Dedicated safe patient handling and mobility coordinators
- Dedicated safe patient handling and mobility (SPHM) coordinators play a crucial role in successful SPHM programs.
- Despite the evidence, many organizations struggle with implementing and sustaining the practice change necessary to maintain SPHM programs.
- Learning how to develop and present a business case to support the SPHM program and coordinator role can aid organizational buy-in.
Healthcare organizations that have implemented effective safe patient handling and mobility (SPHM) programs report a reduction in healthcare worker injury rates related to manual patient handling. In addition, organizations with early mobility programs report a decrease in harm associated with immobility (including hospital-acquired pressure injuries [HAPI] and delirium) and improved financial stewardship through decreased lengths of stay (LOS) and episode-of-care costs. Correlated data remain limited, but mobilization also is noted as an intervention for nonventilator hospital-acquired pneumonia (NV-HAP).
Despite the evidence for SPHM programs, organizations struggle with implementing and sustaining the practice change necessary to maintain them. The SPHM coordinator role serves as a crucial element for success.
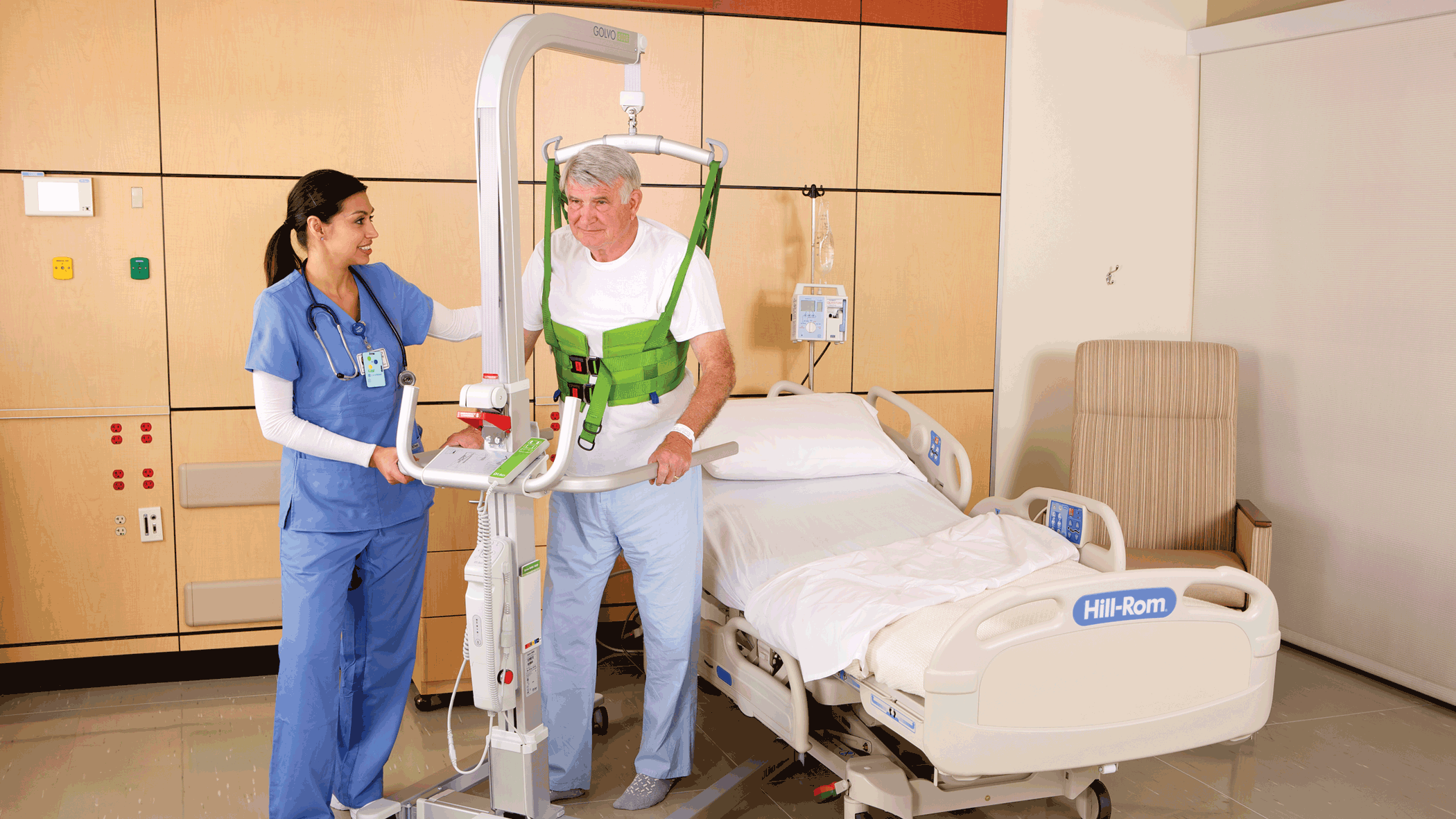
Ceiling lifts and safe patient handling and mobility programs
A lack of information in the literature regarding the SPHM coordinator role prompted us to conduct two separate but similar surveys in 2020 and 2022 to better understand the role. As certified SPHM professionals with extensive collective experience coordinating and supporting healthcare organization SPHM programs, we’ve witnessed how SPHM coordinators support program sustainment and enable positive program and early mobility outcomes. (See SPHM role.)
SPHM role
Typically, safe patient handling and mobility (SPHM) coordinators have responsibility for SPHM program oversight, including equipment justification, education and training, policy development, and metrics. Success requires that the role include interdisciplinary coordination and partnership with healthcare initiatives, including patient safety, quality, rehabilitation, occupational health, nursing leadership, biomedical engineering, and environmental services. The coordinator acts as an advocate, expert, and liaison for organizational safe mobility practices.
