Your knowledge and quick action aid a positive outcome.
- With a mortality rate exceeding 50%, acute mesenteric ischemia requires prompt nursing identification and vascular intervention.
- Most patients experience acute onset of abdominal pain out of proportion to a physical examination, nausea, vomiting, and melena.
- Prompt surgical evaluation is necessary to identify, minimize, and prevent irreversible intestinal damage.
Wanda Star*, a 64-year-old woman with a history of hypertension, coronary artery disease (CAD), and hypercholesterolemia, arrives at the ED with shortness of breath and palpitations that have worsened over 3 months. A 12-lead ECG performed in the ED shows atrial fibrillation with rapid ventricular response. Ms. Star’s heart rate normalizes after a 5 mg I.V. diltiazem bolus and infusion. She’s admitted to the cardiac telemetry unit with diltiazem titration orders and initiation of apixaban 5 mg twice daily.
History and assessment
Although Ms. Star remains in atrial fibrillation, her vital signs are stable: temperature 98.4° F (36.9° C), HR 84 bpm, RR 20 breaths per minute, BP 138/84 mmHg, and O2 saturation 97% on 2L of O2 via nasal cannula. At the beginning of your shift, Ms. Star reports 5/10 diffuse abdominal pain and nausea. After you administer 4 mg of I.V. ondansetron and 2 mg of I.V. morphine sulfate as ordered, her symptoms improve somewhat.
During your 3 am assessment, Ms. Star is vomiting and reports 10/10 diffuse abdominal pain. She won’t let you assess her abdomen. You re-administer 2 mg of IV morphine sulfate without improvement. Her vital signs are temperature 101° F (38.3° C), HR 132 bpm, RR 28 breaths per minute, BP 94/42 mmHg, and O2 saturation 94% on 4L of O2 via nasal cannula.
Taking action
Recognizing Ms. Star’s declining condition, you activate the RRT and page the on-call hospitalist. The team places Ms. Star on a non-rebreather O2 mask at 15L per minute. The hospitalist is concerned about acute mesenteric arterial embolism and orders a STAT complete blood count, comprehensive metabolic panel, lactate, and tri-phasic CT angiogram of the abdomen and pelvis. The CT scan reveals an embolic occlusion of the superior mesenteric artery (SMA), which has resulted in acute mesenteric ischemia (AMI). In addition, Ms. Star’s lactic acid is elevated at 14.6 mg/dL. The hospitalist immediately consults general and vascular surgery.
Outcome
