In June 2013, a mother and her 11-year-old son drove to the North Carolina mountains for an overnight stay and checked into a nice hotel with an indoor pool. Shortly after their arrival, she went to the bathroom to remove her contacts while her son used his iPad on the bed. In the bathroom, she was overcome with nausea, prompting her to lie down on the floor. The last thing she remembered was reaching for the door and calling for her son.
What she didn’t know was that their room was directly above the indoor swimming pool and pool heater. High levels of carbon monoxide (CO) had leaked from the pool heater and venting system directly into their room. Around noon the next day, hotel employees found the young boy dead and his mother unconscious in the bathroom.
CO exposure is the leading cause of poison-related deaths in the United States. More than 450 unintentional, non-fire-related CO deaths occur in the United States yearly, but the Centers for Disease Control and Prevention estimates an additional 20,000 annual exposures require emergency intervention. These figures probably underestimate the incidence of non-lethal acute exposures, because signs and symptoms of CO poisoning are vague and easily mistaken for such conditions as the flu, gastroenteritis, or food poisoning. Also, chronic low-level CO poisoning can occur; it’s particularly problematic for more vulnerable patients, such as children, pregnant females, and those with underlying cardiac and respiratory diseases.
CO sources
Known as the silent killer, CO is a colorless, odorless, tasteless gas. A byproduct of fossil fuel combustion, it can be emitted from furnaces, automobiles, stoves, portable generators, gas ranges, charcoal, and firewood. Other devices may emit CO when they malfunction, are blocked, or are used improperly; they include gas-powered tools (for instance, leaf blowers and concrete-cutting saws) used in enclosed or semi-enclosed spaces.
More unusual means of unintentional CO poisoning including hookah smoking, exposure to methylene chloride (a compound in aerosol sprays and paint thinners that metabolizes into CO), and riding in the back of an enclosed pickup truck.
Although CO poisoning can happen anywhere at any time, it’s most common in the fall and winter. With two-thirds of Americans heating their homes with fuel (such as gas, oil, or wood), CO poisoning is most likely to occur in residences. As of September 2015, only 36 states had laws requiring CO alarms in residential structures.
Clinical presentation, diagnosis, and treatment
When inhaled, CO competes with oxygen for binding sites on red blood cells (RBCs). It binds to hemoglobin more than 200 times more strongly than oxygen does, resulting in a compound called carboxyhemoglobin (COHb). CObound RBCs cause tissue hypoxia and cellular toxicity through immunologic and inflammatory processes. Symptom severity doesn’t necessarily reflect the CO duration or exposure level or the victim’s COHb level.
Although CO poisoning is associated with a cherry-red appearance of the skin, this actually is rare. Also, someone with CO poisoning has a normal pulse oximetry reading, because a pulse oximeter uses light and color to determine tissue saturation and can’t accurately distinguish between oxyhemoglobin and COHb. However, a fast noninvasive CO assessment can be done with a special oximeter that specifically measures how much CO is delivered to tissues.
