
Nurses have an important role to play in identifying and managing dental infections.
Takeaways:
- Dental abscesses are common dental emergencies.
- Dental abscesses may result in sepsis.
- Dietary sugars are the primary contributor to dental caries.
More than half of all dental emergencies not caused by trauma are related to dental abscesses and accompanying tooth pain. A dental abscess is a pocket of infection, typically located around the tooth apex, commonly caused by untreated dental caries. Symptoms include a persistent throbbing toothache that radiates to the jawbone or neck, ear pain, and cheek, face, or jaw swelling. Patients frequently report tooth sensitivity to hot and cold temperatures and discomfort with biting or chewing. Some patients experience foul-smelling or foul-tasting salty fluid in the oral cavity. Individuals with longstanding toothache or dental abscess may present with fever and malaise. During patient assessment, healthcare providers may palpate tender, swollen lymph nodes under the jaw or neck. If the abscess ruptures, the patient may experience pain relief.
Timely evaluation and evidence-based treatment are important to prevent potentially life-threatening complications of dental infection. (See Dental infections: Scope of the problem.) This article presents a case study to highlight the importance of routine oral care to reduce morbidity and mortality associated with dental infections.
When a dental infection occurs, the responsible pathogens can travel from the pulp to the bone and surrounding tissues, invading the bloodstream. According to a data brief from the National Health and Nutrition Examination Survey (2011-2012):
- 91% of U.S adults age 20 to 64 had dental caries.
- 27% had untreated dental caries.
- Dental caries is the single most common chronic disease of childhood.
A 9-year study (from 2000 to 2008) by Shah and colleagues highlighted the serious consequences of untreated periapical abscesses:
- 61,439 hospitalizations were attributed to periapical abscess.
- The mean length of stay was 2.96 days.
- 66 patients died in the hospital.
Sources: Centers for Disease Control and Prevention, Shah et al.
Case description
Tom Sanders* arrives in the emergency department (ED) with complaints of a toothache and general malaise. He says he’s short of breath, and his blood glucose levels have been routinely over 400 mg/dL. Mr. Sanders, who is 55 years old, has a history of depression, hypertension, hyperlipidemia, and type 2 diabetes.
History of present illness
Mr. Sanders, a commercial motor vehicle operator, says he thinks he broke a tooth about a month ago, but because he was beginning a coast-to-coast transport in his tractor trailer he didn’t seek dental treatment. Over time, Mr. Sanders developed mild tooth and jaw pain and tooth sensitivity to hot and cold food and drink. He’s noticed swelling around the gumline, a foul odor, and a salty taste coming from the area. Recently, the jaw pain became severe, extending into his left ear, and he noticed swelling under his jaw. He reports not feeling well and that he’s “uncomfortable” and “chilly.” He’s been taking 400 mg of ibuprofen three times a day for the tooth pain with only minimal relief.
History and medications
Mr. Sanders has been previously diagnosed with depression, hypertension, hyperlipidemia, and type 2 diabetes. He wears a bilevel positive airway pressure (BiPAP) machine for sleep apnea. Because of finances and time constraints, he hasn’t seen a dentist in many years and has a history of poor oral hygiene. Mr. Sanders’ medications include 7.5 mg of amlodipine every morning, 30 mg of duloxetine twice a day, 500 mg of metformin twice a day, and 5 mg of rosuvastatin at bedtime.
Personal and social history
Mr. Sanders is married and has two sons (21 and 24 years old). He lives in the country on several acres of land. Mr. Sanders reports that he has smoked cigarettes for about 15 years. He drinks several beers (five to six) most evenings each week when not on the road. His hobbies include going to the movies with his wife and restoring old cars.
Assessment
Mr. Sanders is 5’10” and weighs 240 pounds. His temperature is 100.9° F (38.3° C), heart rate 102 beats per minute, blood pressure 94/74 mmHg, respiratory rate 22 breaths per minute, oxygen saturation 90% on room air, and fasting blood glucose of 380 mg/dL. On a scale from 0 to 10, he rates his pain as 8. The affected tooth is number 21, the lower left first bicuspid. A small crack with a missing portion of the tooth is noted. The lower left side of his jaw is swollen and tender on palpation. Significant intraoral and extraoral swelling and gingival erythema are noted with anterior cervical lymphadenopathy. (See What to look for.)
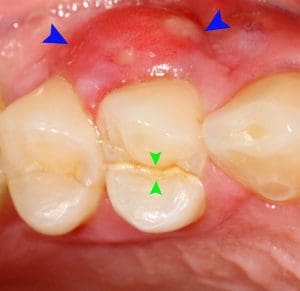
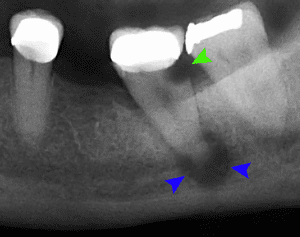
The images below are examples of what might be found during patient assessment. The top image shows a cracked tooth (green arrows) and a lateral periodontal abscess (blue arrows). The second image (X-ray) shows tooth decay (green arrows) and abscess (blue arrows). Both images are courtesy of Coronation Dental Specialty Group, 2014.