With increased oversight, the SPHM coordinator can effectively implement evidence-based models, such as the American Nurses Association SPHM Interprofessional National Standards. These standards allow for timely guidance and interventions for challenging patient handling situations, prompt identification and removal of barriers related to internal processes, and encourage focus on program improvement. Using their expertise to drive root cause analyses and mitigation strategies, coordinators lead investigations and interventions in response to safety events.
The coordinator acts as a liaison with hospital leadership regarding all aspects of the SPHM program. They also answer questions about program return on investment, including employee safety and positive impacts on employee injury claims/workers’ compensation costs, patient safety, costs related to injury claims, reimbursement, and operational efficiency.
The surveys
Two of our authors, Jaworski and Kielich, conducted the surveys. For the 2020 survey, they used SurveyMonkey to collect information from healthcare organizations about the SPHM coordinator role using 10 main questions. They disseminated the survey to an Association of Safe Patient Handling Professionals (ASPHP) listserv group and SPHM coordinators known to them and via social media platforms. Ultimately, 66 people responded. At the ASPHP National SPHM Education Event in March 2021, Jaworski and Kielich presented a poster titled “SPHM…Who Handles the Handling,” which summarized the 2020 results.
In 2022, based on feedback from the first survey, Jaworski and Kielich conducted a follow-up survey with 16 main questions using Microsoft Forms survey. They used the same distribution methods; 80 people responded. Jaworski and Kielich presented the 2020 and 2022 results at the ASPHP National SPHM Education Event in March 2023. (See the questions at myamericannurse.com/?p=417892.)
Survey questions focused on five topics: amount of time dedicated to the SPHM program; length of time the role has existed in the organization; role responsibilities, disciplines, and length of time in the coordinator position; reporting structure; and metrics (tracking program effectiveness). In addition, the 2020 survey asked about SPHM certification. The 2022 survey included questions regarding status of the SPHM coordinator position during and after COVID, size of the facility, SPHM oversight for multiple sites, and use of the American Nurses Association SPHM standards.
Respondent organization sizes ranged from 50 to more than 600 beds. Some respondents worked in critical access hospitals or ambulatory settings; 17 managed multiple sites or had a system role.
Survey questions
In a 2020 survey, we asked safe patient handling and mobility (SPHM) coordinators to answer the following 10 questions.
- Where do you report within your organization?