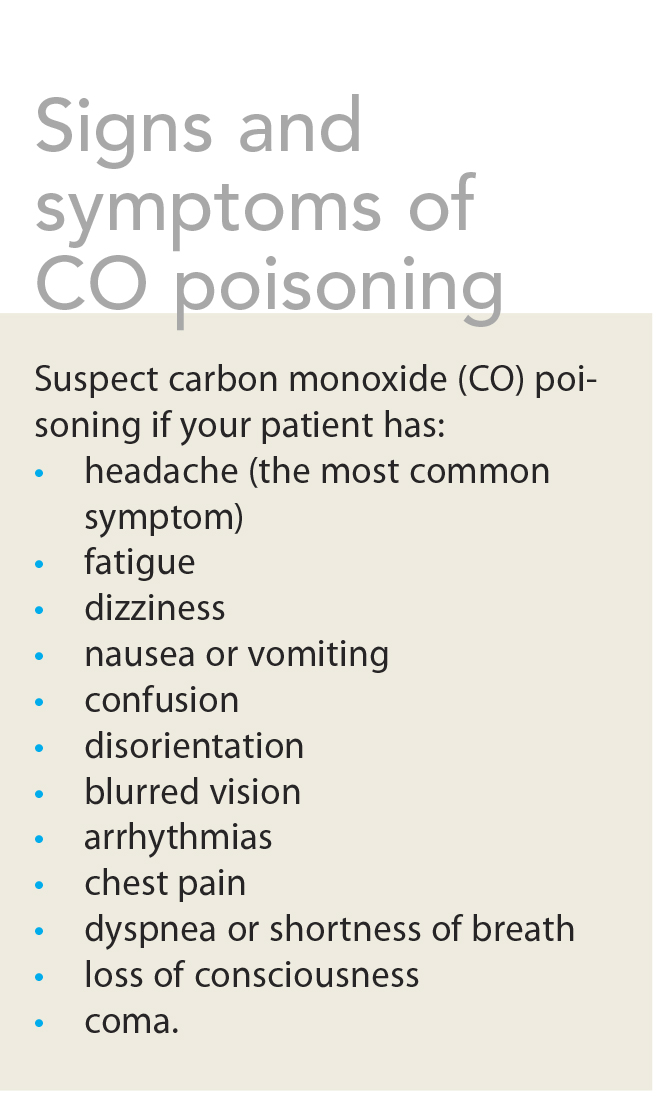
Clinical diagnosis of CO poisoning hinges on a history of CO exposure, signs and symptoms consistent with such exposure, and an elevated COHb level—usually above 3% for nonsmokers or above 10% for smokers. (See Signs and
symptoms of CO poisoning.)
Because oxygen administration hastens CO elimination from the body, first-line treatment is highflow, normobaric, 100% oxygen delivered by mask or endotracheal tube until COHb is normal (below 3%) and symptoms resolve. For exposures causing more severe manifestations (such as loss of consciousness or coronary symptoms) or a COHb level above 25%, hyperbaric oxyge therapy may be used to mitigate long-term neurologic sequelae.
Improving outcomes
You can help improve outcomes for patients who’ve been exposed to CO. In many cases, nurses are the first contact point for those with CO poisoning. Make sure you’re familiar with common signs and symptoms and maintain a high index of suspicion in patients who have these.
Rapid assessment, diagnosis, and treatment are critical in preventing long-term sequelae and death. Request that your emergency department have CO oximeters on hand to allow rapid assessment of patients who present with potential CO exposure.
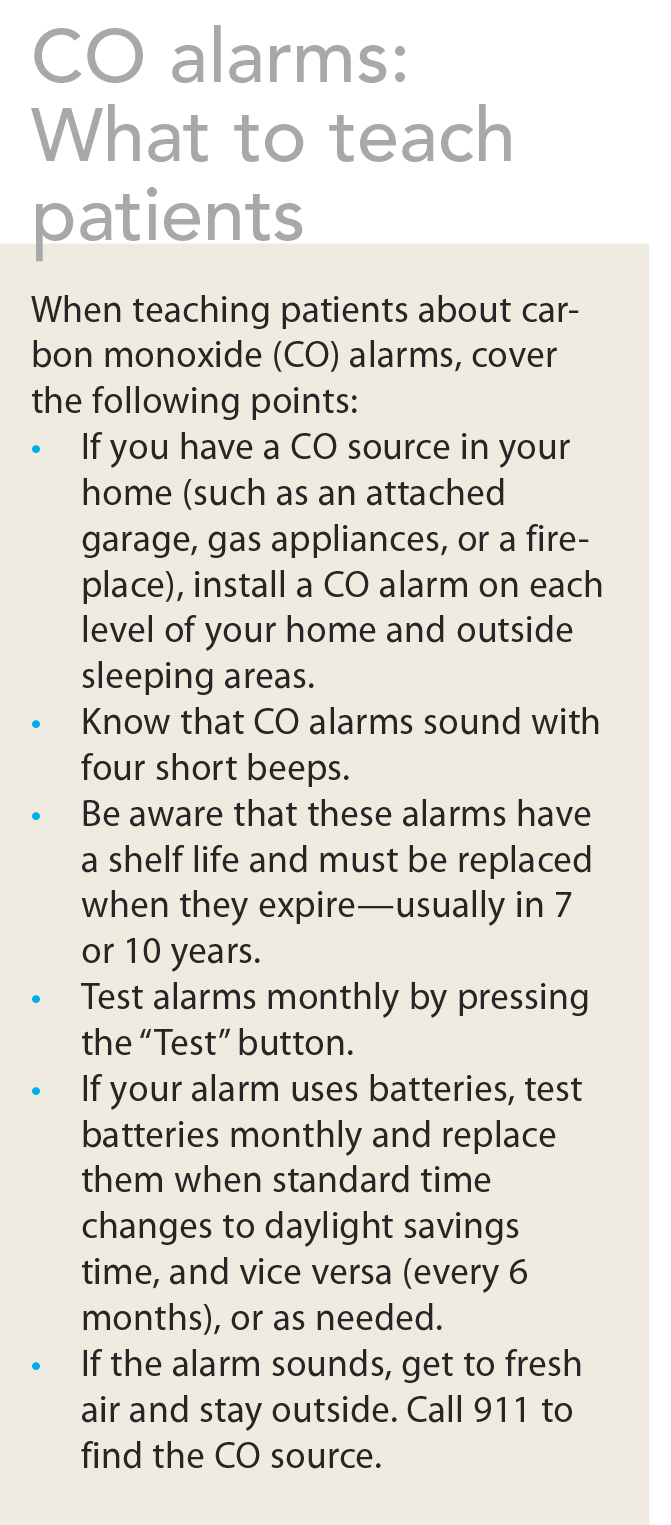