Ms. Star is taken to the hybrid endovascular OR for open embolectomy and mesenteric angiography. No transmural intestinal necrosis is identified. After surgery, she’s admitted to the ICU for serial abdominal examinations, fluid resuscitation to achieve euvolemia and adequate tissue perfusion, and I.V. heparin. To maintain mucosal integrity, the surgeon orders holding enteral nutrition until persistent AMI is ruled out. On postoperative Day 9, Ms. Star is discharged to rehab with prescriptions to continue diltiazem and apixaban.
Education and follow up
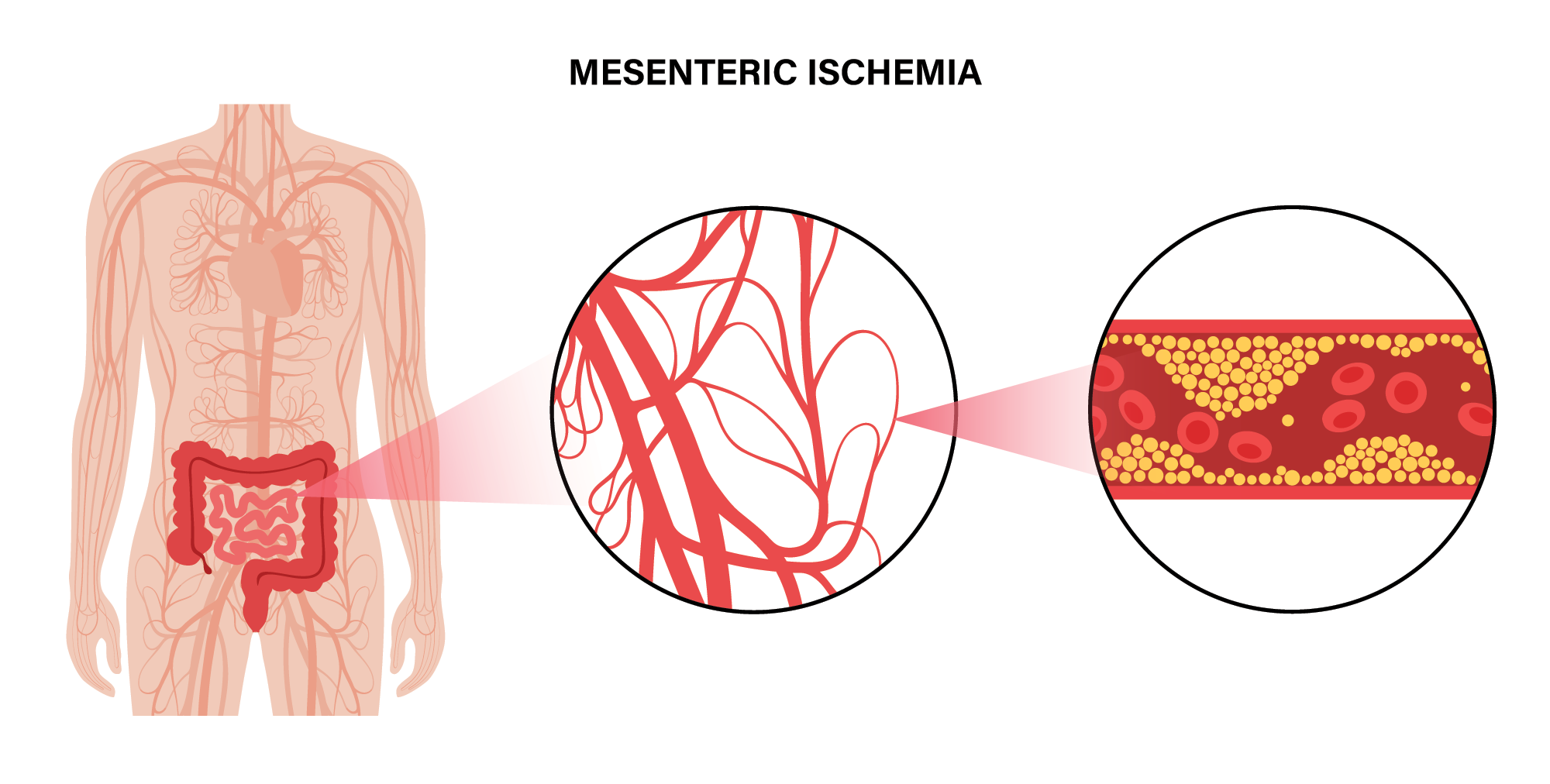
AMI occurs as a result of inadequate blood flow and O2 delivery caused by arterial embolism, arterial thrombosis, venous occlusion, or nonocclusive ischemia. Patients at the highest risk are older adults with dysrhythmias, prior myocardial infarction, and valvular disease. Without prompt revascularization, mortality exceeds 50%.
Most patients experience acute onset of abdominal pain out of proportion to a physical examination, nausea, vomiting, and melena. However, no specific laboratory studies indicate AMI. Initially, symptoms may be nonspecific, resulting in delayed diagnosis, so astute nursing assessments are critical. Prompt surgical evaluation identifies, minimizes, and prevents irreversible damage irreversible intestinal damage.
Ms. Star’s atrial fibrillation, CAD, and advanced age predisposed her to AMI due to SMA occlusion. Activation of the RRT facilitated a quick assessment and implementation of evidence-based treatment.
*Names are fictitious.
Aaron M. Sebach is dean of the College of Health Professions and Natural Sciences at Wilmington University in New Castle, Delaware, and hospital medicine nurse practitioner at TidalHealth Peninsula Regional in Salisbury, Maryland.
American Nurse Journal. 2023; 18(5). Doi: 10.51256/ANJ052356
References:
Kanasaki S, Furukawa A, Fumoto K, et al. Acute mesenteric ischemia: Multidetector CT findings and endovascular management. Radiographics. 2018;38(3):945-61. doi:10.1148/rg.2018170163
Reintam Blaser A, Acosta S, Arabi YM. A clinical approach to acute mesenteric ischemia. Curr Opin Crit Care. 2021;27(2):183-92. doi:10.1097/MCC.0000000000000802
Reintam Blaser A, Forbes A, Björk M. Acute mesenteric ischaemia. Cur Opin Crit Care. 2022;28(6):702-8. doi:10.1097/MCC.0000000000000972
Key words: acute Mesenteric ischemia, abdominal pain, arterial embolism


















