
Get your patients back on their feet with thorough assessments that lead to early and accurate diagnoses.
POSTURAL orthostatic tachycardia syndrome (POTS) affects over 1,000,000 Americans (80% are women of childbearing age). Since POTS was first characterized in 1993, diagnostic criteria and treatments have been established based new insights from research. However, the syndrome’s diverse symptoms and practitioners’ unfamiliarity with the illness leads to misdiagnosis and delays in appropriate treatment.
POTS, a dysfunction of the autonomic nervous system (ANS), is characterized by a group of disorders that are exacerbated upon standing (orthostatic intolerance). (See POTS defined.) Symptoms range from vague (lightheadedness, brain fog, and fatigue) to severe (complete autonomic failure and debilitation). A patient’s quality of life varies depending on the degree of impairment. About 25% of all patients diagnosed with POTS (both primary and secondary) progress to complete disability, and many experience decreased quality of life as symptoms worsen.
Without an accurate diagnosis, nurses can’t provide the education necessary to help patients cope with this syndrome. As POTS awareness grows, nurses will play a pivotal role in early diagnosis through accurate assessment, collaboration with providers and staff, and patient education.
Postural orthostatic tachycardia syndrome
Hypertension update: Implications for nursing practice
Caring for patients with a left ventricular assist device
ANS and POTS symptoms
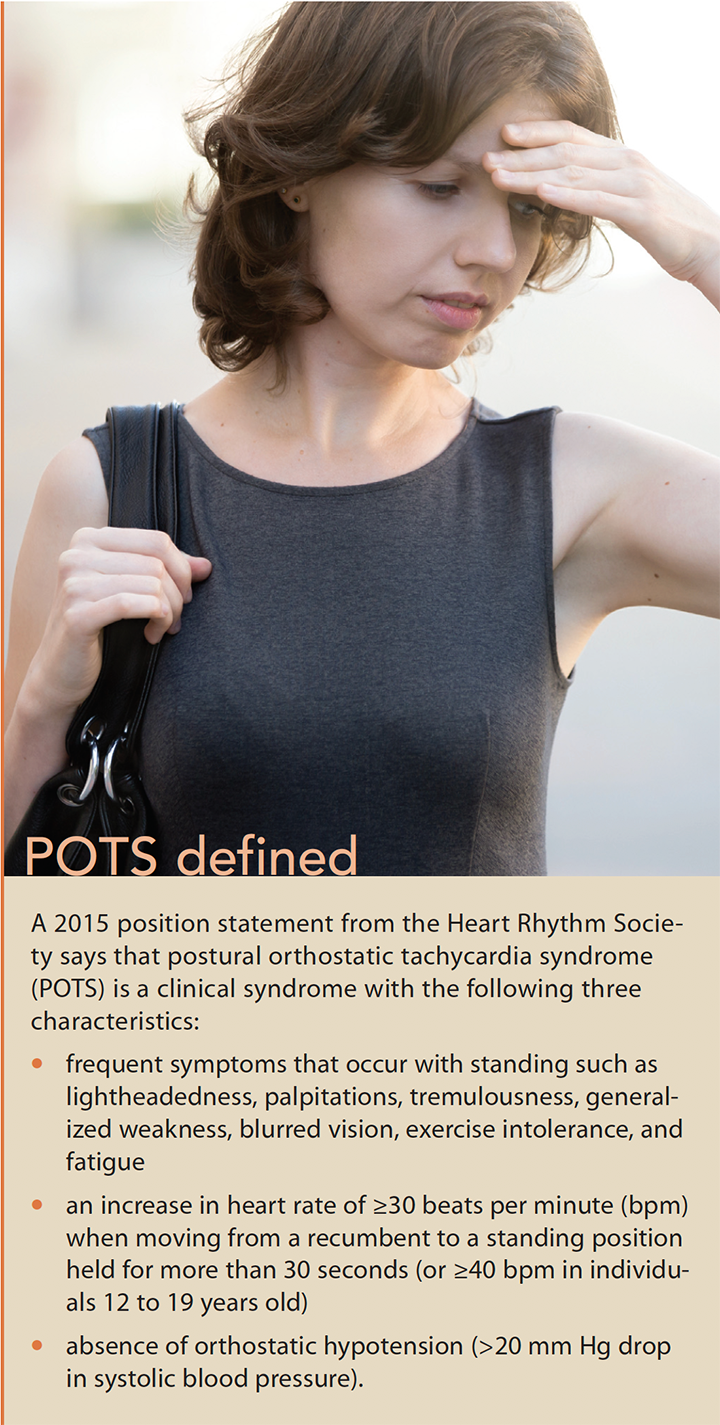 The ANS is a network of neurofibers between the brain and spinal cord that extends to the organs and peripheral nerves. It’s responsible for regulating automatic body functions, such as breathing, heartbeat, blood pressure, digestion, sexual function, and temperature control. Normally, when a person changes position from lying to standing, the body maintains blood pressure by constricting the blood vessels in the lower extremities and increasing the heart rate. With POTS, vasoconstriction and fluid regulation is abnormal, causing blood to pool in the lower extremities and reducing blood flow to critical organs. As a result, the patient experiences symptoms of tachycardia—heart palpitations, chest discomfort, weakness in the lower extremities, and fatigue. Patients may feel lightheaded or lose consciousness, but symptoms are typically relieved when the patient lies down.