- Where do you feel you should be reporting?
- What percentage of your time is dedicated to SPHM?
- Do you feel the allotted time is sufficient to complete your SPHM responsibilities?
- What (if any) other responsibilities do you have outside your SPHM role at your organization?
- Which of the following metrics do you measure as part of your SPHM program?
- Patient handling injuries
- Workers’ compensation claims/costs
- Pressure injuries
- Patient falls
- Length of stay
- Number of mobility events each day
- Nonventilator pneumonia
- Deep vein thrombosis
- Which of these metrics have improved with your SPHM program?
- Are you and your SPHM program performance measured using the above metrics?
- Other comments
- Please answer the following questions as it applies to you and your role.
- I am certified through the Certified Safe Patient Handling Professionals.
- Length of time in the role (ranges given to select)
- I feel this role is secure in my organization.
In 2022, after the COVID-19 pandemic, we asked the following 16 questions:
- During the COVID-19 pandemic were you redeployed from your SPHM role?
- If yes, were you reinstated?
- What size is your facility?
- If you oversee multiple sites, are there local or regional coordinators for the site(s)?
- Which of the below metrics does your SPHM program measure?
- Patient handling injuries
- Workers compensation claims/costs
- Hospital-acquired pressure injuries
- Patient falls
- Length of stay
- Number of mobility events each day
- Compliance with a mobility assessment
- Discharge destination
- In which of these metrics have you seen an improvement?
- Do you provide SPHM coordination 100% of the time?
- If 100% of your time is dedicated to SPHM coordination, how long has your facility maintained this role?
- As a 100% dedicated SPHM coordinator, what is your report structure?
- If 100% of your time is not dedicated to SPHM coordination, what percentage of your FTE is dedicated to SPHM coordination? (ranges given)
- If <100% of your time is dedicated to SPHM coordination, how long has your facility maintained this role?
- As a <100% dedicated SPHM coordinator, what is your report structure?
- If 100% of your time is not dedicated to SPHM coordination, who has oversight for the program?
- Nursing
- Rehab/therapy
- Patient safety (risk management/quality)
- Caregiver safety (occupational health)
- Ergonomics
