Early recognition and prompt action achieve a positive outcome.
- Atelectasis occurs in 90% of patients who receive general anesthesia.
- Partial or complete collapse of the lungs’ small airways impair gas exchange.
- Chest physiotherapy can loosen accumulated mucous.
Gus Kelly*, age 72, is recovering from surgical repair of a large ventral hernia, which took place 2 days ago. When his nurse, Kim Jones, checks on Mr. Kelly after breakfast, he appears confused. His RR is 32 breaths per minute, and his SpO2 is 84% on 2 liters of oxygen per minute via nasal cannula. This decrease from 98% prompts Kim to activate the rapid response team (RRT).
History and assessment
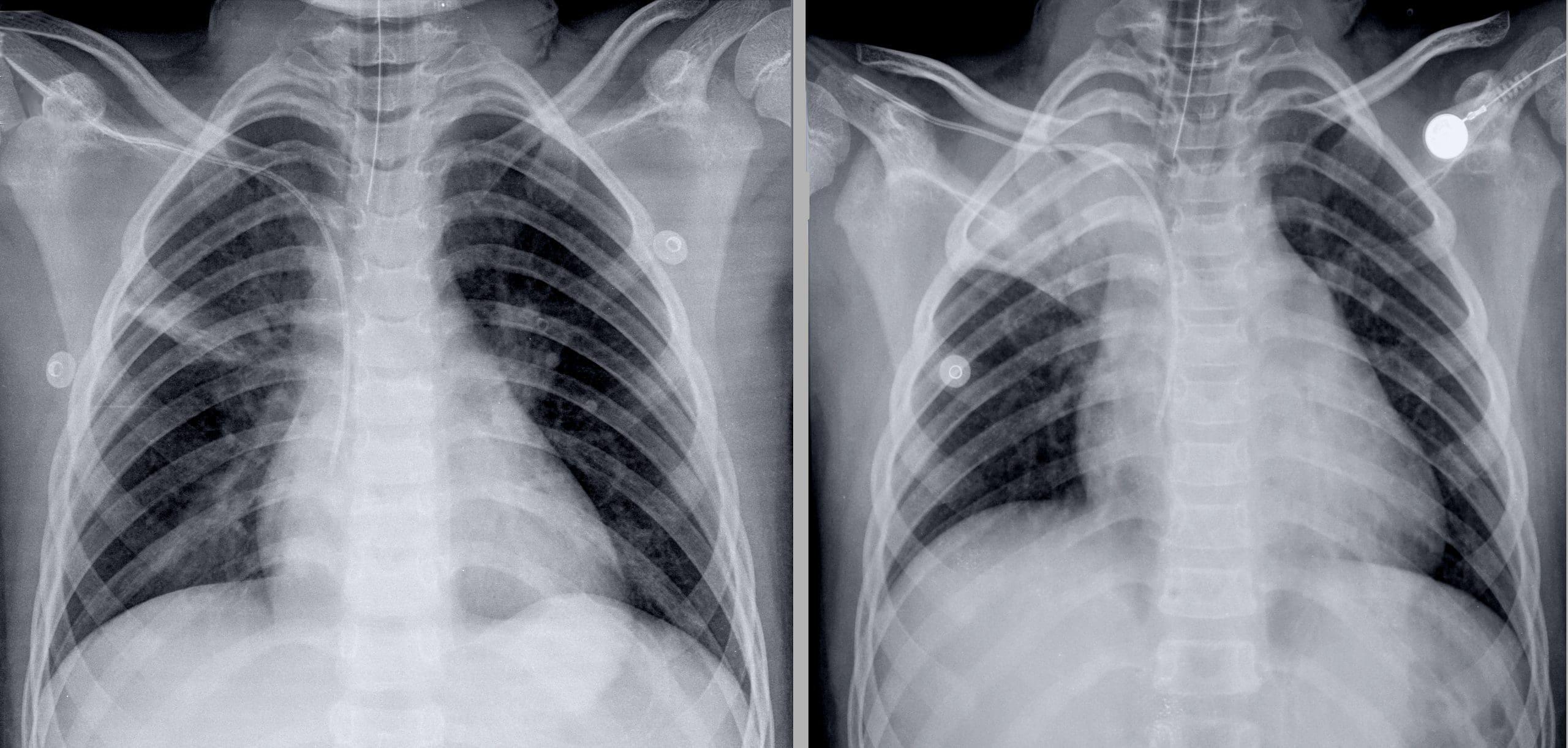
As the RRT nurse, you take Mr. Kelly’s vital signs: temperature 100.4° F (38° C), HR 134 bpm, RR 32 breaths per minute, BP 158/94 mmHG. You note that Mr. Kelly appears anxious and confused and that he’s using accessory muscles to breathe. Upon auscultation, you note that he has diminished breath sounds with coarse crackles bilaterally. He also has a weak cough. A bedside chest X-ray reveals bilateral atelectasis.