The ANS is a network of neurofibers between the brain and spinal cord that extends to the organs and peripheral nerves. It’s responsible for regulating automatic body functions, such as breathing, heartbeat, blood pressure, digestion, sexual function, and temperature control. Normally, when a person changes position from lying to standing, the body maintains blood pressure by constricting the blood vessels in the lower extremities and increasing the heart rate. With POTS, vasoconstriction and fluid regulation is abnormal, causing blood to pool in the lower extremities and reducing blood flow to critical organs. As a result, the patient experiences symptoms of tachycardia—heart palpitations, chest discomfort, weakness in the lower extremities, and fatigue. Patients may feel lightheaded or lose consciousness, but symptoms are typically relieved when the patient lies down.
Dysautonomia (ANS malfunction), extends beyond the cardiovascular system, creating other less common symptoms such as tremors, brain fog, headache, difficulty sleeping, shortness of breath, and blurred vision. Patients also may report problems regulating body temperature, bowel and bladder irregularities, poor sleep quality, and an inability to tolerate exercise. In fact, the severity and disability have been compared to a patient with heart failure or chronic obstructive pulmonary disease. Many individuals with POTS become wheelchair bound or bedbound, leaving them unable to care for their families, attend school, or work. Additionally, problems such as decreased cognitive function and memory further reduce functional abilities.
Forms of POTS
POTS is a heterogenous disorder with no single cause for the variety of symptoms that present, making identification particularly difficult; symptom manifestation and severity vary based on the etiology. POTS is categorized as primary or secondary.
Primary POTS
Primary POTS includes neuropathic, hyperadrenergic, and developmental forms. Neuropathic POTS is the most common, and some statistics indicate that up to 50% of patients with POTS have experienced a recent traumatic event such as an injury, viral illness, or pregnancy prior to onset. Hyperadrenergic POTS has an autoimmune connection or a genetic predisposition, which occurs in about 25% of those affected. Developmental POTS is seen during periods of rapid growth, such as adolescence.
Overall, primary forms of POTS are associated with disruptions in peripheral neurological connections, irregular sympathetic activity, and impaired volume control. Typically, those who are diagnosed younger have a better prognosis, and the symptoms may resolve with or without treatment. For others, the symptoms may become progressively worse.
Secondary POTS
Secondary POTS occurs as a manifestation of another illness such as Lyme disease, diabetes, or cancer, and management is aimed at treating the underlying illness. Regardless of the cause of illness, proper identification is key to determining the course of treatment because most symptoms can be effectively managed with medication, diet, and lifestyle management.