- What is your discipline?
- Nursing
- Occupational therapy
- Physical therapy
- Ergonomics
- Caregiver safety
- Patient safety
- Do you currently follow the American Nurses Association SPHM Interprofessional Standards?
- Additional comments
The results
The surveys offered insight into the responsibilities of the SPHM role as it’s deployed in various organizations. (See Survey results)
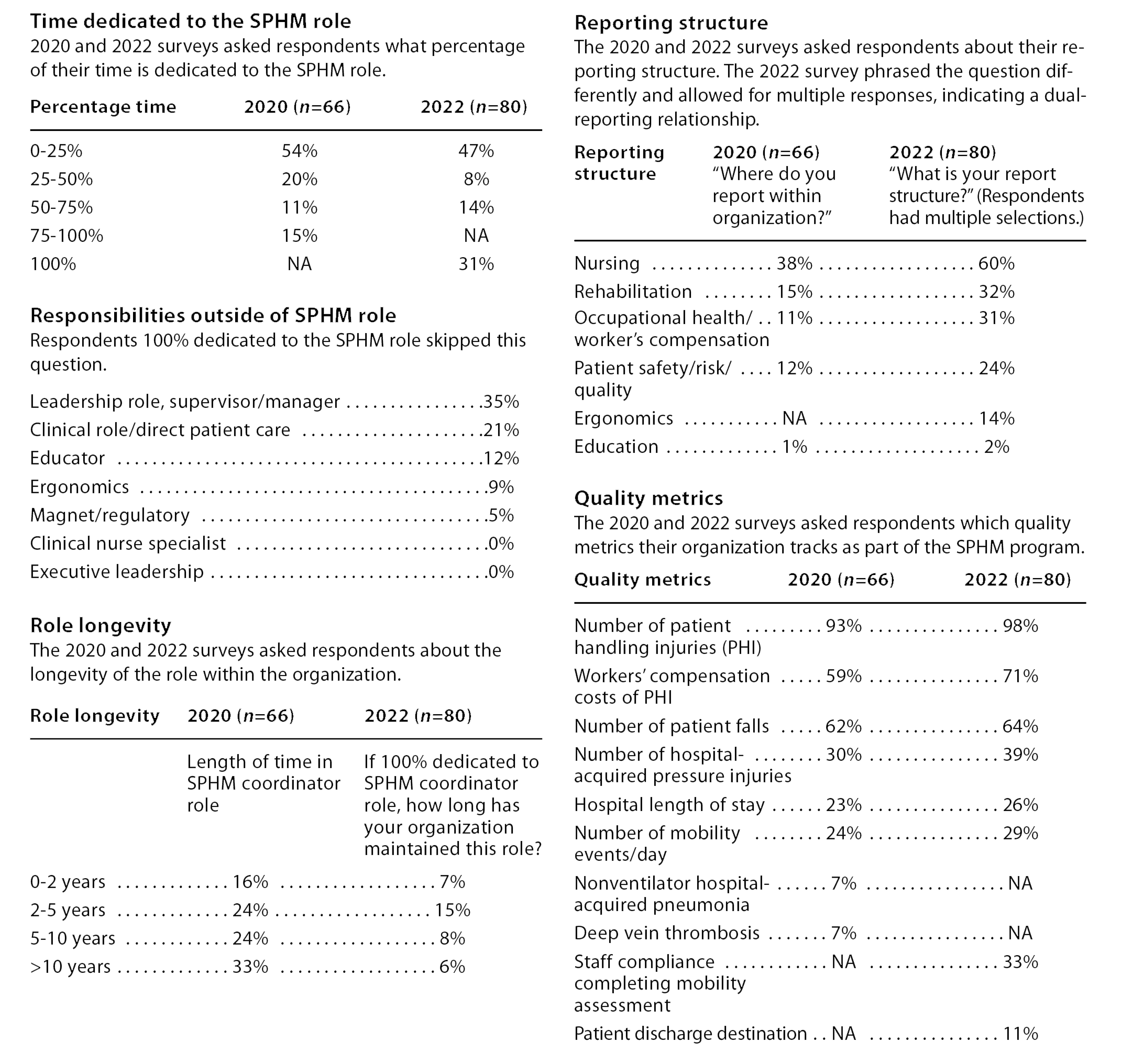
Survey Results
The 2020 and 2022 surveys of safe patient handling and mobility (SPHM) coordinators included questions about the following topics: amount of time dedicated to the role; responsibilities outside of the SPHM role; role longevity (if 100% of respondent time is dedicated to the role, how long that has been the case); reporting structure; and studied metrics
Dedicated time
In the 2020 survey, 15% of respondents reported that they spend 100% of their full-time job as an SPHM coordinator. In 2022, that number increased to 31%. This rise may result from organizations recognizing the importance of the role. We found this increase promising because we believe that having a dedicated full-time SPHM coordinator plays a crucial role in program sustainability and success.
For those whose position wasn’t 100% dedicated to the coordinator role, the 2020 survey asked respondents to list their other responsibilities. Answers included educator, ergonomics, and executive leadership. We question whether anything less than 100% dedicated time indicated that the respondent functioned more as a SPHM point-person rather than a coordinator.
Length of time
The surveys asked similar, though not identical, questions regarding the length of time the SPHM coordinator role has existed in the respondents’ organizations. In 2020, the survey asked the respondents how long they’ve served in the coordinator role (33% had served for over 10 years). In 2022, the survey asked, if their organization has a 100% dedicated SPHM coordinator role, how long has it existed (15% said 2 to 5 years).
We believe that the appointment of a dedicated SPHM coordinator serves as a powerful optic that highlights an organization’s commitment to sustaining SPHM practices.
Disciplines and reporting structure
In 2022, most of the respondents reported their discipline as nursing (50%), with physical therapy (24%) and occupational therapy (15%) as the next highest groups.
