total scale scores above the normal range (10 or higher with a range of 0–24) indicate excessive sleepiness and should be followed up with additional questions. Excessive sleepiness may be attributed to OSA, restless legs syndrome, or other disorders such as narcolepsy.
Nurses can use targeted questionnaires to assess for OSA risk factors. One such tool is the STOP-Bang questionnaire: Snoring, Tired, Observed stopping breathing/choking or gasping, and high blood Pressure; BMI, Age, Neck size and Gender.
Sleep and health disparities should be assessed in patients of all ages. Children living in at-risk neighborhoods and attending unsafe schools are at high risk to report a reduction in adequate sleep. Nurses who work with the pediatric population should be attuned to sleep disparities among children residing in lower socioeconomic neighborhoods. Data demonstrate that the ability to sleep well has a significant and potentially long-term impact on children. Health issues include obesity and type 2 diabetes. One of the most-used and simply administered questionnaires for children is BEARS. (See BEARS sleep screening tool.)
BEARS sleep screening tool
The questions asked in BEARS help pinpoint sleep issues that may contribute to behavior, growth, and academic problems in children. Although BEARS wasn’t developed for this purpose, it may offer some insight into a child’s living circumstances, sleeping conditions, and neighborhood environment. (For example, a parent might respond, “My child/I have difficulty falling asleep because we feel we’re at risk in our neighborhood, or we all sleep in one room,” which may signal that they’re experiencing social determinants of health issues in the home).
Bedtime problems (won’t stay in the bed, inability to fall asleep, strange feelings in the legs (restless legs syndrome)
Sample question: Does my child have trouble going to bed or trouble falling asleep?
Excessive daytime sleepiness (falling asleep when you don’t want to do, inability to concentrate)
Sample question: Is my child difficult to awaken in the morning?
Awakenings during the night (up to go to the bathroom/bed wetting, choking sensation, wake up cannot go back to sleep)
Sample question: Does my child awaken during the night and have trouble going back to sleep?
Regularity and duration of sleep (bedtime and wake-up time consistent, impacts to routine (2 jobs, shift work)
Sample question: What time does my child go to bed and get up on weekdays?
Snoring (indicator of upper airway restriction, strong indicator for OSA)
Sample question: Does my child stop breathing, gasp, or choke during sleep?
Source: Owens JA, Dalzell V, 2005.
What should we do about it?
Many beliefs and attitudes about sleep may be culturally intertwined. For instance, co-sleeping with infants is acceptable in many cultures; however, in several countries (including the United States and Australia) it’s discouraged and replaced with a crib next to the parental bed. In addition, some people may lack education about sleep and associated disorders. Providing information about the importance of adequate sleep, sleep hygiene, and sleep disorders is a good starting place for discussions with patients.
Nurses and other healthcare providers should recognize the interrelation of sleep, health, and social determinants. Identifying and addressing sleep complaints may improve overall health, response to illness, and mood. Simple suggestions to improve sleep health include maintaining sleep routines (for example, getting up the same time each day); limiting exposure to secondhand smoke; reducing TV, computer, and smartphone time; and decreasing caffeine intake. (See Healthcare workers and sleep.)
Healthcare workers and sleep
Many healthcare workers are so focused on caring for others that they ignore their own health issues. Consider taking these steps to improve your sleep.
- Keep a sleep log to evaluate your sleep quality and quantity.
- If you’re not getting the recommended amount of sleep, consider prioritizing sleep over other activities.
- If you work a regular schedule, try to maintain a regular sleep schedule as well.
- If you work night shift, small changes to the environment (such as blackout curtains or avoiding caffeine after noon) can help improve sleep and limit associated health consequences.
- You can access additional sleep tips for healthcare providers at
aasm.org/wp-content/uploads/2021/05/Prioritizing-Sleep-and-Managing-Fatigue.pdf
Identifying a potential sleep-related disorder such as OSA and, as appropriate, recommending referrals to sleep specialists may result in diagnosis and follow-up treatment. Unfortunately, many areas of high social disparity may lack sleep specialists. Coordinating services with other community resources may provide additional support. Changing some aspects of SDoH (moving out of a risky neighborhood) may not be possible, but recognizing the importance of sleep and implementing healthy sleep habits can have positive health and quality of life outcomes.
Always ask
Both health and healthy sleep are affected by SDoH, and a complex interaction between good sleep and good health exists. Always asking about sleep during assessments and acting on the information may have far-reaching implications for patients’ overall health and well-being.