Assessment and diagnosis
Many patients wait years for an accurate diagnosis. Unless a provider is familiar with POTS, attention may focus on other diagnoses, preventing accurate testing and treatment. In fact, many patients are misdiagnosed with a psychiatric disorder or are identified as having anxiety, panic attacks, or chronic fatigue. A thorough assessment, including a family history, can help avoid misdiagnosis. It should include:
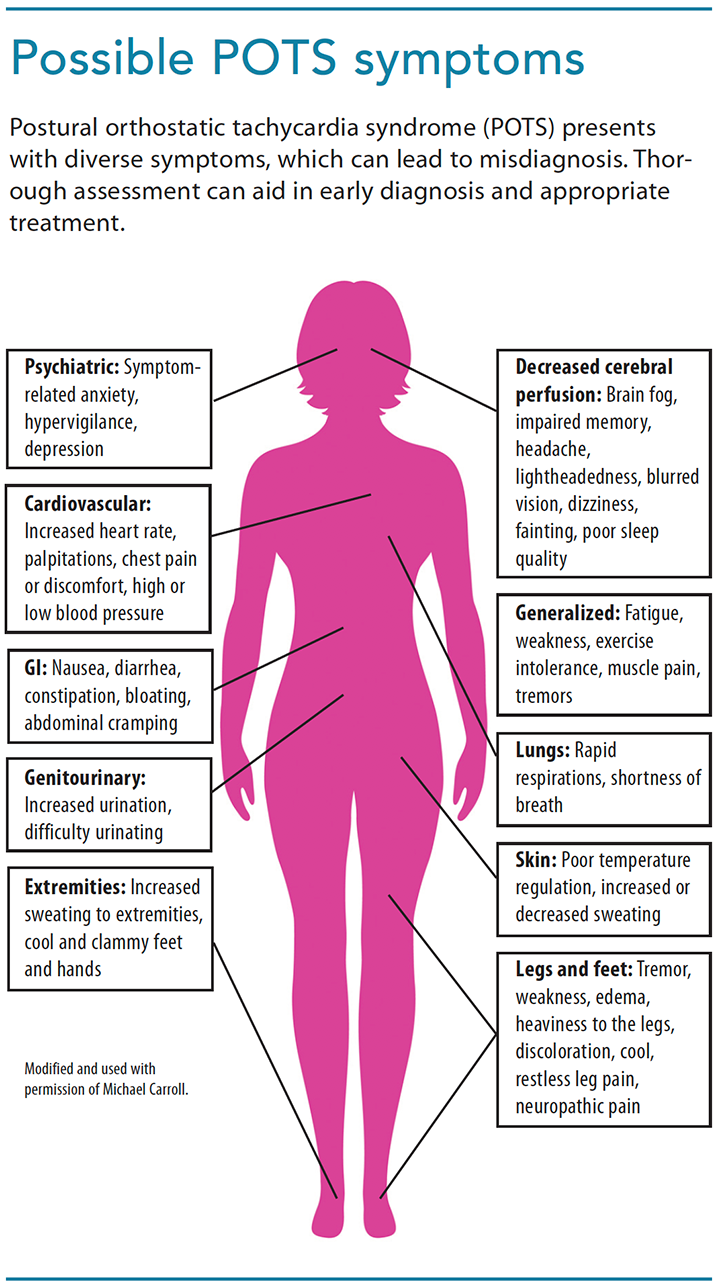
- A review of all systems. Patients won’t recognize that other less prominent symptoms may be connected to neurologic dysfunction, so they may not mention them. (See Possible POTS symptoms.)
- Neurologic and cardiovascular assessment. Assess for palpitations, tachycardia, chest discomfort, pallor, syncope, shortness of breath, brain fog, or problems with memory. In peripheral extremities, assess bilaterally for pulse strength, sensation, discoloration, temperature, excessive or decreased sweating, edema or heaviness to the legs, weakness, and tremor. To best assess whether the patient has sustained, rather than transient, orthostatic tachycardia, take the first readings after he or she has been supine for at least 5 minutes, and again after 1, 3, 5, and 10 minutes of standing.