Based on survey results, standardized reporting structures for SPHM coordinators don’t exist. The 2020 survey indicated that most SPHM coordinators report to nursing (38%), followed by rehabilitation (15%) and occupational/employee health (10%). In 2022, respondents could select more than one option; many listed more than one reporting relationship.
Due to the impact of SPHM practices on employee injuries, many organizations place their SPHM programs within the ergonomics, employee/occupational health, or workers’ compensation departments. However, we noted a shift in organizations placing SPHM programs within nursing or patient safety/quality departments focused on nursing-sensitive indicators such as mobilizing patients early, using SPHM equipment, and reducing falls.
Placement of SPHM coordinators within an organization impacts the ability to maintain momentum and creates a sense of urgency regarding SPHM practices and culture change. If positioned in a clinical hierarchy, the SPHM coordinator would have a seat at the table for decision-making regarding mobility, falls, LOS, equipment, and sling selection where safe mobility positively impacts patient initiatives. When placed in a nonclinical hierarchy, such as human resources or workers’ compensation departments, the SPHM coordinator’s involvement will include workers’ compensation data collection, incident reports, injury categories, and tracking costs related to patient handling injuries. Penalties and diminished reimbursements from the Centers for Medicare & Medicaid Services (CMS) affects hospital finances. Fiscal stewardship will be fully realized by the chief financial officer and the rest of the C-suite when savings associated with both employee and patient injury reduction are recognized.
Although healthcare organizations may differ with regard to SPHM program placement, the overarching goal remains the same: an identified person whose full-time job description entails overseeing the SPHM program and collaborating with departments that impact caregiver and patient care initiatives. If the coordinator doesn’t directly report to nursing, a strong link to nursing leadership and patient care should exist. Part of this practice change includes a nursing acknowledgement that mobility is a shared responsibility between therapy and nursing and must involve the consistent use of SPHM equipment to mobilize and transfer patients safely during the patient’s entire hospitalization. Comments from respondents echoed this sentiment; for example, one said, “SPHM programs need to have a strong nursing practice and leadership component.”
Do you want to hear more about this topic?
Watch the Who handles the handling? OnDemand Webinar!
Metrics
An important aspect of the SPHM coordinator role includes tracking program impact, which requires strong data management and analysis skills. Early studies noted the impact of SPHM technology in reducing healthcare worker injuries. Studies published in 2023 by Ryan, Boynton, and Gabele reaffirm that consistent use of SPHM technology reduces caregiver injuries and impacts patient outcomes.
In both surveys, respondents reported patient handling injuries, workers’ compensation claims, patient falls, and pressure injuries comprised the top four metrics collected from the respondents. Additional metrics reported in both surveys included LOS and the number of mobility events when a patient was moved outside of their bed or ambulated.
Tracking patient outcome shows promise. Consider the impact of mobilizing patients early and often using SPHM technology. Duke University Medical Center implemented an inpatient mobility care program to track patient mobility status based on Bedside Mobility Assessment Tool scores. The medical center aimed to increase the number of mobility events to prevent patient decline and improve discharge disposition. This focus led to significant financial benefits by decreasing LOS and avoiding costs for additional days of care. In 11 months, the organization saved $512,958.
A 2019 study by Jones and colleagues describes a nurse-led mobility initiative that resulted in a 40% increase in mobility events and a 14% decrease in inappropriate physical therapy orders. The researchers noted no significant change in falls or pressure injuries. They also found that sustainability depends on many factors, including maintaining support for a mobility coordinator.
The literature documents the impact of immobility on the body, including the loss of functional gait, strength, and balance. Mobility serves as a key component in hospital quality initiatives, including geriatric care models and LOS. A more recent approach to fall prevention focuses on safe mobility and keeping patients moving rather than staying in bed. (See Early mobility and SPHM practices.)
Early mobility and SPHM practices
In response to universal recognition of early mobility as vital to decreasing hospital-acquired complications and preventing deconditioning and strength loss, healthcare organizations are implementing early mobility programs.
Wald and colleagues, in an executive summary white paper for the American Geriatrics Society (AGS), recommend that the Centers for Medicare & Medicaid Services (CMS) develop a mobility quality measure to incentivize organizations to actively intervene to prevent mobility loss among hospitalized older adults. The AGS also recommends shifting the regulatory focus in acute care from fall prevention to safe mobility.