In all practice settings, use targeted patient education, including a basic overview of CO alarms, alarm placement and maintenance, and what to do if the alarm sounds. (See CO alarms: What to teach patients.)
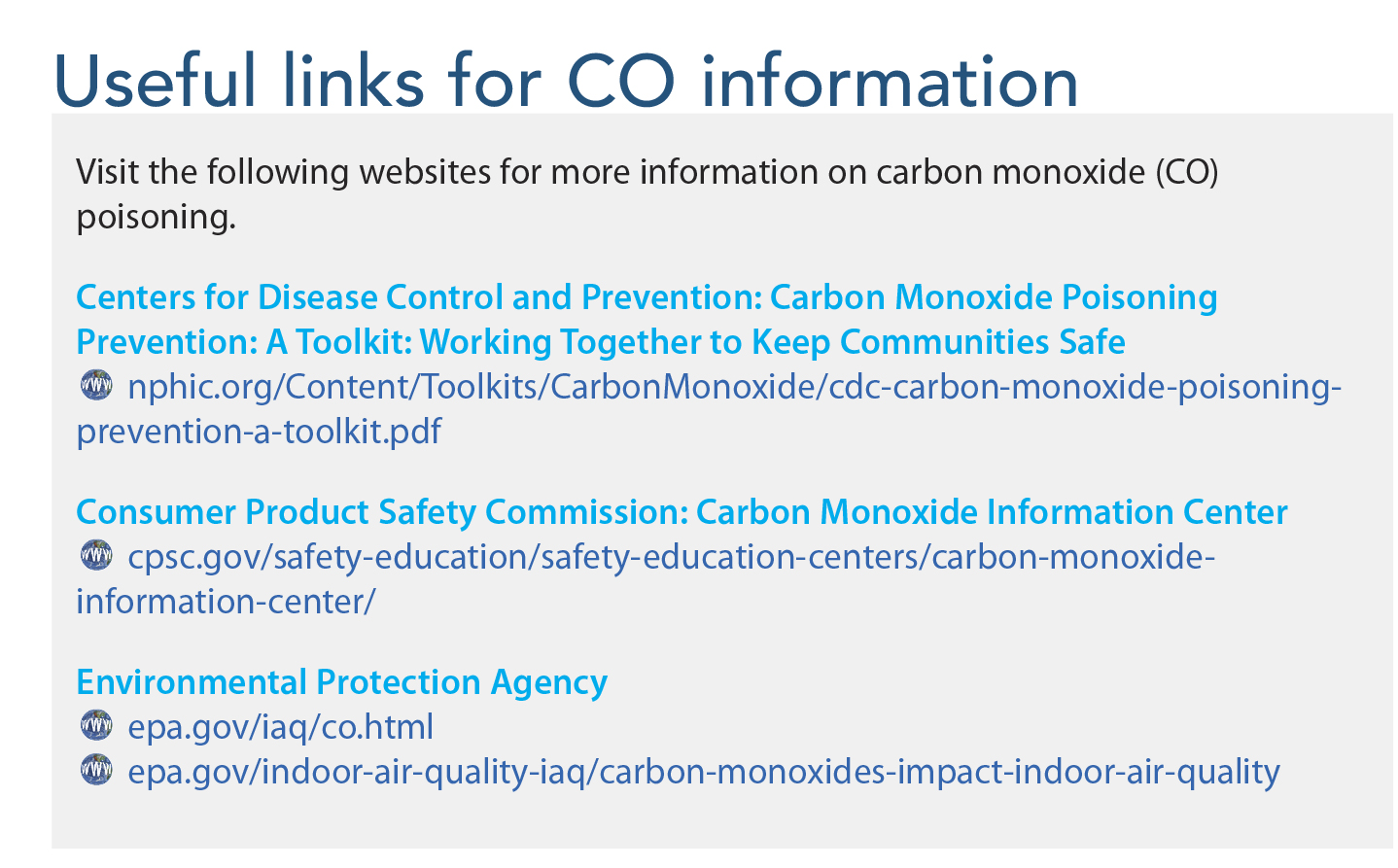
Reinforce patients’ understanding of symptoms of CO poisoning, common CO sources, and safe heating practices. These simple health-promotion tips can prevent tragedies caused by this silent killer. (For online resources, see Useful links for CO information.)
Raising public awareness
Public health measures may reduce CO exposures. Whatever your work setting, promote CO awareness and safety practices among colleagues and patients. If you’re in a leadership position, partner with fire and safety officials, first responders, and medical organizations to encourage use of CO alarms and equipment in the workplace.
Initiate conversations with community leaders and legislators to advocate for residential CO alarm requirements in city and county laws and building codes. With the help of these collaborative partners, you can increase awareness and help shape policies and procedures related to CO safety.
