
A progressive degenerative disease, Parkinson disease (PD) is marked by tremor, slow movement, stiffness, and balance problems. It affects about 1 million Americans—more than amyotrophic lateral sclerosis, multiple sclerosis, and muscular dystrophy combined.
Patients with PD are admitted to hospitals at higher rates than the general population and have longer stays. Medication mismanagement is the most common complication of their hospitalization. Three in every four don’t receive their medications on time, resulting in potentially serious consequences. Many worry they’ll have exacerbations of “wearing off” symptoms if they get their medications late. (Wearing off means a return of Parkinson symptoms, which increases the risk for falls and other mishaps.) What’s more, certain medications commonly prescribed during hospitalization can worsen PD symptoms.
To promote good outcomes, you must be knowledgeable about nursing care for these patients— especially PD medications and how to manage the hospital medication regimen. To help ensure safe, effective care and appropriate medication therapy, be sure to reconcile patients’ medications and assess their swallowing and fall risk.
Causes
Experts don’t fully understand what causes PD, but they suspect a multifactorial combination of age, environment, and heredity.
• Advanced age: PD is most commonly diagnosed in people older than age 60.
• Environment: Some pesticides, solvents, and heavy metals are strongly linked to PD, as is traumatic brain injury.
• Heredity: Someone whose parent had PD has slightly higher odds of developing PD than the general population. Also, certain genes have been linked to PD.
Pathophysiology and assessment
In PD, dopamine-producing neurons in the brain’s substantia nigra decrease. Eventually, dopamine production drops below a certain threshold.
Early PD signs and symptoms are subtle and come on gradually. As the disease progresses, tremor may begin to interfere with daily activities. Classic motor symptoms include tremor, bradykinesia (slow movement), rigidity or stiffness, poor balance, and incoordination. Those affected may have difficulty walking, talking, or completing simple tasks.