Taking action
You place Mr. Kelly on a non-rebreather mask with 100% oxygen concentration and connect him to the cardiac monitor, which shows sinus tachycardia. You and Kim perform chest physiotherapy to help Mr. Kelly cough up secretions blocking his airway. After he coughs up yellow secretions, his SpO2 improves to 98%. You wean him to 6 liters of oxygen via nasal cannula and check his vital signs, which are HR 92 bpm, RR 25 breaths per minute, and SpO2 96%.
You and Kim help Mr. Kelly to a chair and explain that increasing mobility prevents atelectasis. After weaning Mr. Kelly to 2 liters of oxygen via nasal cannula, you ask about his incentive spirometer use, coughing, deep breathing, and pain level. Mr. Kelly says that he doesn’t use the spirometer and that he doesn’t like taking pain medication. You explain that inspiratory effort opens the small airway passages in his lungs and that coughing and deep breathing will prevent future atelectasis. You also explain that managing pain will make coughing and deep breathing easier and more effective.
Mr. Kelly demonstrates proper use of the spirometer and says that he understands the other instructions you’ve provided. During proactive rounds, you’ll follow up on his progress.
Education and follow-up
Atelectasis, which occurs in 90% of patients undergoing general anesthesia, results from partial or complete collapse of the small airways of the lungs, which impairs gas exchange of carbon dioxide and oxygen. Impeded gas exchange may lead to patient confusion and anxiety, and the inability to clear increased secretions can result in further complications, including pneumonia.
Lack of mobility and an inability to cough results in increased mucous in the lungs. Chest physiotherapy or percussion can loosen accumulated mucous and help the patient cough up secretions.
Outcome
Nurses provide chest physiotherapy, and Mr. Kelly uses his incentive spirometer every hour. He’s weaned to room air, a follow-up chest X-ray shows that the atelectasis has diminished, and his breath sounds are clear. Thanks to Kim’s early recognition of the signs of atelectasis and your quick action, Mr. Kelly is discharged 4 days after surgery.
*Names are fictitious.
Elizabeth Avis and Lois Grant are rapid response nurses at Thomas Jefferson University Hospital in Philadelphia, Pennsylvania.
American Nurse Journal. 2023; 18(6). Doi: 10.51256/ANJ062350
References
Grott K, Chauhan S, Dunlap JD, Lee S. Atelectasis (nursing). StatPearls. October 12, 2022. ncbi.nlm.nih.gov/books/NBK572133/
Kotta PA, Ali JM. Incentive spirometry for prevention of postoperative pulmonary complications after thoracic surgery. Respir Care. 2021;66(2):327-33. doi:10.4187/respcare.07972
Longhini F, Bruni A, Garofalo E, et al. Chest physiotherapy improves lung aeration in hypersecretive critically ill patients: A pilot randomized physiological study. Crit Care. 2020;24(1):479. doi:10.1186/s13054-020-03198-6
Stark P. Atelectasis: Types and pathogenesis in adults. UpToDate. October 14, 2021.
Villa G, Iacopo L, Amass T, et al. Effects of psychological interventions on anxiety and pain in patients undergoing major elective abdominal surgery: A systemic review. Perioper Med (Lond). 2020;9(1):38. doi:10.1186/s13741-020-00169-x
Zhou Y, Xu M. Analysis of the effect of quality nursing after thoracic surgery. Emerg Med Int. 2022;2022:6204832. doi:10.1155/2022/6204832
Key words: postoperative atelectasis, general anesthesia, postoperative complications.


