Robyn Woidtke is currently a consultant to the sleep and medical device industries. She’s located in Northern California. Richard Rosenberg is an instructor in the department of psychology at California State University in Long Beach.
References
Artiga S, Hinton E. Beyond health care: The role of social determinants in promoting health and health equity. Kaiser Family Foundation. May 10, 2018. kff.org/racial-equity-and-health-policy/issue-brief/beyond-health-care-the-role-of-social-determinants-in-promoting-health-and-health-equity
Centers for Disease Control and Prevention. About chronic diseases. cdc.gov/chronicdisease/about/index.htm. April 28, 2021.
Centers for Disease Control and Prevention. Data and statistics: short sleep during among US adults. May 2, 2017. cdc.gov/sleep/data_statistics.html
Engel GL. The need for a new medical model: A challenge for biomedicine. Science. 1977;196(4286):129-36. doi:10.1126/science.847460
Grandner MA. Sleep, health, and society. Sleep Med Clin. 2017;12(1):1-22. doi:10.1016/j.jsmc.2016.10.012
Hale L, Hale B. Treat the source not the symptoms: Why thinking about sleep informs the social determinants of health. Health Educ Res. 2010;25(3):395-400. doi:10.1093/her/cyq027
Hale L, Troxel W, Buysse DJ. Sleep health: An opportunity for public health to address health equity. Annu Rev Public Health. 2020;41(1):81-99. doi:10.1146/annurev-publhealth-040119-094412
Iliff JJ, Wang M, Liao Y, et al. A paravascular pathway facilitates CSF flow through the brain parenchyma and the clearance of interstitial solutes, including amyloid β. Sci Transl Med 2012;4(147). doi:10.1126/scitranslmed.3003748
Jeon M, Dimitriou D, Halstead EJ. A systematic review on cross-cultural comparative studies of sleep in young populations: The roles of cultural factors. Int J Environ Res Public Health. 2021;18(4):2005. doi:10.3390/ijerph18042005
Ji XW, Grandner M, Petrov M. The role of age, sex, race/ethnicity, education, and marital status in the relationship of chronic health conditions and habitual sleep duration. Sleep. 2018;41(suppl 1):A332. doi:10.1093/sleep/zsy061.893
Laposky AD, Cauter EV, Diez-Roux AV. Reducing health disparities: The role of sleep deficiency and sleep disorders. Sleep Med. 2016;18:3-6. doi:10.1016/j.sleep.2015.01.007
Nauen DW, Troncoso JC. Amyloid-beta is present in human lymph nodes and greatly enriched in those of the cervical region. Alzheimers Dement. 2021;1-6. doi:10.1002/alz.12385
Nedergaard M. Garbage truck of the brain. Science. 2013;340(6140):1529-30. doi:10.1126/science.1240514
Owens JA, Dalzell V. Use of the ‘BEARS’ sleep screening tool in a pediatric residents’ community clinic: A pilot study. Sleep Med. 2005;6(1):63-9.
Ruggiero AR, Peach HD, Gaultney JF. Association of sleep attitudes with sleep hygiene, duration, and quality: A survey exploration of the moderating effect of age, gender, race, and perceived socioeconomic status. Health Psychol Behav Med. 2019;7(1):19-44. doi:10.1080/21642850.2019.1567343
Singh M, Hall KA, Reynolds A, Palmer LJ, Mukherjee S. The Relationship of Sleep Duration with Ethnicity and Chronic Disease in a Canadian General Population Cohort. Nat Sci Sleep. 2020;12:239-51. doi:10.2147/NSS.S226834
Thornton M, Persaud S. Preparing today’s nurses: Social determinants of health and nursing education OJIN: Online J Issues Nurs. 2018;23(3). doi:10.3912/OJIN.Vol23No03Man05 ojin.nursingworld.org/MainMenuCategories/ANAMarketplace/ANAPeriodicals/OJIN/TableofContents/Vol-23-2018/No3-Sept-2018/Social-Determinants-of-Health-Nursing-Education.html
Wickwire EM, Jobe SL, Oldstone LM, Scharf SM, Johnson AM, Albrecht JS. Lower socioeconomic status and co-morbid conditions are associated with reduced continuous positive airway pressure adherence among older adult Medicare beneficiaries with obstructive sleep apnea. Sleep. 2020;43(12):Zsaa122. doi:10.1093/sleep/zsaa122
Ye L, Smith A. Developing and testing a sleep education program for college nursing students. J Nurs Educ. 2015;54(9):532-5. doi:10.3928/01484834-20150814-09

