Some patients also have nonmotor symptoms, such as depression and anxiety; slowed thinking; moodiness, loss of smell; pain; hypotension; difficulty swallowing, chewing, and speaking; urinary problems; constipation; skin problems; and sleep disruption. Researchers believe many years of nonmotor symptoms occur before the classic triad of motor symptoms (tremor, bradykinesia, and rigidity) leads to PD diagnosis.
Medications for PD
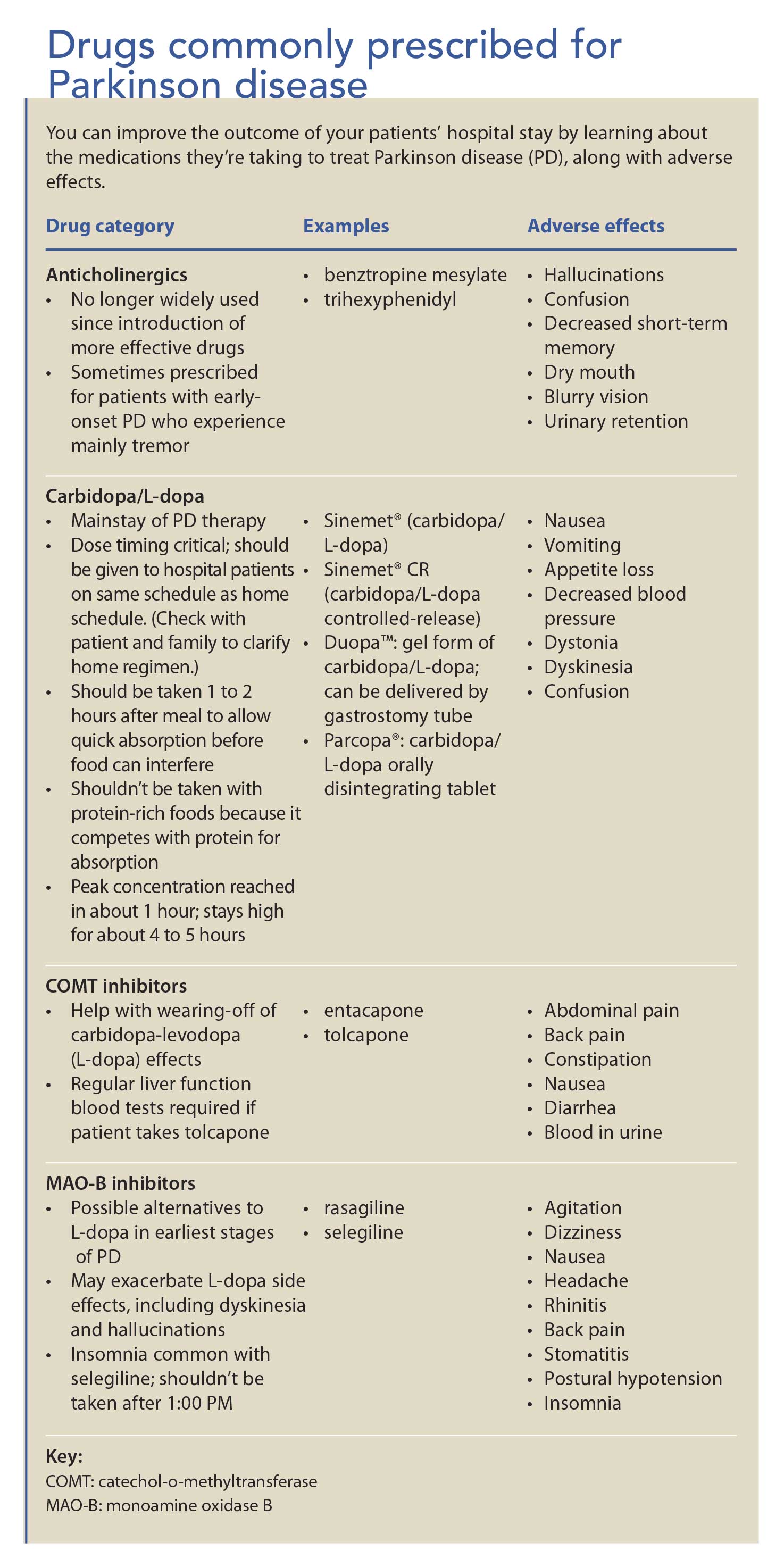
PD medications fall into five general categories.
• Carbidopa-levodopa (L-dopa), the mainstay of PD medications, is a combination drug. L-dopa crosses the blood-brain barrier, where it’s converted to dopamine. Carbidopa doesn’t cross this barrier; instead, it helps block L-dopa breakdown before it enters the brain, making more L-dopa available for transport to the brain.
• Dopamine agonists (such as apomorphine, ropinirole, and pramipexole) mimic the effects of dopamine.
• Monoamine oxidase B inhibitors (such as selegiline) block an enzyme that breaks down Ldopa.
• Catechol-o-methyltransferase inhibitors (such as entacapone and tolcapone) inhibit an enzyme that degrades dopamine, prolonging its effect and easing wearing-off symptoms.
• Anticholinergics enhance the activity of acetylcholine, a neurotransmitter that regulates movement and memory. (See Drugs commonly prescribed for Parkinson disease.)
Some patients also may be prescribed miscellaneous drugs, such as:
• droxidopa, a synthetic norephinephrine precursor that raises
blood pressure
• rivastigmine tartrate, which slows acetylcholine breakdown and may help treat mild to moderate dementia associated with PD.
Factors that affect medication choices and dosages include the patient’s age and signs and symptoms. Be aware that nausea is a major side effect of many PD medications. It can be so troublesome that some patients decide not to take their medications.
Medication and mealtimes: A coordinating act
Take the time to understand your patient’s specific medication regimen and meal schedule. Patients may have individualized schedules for medication and meals, which may differ dramatically from standard hospital schedules. At home, patients typically customize their medication schedules to their lifestyle; some may take PD medications as often as every 2 hours. For an early riser, a four-timesdaily dosing schedule may mean 6 A.M., 11 A.M., 4 P.M., and 9 P.M., which aren’t typical hospital administration times. Many patients become highly dependent on their at-home schedule.