In 2023, CMS included a request for comment in the inpatient prospective payment system regarding the role of a mobility assessment in the certification process of a geriatric center of excellence. The federal regulatory level has begun recognizing the role of safe mobility and mobility assessment. In 2022, the United States Appropriations Bill included language to guide hospitals to incorporate mobility assessments.
What’s not universally recognized is the impact of SPHM technology on increasing patient mobility. This practice change is necessary to shift healthcare workers from manually moving patients to using technology—such as mechanical lifts (powered ceiling-mounted and floor-based mobile total lifts, powered sit-to-stands), non-powered stand aids, and air-assisted and friction-reducing devices—to accomplish care tasks more safely.
A 2020 study by Kayser and colleagues showed that limited mobility patients were 1.94 times more likely to be observed in a bedside chair when a lift is used. The focus of a dedicated SPHM coordinator can help ensure the removal of all barriers cited by healthcare workers and the implementation of solid processes that support staff.
Building the business case
With evidence emerging on the positive outcomes of SPHM programs, having a dedicated person oversee the program should reap benefits.
Some of the greatest challenges to building viable SPHM programs include failure to change practice or culture and an inability to build a sustainable program that frontline workers believe benefits themselves and their patients. Appointing a dedicated coordinator with appropriate credentials, experience, background, and administrative support, who has comprehensive oversight of the SPHM program, could help overcome these challenges. In 2019, the Federal Guidelines Institute published a revised white paper, “Patient Handling and Mobility Assessment (PHAMA),” which aims to ensure safe work environments by facilitating the incorporation of SPHM technology into healthcare facility design.
In addition to technology recommendations, PHAMA offers program strategy guidance. Appendix Q specifically references the coordinator role and its benefits to overall program implementation and sustainment. Without such a position, peer leaders in patient care areas face limitations and SPHM programs lose their impact. The paper also points out that larger organizations need at least one full-time coordinator.
The 2022 survey indicated that, even during the COVID-19 pandemic, organizations deemed the role important. Some respondents reported that they were reassigned during the pandemic but were reinstated to their coordinator position afterwards.
Justifying the SPHM coordinator role
Justifying and maintaining a qualified SPHM coordinator can prove challenging. When building a business case, according to La Duke, ask the following questions:
- What problem do you want to solve by spending this money (for example, standardize care, decrease staff injuries, improve patient safety and outcomes)?
- How much does this problem cost the organization (for example, cost of false-starts and failures to get staff buy-in; ongoing patient falls, HAPI’s, and NV-HAP; purchase of equipment that staff refuse to use; failure to provide adequate types and amounts of equipment)?
- How much will it cost to fix the problem (create and fund a full-time SPHM coordinator, complete a gap analysis, and purchase optimal amounts and types of SPHM equipment for each unit)?
- How long will it take before the hospital has saved money by addressing the problem equal to the cost of the problem (estimated return on investment date [ROI], tracking and reporting of financial savings)?
Dang and colleagues summarized current evidence of SPHM impact on healthcare worker and patient outcomes necessary to develop an ROI model in the ICU setting. ROI cases should recognize the impact SPHM programs have on avoiding complications associated with immobility, decreasing LOS, and enhancing patient initiatives (including HAPIs, delirium, falls, 30-day readmission, and hospital-acquired condition penalties). Similarly, value accrues as a result of consideration given to anticipated loss and costs if an SPHM coordinator position isn’t funded and a program fails to meet expectations and goals.
Boynton showed that, in a system of 24 hospitals, those without dedicated SPHM leads and adequate administrative and financial support continued to struggle and failed to meet goals. In contrast, hospitals with dedicated SPHM leads and optimal support reported good results and documented them in biannual dashboard reports.