Discussion
When bacteria invade and infect a tooth, a periodontal pocket (abscess) develops as biofilm accumulates. The biofilm occupies the narrow spaces surrounding the tooth, and bacteria enter the pulp chamber and root canals. This process can occur with or without pain. Without intervention, the bacteria continue down the root canal and deposit toxic waste in the space surrounding the tooth, resulting in a pus-filled abscess. The acute inflammation may then cause increasingly noticeable signs and symptoms and eventually penetrate the surrounding facial tissues and structures, leading to severe infection, sepsis, and possibly death.
Etiology and pathogenesis
Abscesses most commonly are caused by tooth decay, a break or crack in the tooth, or a failed root canal. These predisposing factors can be diagnosed early in people who receive routine dental care. However, regular professional dental care frequently is a luxury that patients, such as Mr. Sanders, can’t afford. An estimated 130 million adults and children in the United States lack dental coverage. Nurses, nurse practitioners (NPs), and other members of a multidisciplinary care team who suspect dental neglect and perform a simple oral examination may identify an opportunity for early intervention. Healthcare providers also can help patients identify factors (such as smokeless tobacco use, poor brushing and flossing, and certain prescription medications) that may predispose them to tooth decay and gum disease.
Mr. Sanders has several factors that may have contributed to his poor dentition. For example, some of the medications he’s taking—antihypertensives, diuretics, and serotonin-norepinephrine reuptake inhibitors—are associated with xerostomia (dry mouth). The reduced saliva caused by these medications robs the oral cavity of one of its greatest protective mechanisms to combat tooth decay. Smoking also has an impact on oral health. The heat from smoking combined with nicotine contribute to blood vessel vasoconstriction, reducing blood flow and diminishing immune function, which contributes to oral bacteria proliferation. And positive airway pressure devices, such as BiPAP machines, may dry the oral mucous membranes and contribute to dental problems.
Mr. Sanders’ occupation requires long hours and living conditions that may result in making poor food choices, drinking caffeinated beverages with significant amounts of sugar and acid, and neglecting his oral care. Poor dentition commonly is attributed to a lack of proper oral hygiene practices and failure to obtain routine dental cleanings. In addition, poor oral health is related to diabetes, coronary artery disease, and metabolic syndrome. The mechanisms aren’t clearly understood, but research indicates that chronic inflammation may play a role in oral and systemic health. When an oral infection becomes systemic, it’s difficult to treat and may require aggressive, costly, time-consuming measures. In Mr. Sanders’ case, he also may suffer lost wages because of illness severity.
Dental caries and periapical abscesses generally aren’t life-threatening, but oral infections can spread rapidly, placing patients at risk for sepsis and airway compromise when left untreated. Pathogens generally responsible for dental abscess include the strict anaerobes Prevotella and Fusobacterium species as well as facultative anaerobes such as viridans group streptococci and Streptococcus anginosus.
Treatment
The primary goal of dental abscess treatment is infection elimination, with a secondary goal of symptom relief. Initial treatment may begin with incision and drainage of the dental abscess in a dental clinic or the ED. In some cases, a root canal to expose and clean the tooth root or a tooth extraction is required. Nurses and nurse practitioners should plan for appropriate pain control associated with this infection. If a patient presents with a fever or airway compromise related to edema, he or she may require I.V. antibiotics.
According to the most recent guidelines from the American Dental Association (ADA), antibiotics are not recommended in most clinical scenarios, and definitive, conservative dental treatment is effective for most patients who are immunocompetent. The ADA recommends antibiotics in patients who have signs of systemic infection, such as fever and malaise. If the patient is immunocompromised or the risk for systemic progression is high, antibiotic therapy may be warranted but is not without risk.
Choosing an antibiotic should include considering local bacterial resistance patterns, patient allergies, and other patient conditions. Antibiotics used to treat gram-negative bacteria, strict anaerobes, and facultative anaerobes typically are appropriate for treating a dental infection. Oral amoxicillin 500 mg, three times per day for 3 to 7 days remains the regimen of choice. If the patient has a penicillin allergy without life-threatening symptoms (such as anaphylaxis, angioedema, or hives), oral cephalexin 500 mg, four times per day for 3 to 7 days may be ordered. For patients who experience life-threatening allergy symptoms, oral azithromycin 500 mg on day 1, followed by 250 mg for an additional 4 days should be substituted. Oral clindamycin also may be used for patients with penicillin allergies, but Clostridioides difficile infection risk increases. (View an algorithm for antibiotic use from the ADA here.)