Work with your patient, the hospital pharmacy, and the patient’s physician to establish a medication schedule as close as possible to the patient’s home schedule. Also, make every attempt to administer drugs at consistent times. Know that PD medications must be given at specific times, not simply within the common hospital window of an hour before to an hour after the scheduled time.
Dietary tips for patients with PD
Certain medications (consult a pharmacist as to which ones) should be taken 30 minutes before or 1 to 2 hours after a protein meal to allow the drug to reach the small intestine and absorb faster. Although an empty stomach aids medication absorption, some PD medications can cause nausea. To help prevent nausea, give a carbohydrate snack (such as crackers, toast, oatmeal, or applesauce) with the medication. Some patients find ginger tea also helps.
Because L-dopa competes for dietary protein absorption, patients generally should avoid protein-rich meals around the same time as L-dopa doses. Some may follow a protein redistribution diet similar to this:
• They eat meat, fish, and other protein foods at dinner, because they’re typically sedentary after dinner.
• They eat meals based mainly on grains, fruits, and vegetables during the day, when they generally want to be active and need the benefits of L-dopa the most.
Constipation, a nonmotor symptom of PD, may be exacerbated by such medications as opioid analgesics, diuretics, and iron supplements. To help patients avoid constipation, encourage them to drink water (as medically advised); eat dietary sources of fibers, such as vegetables, whole grains, and fruits; and take a daily stool softener and fiber supplement as appropriate.
Preventing drug interactions
Many common medications given in the hospital interact with PD medications to cause distressing effects. Double-check your patient’s medication list for problematic combinations. Be aware that the following medications can interact with PD drugs.
• Metoclopramide, prochlorperazine, and promethazine (commonly prescribed to treat nausea) are dopamine antagonists and can worsen PD signs and symptoms.
• Haloperidol, risperidone, olanzapine, and most other typical or atypical neuroleptic medications can cause confusion and may worsen motor symptoms of PD.
• Benzodiazepines, such as lorazepam, alprazolam, and clonazepam, can cause confusion and worsen balance difficulties.
• Diphenhydramine can cause confusion.