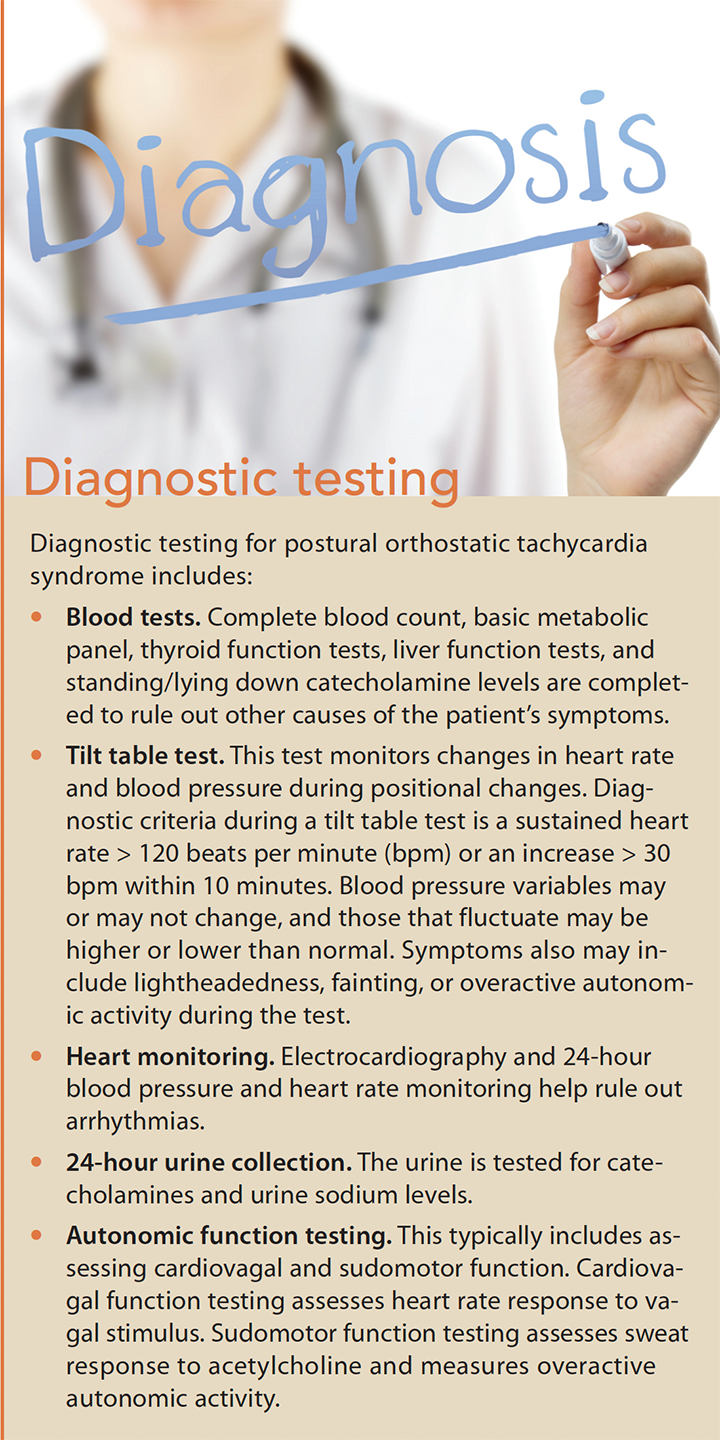
- GI and urinary assessment. Assess for constipation, diarrhea, and bloating or cramps, as well as urinating difficulty or frequency. Diagnostic testing includes blood tests, tilt table test, heart monitoring, 24-hour urine collection, and autonomic function testing. (See Diagnostic testing.)
Treatment
Individualized treatment is aimed at symptom control and improving vascular function with nonpharmacologic and pharmacologic strategies.
Nonpharmacologic interventions
Initial nonpharmacologic management includes improving volume expansion, preventing blood pooling, increasing endurance and orthostatic tolerance, avoiding triggers, and addressing psychological needs.
Improving volume expansion. Many patients with POTS have low urinary sodium levels indicative of low blood volume. Patients can expand volume by increasing their salt and fluid intake and elevating the head of the bed off the ground 4 to 6 inches.
Preventing blood pooling. Garments that, ideally, compress the calf, thigh, and lower abdomen are used to prevent blood from pooling in the lower extremities; leg compression alone tends to be less effective.
Increasing endurance and orthostatic tolerance. Strength training and aerobic exercise increase endurance and is recommended three times per week with gradual intensity. Because patients with POTS experience exercise intolerance, they’ll need adequate rest periods before and after exercise. Initially, horizontal types of exercise, such as swimming, rowing, and riding a recumbent bike, are used to avoid POTS symptoms. As patients progress, upright activities can be added.