National standards
The American Nurses Association SPHM standards have proven integral to enhancing the credibility of SPHM programs and encouraging organizations to develop them for both patient handling injury reduction and improved patient mobility to reduce harmful effects of immobility. The association’s SPHM standards encourage employers to establish a formal program to reduce the risk of injury to patients and healthcare workers while improving quality of care. The standards recommend an organizational committee approach to link department and SPHM goals and create a culture of safety.
The 2022 survey asked respondents if their facilities follow the American Nurses Association SPHM standards; 54 (68%) responded, “Yes”; 2 (3%) answered, “No”; and 24 (30%) stated that they were unaware of the standards.
The American Nurses Association, via a nurse staffing task force, continues to address staffing issues, which escalated during the pandemic. The task force recommends reformation of the work environment by prioritizing safety management systems. SPHM programming has a direct correlation with safe work environments by minimizing manual handling as the go-to and accepted method for moving and transferring patients.
No one discipline is immune from turnover. PHAMA recommends that, when making a business case for SPHM programs and obtaining funding for an SPHM coordinator, consider savings associated with improved patient health and quality of life as well as savings as a result of improved staff retention.
Coordinator job description
When considering creation of a new SPHM coordinator role, look at similar roles created to address patient populations and their needs, such as geriatric resource nurses or early recovery after surgery (ERAS) programs. As described by Watson in a 2018 article about nurse coordinators and ERAS, during implementation of a sustainable program, the nurse coordinator establishes evidence-based practice guidelines, shepherds appropriate committees, maintains practice and culture change momentum, creates evidence-based education plans and materials, and conducts data collection and reporting structures.
SPHM program implementation and sustainability require the same steps. Role qualifications include the ability to reach across the organization, solid project management skills, and high-level decision-making authority. When asked by Falco and colleagues what skills ensure successful management of SPHM programs, SPHM coordinators identified soft skills like communication and emotional intelligence as well as hard skills such as advanced clinical knowledge with equipment and the ability to analyze data. Due to frequent requests, the authors created a job description for the SPHM coordinator role. (See SPHM job description.)
SPHM coordinator job description
The summary below describes the job description we created for the safe patient handling and mobility coordinator role.
The full-time SPHM coordinator/manager
- Manages development, implementation, evaluation, education, continuous improvement, and on-going sustainability of the program
- Serves as an advocate and expert liaison for patient outcomes, caregiver safety, and safe mobility practices across the organization
Education and experience
- Bachelor’s degree, 2 to 5 years’ experience and licensure in healthcare-related field
- Direct patient care experience strongly recommended
- Formal project management education or experience
- Safe patient handling professional and/or ergonomics certification preferred
Required skills and abilities
- Experience using patient handling and mobility devices; critical/analytical thinking
- Strong computer and communication skills
- Data analysis with ability to identify trends and opportunities
- Ability to create a business case for SPHM expansion
Essential functions of the role include the following:
Program development and implementation
- Elicit interdisciplinary support to foster a just culture
- Create and enforce policies for mobility assessments and SPHM technology
- Create a sense of urgency regarding SPHM practices and culture change
- Review literature ensuring foundational evidence-based practice for the care pathway
- Maintain oversight focused on implementing evidence-based models such as the American Nurses Association SPHM Standards; include bedside champions and mobility assessment to build sustainment
- Provide oversight to drive maximum benefit from SPHM program
Program design
- Integrate and coordinate with falls, mobility, safety, quality, and workplace violence committees; contribute expertise to enhance patient outcome quality initiatives
Education, training, and clinical solutions
- Mentor interdisciplinary SPHM champions
- Develop SPHM education/training programs
- Evaluate need for retraining post-injury and address unit-specific gaps in practice
- Provide just-in-time interventions for challenging situations; prompt identification and removal of barriers related to processes such as sling par levels
Compliance and accountability
- Collaborate with clinical managers, risk management, caregiver safety leads, employee/occupational health, environmental and facility management, human resources
- Ensure organization complies with regulations/guidelines as required by state and federal laws
Metrics
- Collect data related to SPHM outcomes
- Create database for tracking data related to program
- Provide data reports to leadership
Operations
- Set facility SPHM specifications for construction; coordinate with design and construction teams to ensure adherence to specifications
- Work with capital equipment planners using Federal Guidelines Institute/Patient Mobility and Assessment guidelines
- Collaborate with supply chain for equipment purchasing and par levels
- Establish processes for sling use
- Coordinate with plant operations, biomedical department, and facilities to ensure ongoing device inspection, maintenance, and timely repair
Budget
- Establish criteria/budget process for purchase and replacement of SPHM equipment
- Collaborate with leadership to ensure financial support to meet evolving SPHM equipment needs
Significant impact
A dedicated coordinator responsible for SPHM practices can significantly impact nursing-sensitive indicators, address complications associated with immobility, improve patient outcomes, and trigger cost savings. These coordinators can help ensure a safe work environment with goals of decreasing risk, preventing patient handling injuries, and keeping experienced caregivers at the bedside. Success requires that this role include strong interdisciplinary coordination as well as partnership with other healthcare initiatives and departments.