CO poisoning is a nationwide problem that doesn’t discriminate. Bringing about major change will require coordination with many individuals and organization—and nurses are well prepared to lead such change. As the largest and most trusted workforce in the country, we can make a difference.
The authors work at the University of South Carolina College of Nursing in Columbia. Amber Proctor Williams is a clinical associate professor. RobinDawson Estrada is an assistant professor.
Selected references
Ashurst JV, Urquhart M, Cook, MD. Carbon monoxide poisoning secondary to hookah smoking. J Am Osteopath Assoc. 2012;112(10):686-8.
Centers for Disease Control and Prevention. Carbon monoxide poisoning: Frequently asked questions. Last updated December 30, 2015.
Hampson NB, Piantadosi CA, Thom SR, Weaver LK. Practice recommendations in the diagnosis, management, and prevention of carbon monoxide poisoning. Am. J Respir Crit Care Med. 2012;186(11):1095-101.
National Conference of State Legislators. Carbon monoxide detector requirements, laws and regulations. Last updated October 1, 2015.
OSHA/NIOSH Hazard Alert: Methylene chloride hazards for bathtub refinishers. Last updated June 6, 2014.

















{kind=link}
{kind=link}
{kind=link}
1 Comment.
Too bad it wasn’t opioids. The CDC would be all over that.
I didn’t realize it was so prevalent until it happened to someone I knew and one of my brother’s coworker.