Physical countermeasure maneuvers can help improve the patient’s orthostatic tolerance by raising arterial pressure. These maneuvers include squeezing a rubber ball, squatting, walking, or combined leg crossing and muscle tensing.
Avoiding triggers. Advise patients with POTS to avoid activities—such as prolonged standing, heat exposure, and consuming alcohol, caffeine, and large meals—that may trigger symptoms. And emphasize that if they experience symptoms, they should lie down or rest to prevent loss of consciousness or injury.
Addressing psychological needs. Although studies indicate that those with POTS typically have lower lifetime anxiety levels, many patients with POTS become hypervigilant in the presence of symptoms and experience increased stress and anxiety that affects their quality of life.
Direct interventions to both physical and psychological domains. Teach stress-reduction techniques and cognitive behavioral interventions to help patients manage symptoms and reduce fears about ongoing problems. Caregivers and family members also require education about how to support and care for their loved one. Direct patients and caregivers to agencies such as Dysautonomia International (dysautonomiainternational.org) or the Dysautonomia Foundation (familialdysautonomia. org), where they can find additional support, information about symptom management, and provider directories.
Pharmacologic management
Medications may be prescribed for severe symptoms or if nonpharmacologic treatments aren’t effective. Mineralocorticoids, antidiuretics, and hematopoietic agents help to increase blood volume; vasoconstrictors increase blood pressure; and beta-blockers decrease heart rate. Drugs such as selective serotonin reuptake inhibitors, selective norepinephrine reuptake inhibitors, clonidine, and pyridostigmine may be prescribed to facilitate cardiovascular function and synapse transmission within the neurologic system.
Early identification is key
Although POTS comes in many forms, researchers are learning more about the causes and treatments of this debilitating illness. You can help disseminate POTS awareness by educating your peers and patients. Early identification is key to treatment success because it will reduce the amount of time a patient spends seeking answers. Quicker diagnosis and treatment will increase patients’ ability to get back on their feet and return to an optimal quality of life.
Marna M. Revlock is an assistant professor at Aultman College in Canton, Ohio.
Selected references
Anderson JW, Lambert EA, Sari CI, et al. Cognitive function, health-related quality of life, and symptoms of depression and anxiety sensitivity are impaired in patients with the postural orthostatic tachycardia syndrome (POTS). Front Physiol. 2014;5:230.
Arnold AC, Ng J, Raj SR. Postural tachycardia syndrome—Diagnosis, physiology, and prognosis [published online ahead of print, 2018]. Auton Neurosci. sciencedirect.com/science/article/pii/S1566070217303545
Benarroch EE. Postural tachycardia syndrome: A heterogeneous and multifactorial disorder. Mayo Clin Proc. 2012;87(12):1214-25.
Busmer L. Diagnosis and management of postural tachycardia syndrome. Nurs Stand. 2013;27(20):44-8.
Fu Q, Levine BD. Exercise and non-pharmacological treatment of POTS [published online ahead of print, 2018]. Auton Neurosci. sciencedirect. com/science/article/pii/S1566070218300663
Kavi L, Gammage MD, Grubb BP, Karabin BL. Postural tachycardia syndrome: Multiple symptoms, but easily missed. Br J Gen Pract. 2012;62(599):286-7.
Lambert E, Lambert GW. Sympathetic dysfunction in vasovagal syncope and the postural orthostatic tachycardia syndrome. Front Physiol. 2014;5:280.
Miller AJ, Raj SR. Pharmacotherapy for postural tachycardia syndrome [published online ahead of print, 2018]. Auton Neurosci. sciencedirect. com/science/article/pii/S1566070218300250
Genetic and Rare Diseases (GARD) Information Center. Postural orthostatic tachycardia syndrome. Updated 2017. rarediseases.info .nih.gov/diseases/9597/postural-orthostatic-tachycardia-syndrome
Sheldon RS, Grubb BP, Olshansky B, et al. 2015 Heart Rhythm Society expert consensus statement on the diagnosis and treatment of postural tachycardia syndrome, inappropriate sinus tachycardia, and vasovagal syncope. Heart Rhythm. 2015;12(6):e41-63.

