The 2020 and 2022 survey results indicate that hospitals have implemented the SPHM coordinator role with promising results. Although a variety of disciplines may successfully fill this role, nursing leadership must remain engaged and accountable. We encourage further research on the impact of dedicated full-time SPHM coordinators on patient initiatives, improved patient outcomes, and a safer work environment, as well as research into links between SPHM practices and improved mobility practices.
Renée Kielich is a clinical consultant specializing in safe mobility programming. Tricia Jaworski is safe patient handling and mobility program manager at Advocate Health. Teresa Boynton is a clinical consultant specializing in safe mobility programming. Nicole Hopewell is a clinical consultant specializing in safe mobility programming.
American Nurse Journal. 2025; 20(6). Doi: 10.51256/ANJ062554
References
Boynton T. Coding and applying injury claims data to implement and sustain effective safe patient handling and mobility solutions. Int J Ind Ergon. 2023;93:103397. doi:10.1016/j.ergon.2022.103397
Dang T, Roberts D, Murray AK, Wiggermann N. A return-on-investment model using clinical and economic data related to safe patient handling and mobility programs in the ICU. Int J Ind Ergon. 2022;92:103372. doi:10.1016/j.ergon.2022.103372
Falco K, Monaghan HM. Soft skills: The foundation for effective SPHM program leadership: A national survey. Int J SPHM Falls Manage. 2018;8(2):76-90.
Gabele D, Mendez S, Giuliano KK. Early and progressive mobility in a community hospital. Nurs Manage. 2023;54(3):22-7. doi:10.1097/01.NUMA.0000919068.76409.b2
Jones RA, Merkle S, Ruvalcaba L, Ashton P, Bailey C, Lopez M. Nurse-led mobility program: Driving a culture of early mobilization in medical-surgical nursing. J Nurs Care Qual. 2020;35(1):20-6. doi:10.1097/ncq.0000000000000404
Kayser SA, Wiggermann N, Kumpar D. Factors associated with safe patient handling practice in acute care and its relationship with patient mobilization: A cross-sectional study. Int J Nurs Stud. 2020;104:103508. doi:10.1016/j.ijnurstu.2019.103508
La Duke P. Going for broke: Building a business case for safety. OHS Professional. March 2020:14-7. issuu.com/safetyinstitute/docs/ohspromarch2020final
Ryan D, Anderson C, Connolly AM, Veety L, Villavicencio T, Parks L. An evaluation on the effects of safe person handling program implementation at long term care facilities for persons with complex intellectual, developmental, and medical conditions. Am J Ind Med. 2023;66(4):320-32. doi:10.1002/ajim.23468
Wald HL, Ramaswamy R, Perskin MH, et al. The case for mobility assessment in hospitalized older adults: American Geriatrics Society White Paper Executive Summary. J Am Geriatr Soc. 2019;67(1):11-6. doi:10.1111/jgs.15595
Watson DJ. Nurse coordinators and ERAS programs. Nurs Manage. 2018;49(1):42-9. doi:10.1097/01.numa.0000527718.90264.89
Key words: patient mobility, safe patient handling, safe patient handling and mobility coordinators, patient safety, falls prevention


