Dental abscess pain rarely responds to analgesic agents. And although pain is a predominant sign of abscess, the elderly, people who’ve been treated with glucocorticoids, and those with diabetes may have a reduced pain response. Providers should exercise caution and adhere to best practices when considering analgesia for dental conditions. Evidence suggests that nonsteroidal anti-inflammatory drugs plus 1,000 mg of acetaminophen may be effective and less harmful than opiates. The lowest effective dose and shortest duration should be ordered for temporary dental pain relief. The goal of acute pain control should never be to eliminate pain but rather to reduce it to a tolerable level.
Nurses’ role
Early intervention and prevention are vital to good oral health and reducing dental infection risk. Nurses should have a basic understanding of the Universal Numbering System (American system) so they can accurately identify tooth position when consulting with dental professionals on behalf of patients. (See Dental basics.)
In addition, nurses and patients should be aware of the scientific link between free sugars and dental caries. Acid-producing bacteria, poor oral hygiene, and other factors play a role in cariogenic processes, but free sugars (specifically, sucrose) are necessary for dental caries development. Nurses should educate patients about reducing their sugar intake and the important supportive role of good oral hygiene and fluoride.
Early recognition and diagnosis of sepsis is critical. A high level of suspicion coupled with consultation from skilled nurse colleagues and members of the care team is imperative. Regardless of the presenting disease process, viral and bacterial infections can lead to an overactivation of the immune cascade and result in poor patient outcomes or death. Vigilance can help prevent a lengthy hospital stay and ensure patients emerge from their experience with knowledge to improve their oral health.
Culture, education, socioeconomic status, and other social determinants of health have been shown to contribute to poor dental health outcomes. Complete medical histories that include dietary habits and oral hygiene practices will help identify barriers to good oral health so nurses can help patients establish affordable and manageable nutrition and oral care regimens.
Basic knowledge of dental anatomy and the Universal Numbering System (American system) helps nurses accurately and efficiently communicate with dental professional team members on behalf of patients.

Patient outcome
Mr. Sanders was admitted for I.V. fluids, antibiotic therapy, and to initiate insulin. To rule out descending infection or airway compromise, an X-ray and magnetic resonance imaging of the head were ordered. His complete blood count showed an increased neutrophil count. He was started on ampicillin-sulbactam 3 g I.V. every 6 hours and oral metronidazole 500 mg, three times daily for 7 days. His pain was managed with acetaminophen and ibuprofen. Mr. Sanders was placed on 2 liters of oxygen via nasal canula and started on long- and short-acting insulins. A consult for social services, diabetes education, and a follow-up appointment with endocrinology were ordered. His vital signs returned to normal, and his blood glucose improved. Mr. Sanders was discharged after 48 hours to the care of an oral surgeon. Due to the cost of care, Mr. Sanders opted for tooth extraction rather than a root canal.
Erik Southard is a professor and DNP program director, Emily Cannon is an assistant professor, and Renee Bauer an associate professor at the School of Nursing, Indiana State University in Terre Haute. Rebekah Southard is a registered dental hygienist at Villarreal Dental in Terre Haute.
*Name is fictitious.
References
Bernstein J, Gebel C, Vargas C, et al. Integration of oral health in the well-child visit at federally qualified health centers: Study of 6 clinics, August 2014-March 2015. Prev Chronic Dis. 2016;13:E58.
Centers for Disease Control and Prevention. National Center for Health Statistics. Data Brief 197: Dental Caries and Tooth Loss in Adults in the United States, 2011-2012. cdc.gov/nchs/data/databriefs/db197_table.pdf
Durso SC. Oral manifestations of disease. In: Jameson JL, Fauci AS, Kasper DL, Hauser SL, Longo DL, Loscalzo J, eds. Harrison’s Principles of Internal Medicine. 20th ed. New York: McGraw-Hill Education; 2018.
Hodgdon A. Dental and related infections. Emerg Med Clin North Am. 2013;31(2):465-80.
Lockhart PB, Tampi MP, Abt E, et al. Evidence-based clinical practice guideline on antibiotic use for the urgent management of pulpal- and periapical-related dental pain and intraoral swelling: A report from the American Dental Association. J Am Dent Assoc. 2019;150(11):906-21.
Mayo Clinic. Tooth abscess. mayoclinic.org/diseases-conditions/tooth-abscess/symptoms-causes/syc-20350901.
Sanders JL, Houck RC. Dental abscess. StatPearls [Internet]. June 30, 2019. ncbi.nlm.nih.gov/books/NBK493149
Shah AC, Leong KK, Lee MK, Allareddy V. Outcomes of hospitalizations attributed to periapical abscess from 2000 to 2008: A longitudinal trend analysis. J Endod. 2013;39(9):1104-10.
Sheiham A, James WP. Diet and dental caries: The pivotal role of free sugars reemphasized. J Dent Res. 2015;94(10):1341-7.
Siqueira JF Jr, Rôças IN. Microbiology and treatment of acute apical abscesses. Clin Microbiol Rev. 2013;26(2):255-73.
WebMD. Dental health and dry mouth. webmd.com/oral-health/guide/dental-health-dry-mouth#1

