• Opioids can cause confusion and worsen balance problems.
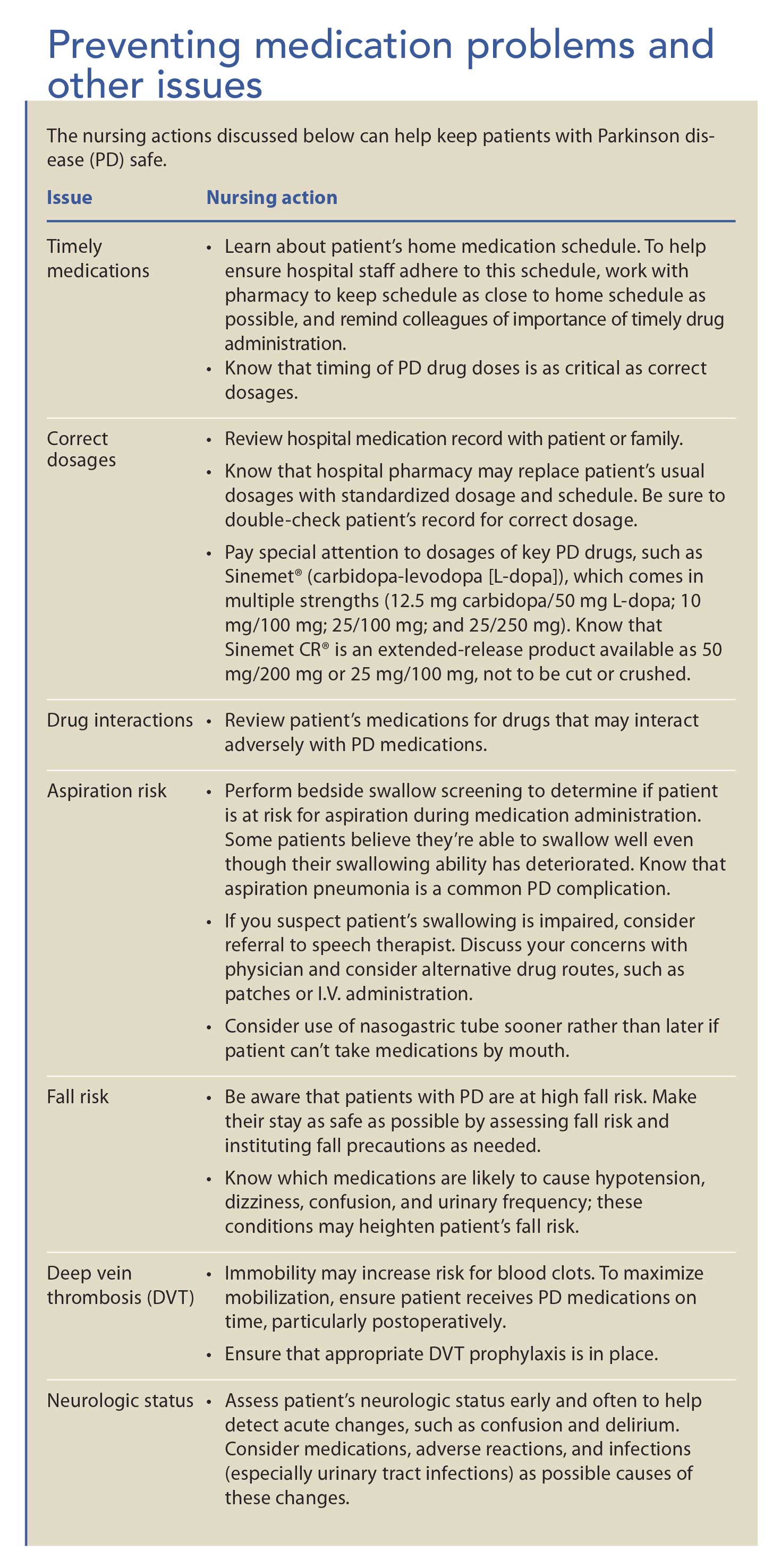
A patient with PD who receives opioids requires extra nursing vigilance. If possible, administer nonopioid analgesics, such as acetaminophen or ibuprofen, instead. (See Preventing medication problems and other issues.)
Listen to your patient
Many patients with PD are well-informed about their disease and medications. In some cases, they and their families know more about the disease and treatment than hospital clinicians. You can help them avoid complications of hospitalization by taking the time to listen to them, learn about their medications and special needs, and communicate their concerns and requests to other healthcare care team members.
The authors work in the department of nursing and health sciences at California State University East Bay in Hayward. Dorothy J. Moore is an adjunct lecturer, Bonnie M. Smith is a lecturer and Maria H. Cho is an assistant professor. Moore also is an emergency department staff nurse at Kaiser Permanente Oakland Medical Center in Oakland, California.
Selected references
Aminoff MJ, Christine CW, Friedman JH, et al; National Parkinson Foundation Working Group on Hospitalization in Parkinson’s Disease. Management of the hospitalized patient with Parkinson’s disease: current state of the field and need for guidelines. Parkinsonism Relat Disord. 2011;17(3):139-45.
Gerlach OH, Broen MP, van Domburg PH, Vermeij AJ, Weber WE. Deterioration of Parkinson’s disease during hospitalization: survey of 684 patients. BMC Neurol. 2012;12:13.
Parkinson’s Disease Causes. The Michael J. Fox Foundation for Parkinson’s Research.
Relationship between protein and L-dopa. Interaction animation. Live Well With Parkinson’s.
Span P. Hospital dangers for patients with Parkinson’s. The New York Times. April 17, 2013.
Treatment of Parkinson’s disease. 2013. WearingOff.

















{kind=link}
{kind=link}
1 Comment.
My sister is 61 years and has been suffering from PD for the past 6years. Lately her condition started hallucinating and I did not know how to handle the situation. She could not sleep and tried to find and catch the imaginary people who she thinks are real, she had tremors for several years and was gradually becoming worse before we found PD herbal supplement from totalcureherbsfoundation.com that was able to get rid of her disease and alleviate all symptoms within the short period of her 15 weeks of usage.