
Early diagnosis and treatment can help ensure good outcomes.
Takeaways:
- Postural orthostatic tachycardia syndrome (POTS) is characterized by too little blood return to the heart when moving from a lying or sitting to a standing position, resulting in a range of symptoms.
- POTS has various underlying causes, making diagnosis and treatment difficult.
- Nurses can play an important role in educating patients about strategies to decrease symptoms of POTS and enhance quality of life.
Mary Watson*, a 32-year-old woman, arrives at her provider’s office with complaints of dizziness, fatigue, and a rapid heart rate when changing from a sitting to a standing position. She says that her symptoms began suddenly after recovering from COVID-19, which she contracted 3 months previously. Her symptoms during the infection included fever, headache, cough, and fatigue for a couple of weeks. She treated herself at home with ibuprofen for headache and fever, fluids, and rest.
Ms. Watson exhibits distress as she explains how these new symptoms have disrupted her life. She can’t work, exercise, or care for her family. The provider notes that, when seated, Ms. Watson’s heart rate (HR) is 86 beats per minute (bpm) and her blood pressure (BP) is 114/86 mmHg. Upon standing, Ms. Watson’s HR increases to 120 bpm and her BP drops to 109/85 mmHg. The provider suspects that the patient may be suffering from postural orthostatic tachycardia syndrome (POTS) as a result of COVID-19, but must conduct additional diagnostic tests before making any conclusions and determining treatment options.
Atrial fibrillation: Recognition and management to improve quality of life
Postural orthostatic tachycardia syndrome
Attacking anterior-wall myocardial infarction in time
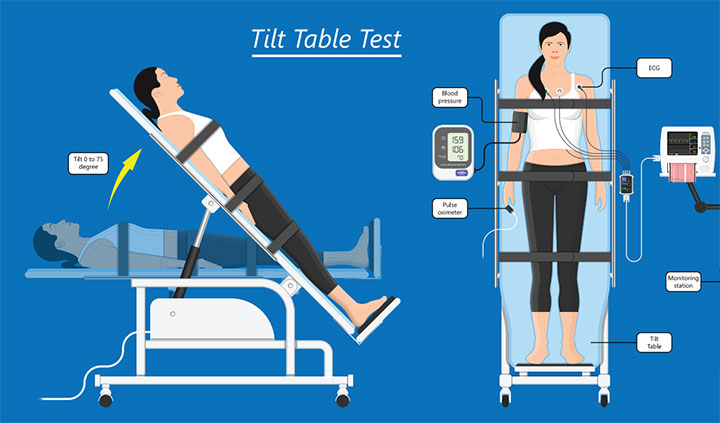
Results from a complete blood count, comprehensive metabolic panel, and thyroid profile are unremarkable. Ms. Watson undergoes an echocardiogram and electrocardiogram, which reveals no abnormalities or dysrhythmias. The provider orders a head-up tilt table test. The results include a rapid increase in heart rate and dizziness, suggesting that Ms. Watson suffers from POTS. The provider prescribes lifestyle changes and outpatient physical therapy to help control symptoms. After 6 months of treatment, Ms. Watson’s symptoms improve and she returns to work and caring for her family.
Pathophysiology
POTS is characterized by too little blood return to the heart when a person moves from a lying down or sitting position to a standing position (orthostatic intolerance). The person becomes lightheaded or dizzy and experiences a rapid increase in heart rate, which is reversed by sitting or lying down.
Normally, when a person moves from a sitting to a standing position, gravity pulls blood to the lower extremities. In response, blood vessels quickly narrow and the heart rate increases slightly to maintain normal blood flow to the heart and brain. All of these actions are a function of the autonomic nervous system. In POTS, this system doesn’t function properly (dysautonomia). The blood supplied to the heart and brain decreases with position change and blood remains in the lower extremities, which causes the body to compensate by dramatically increasing the HR.
Based on underlying causes, researchers have identified several POTS subtypes: neuropathic, hyperadrenergic, hypovolemic, autoimmunity, and excessive mast cell activation. (See POTS subtypes.)
POTS subtypes
Researchers have identified several postural orthostatic tachycardia syndrome (POTS) subtypes.
- Neuropathic POTS, the most common subtype, features disruption of the normal constriction of blood vessels in the lower extremities, which leads to stimulation of the sympathetic nervous system and a rapid increase in heart rate (HR). Causes include a traumatic injury, viral illness, or pregnancy.
- Hyperadrenergic POTS is believed to be an impairment in the body’s ability to reuptake norepinephrine (a neurotransmitter released in the bloodstream to increase HR and blood pressure [BP] as part of the automatic nervous system), which leads to overstimulation of the sympathetic nervous system. Symptoms include palpitations, tachycardia, tremors, and anxiety.
- Hypovolemic POTS is associated with a disruption of the renin-angiotensin-aldosterone system. This system helps regulate blood volume and BP. Up to 70% of patients with this subtype have reduced blood volume, which causes decreased venous return.
- Autoimmunity POTS has been suggested based on its association with onset after stress or viral illness in a patient with a personal or family history of systemic autoimmune disorders (such as Sjögren’s syndrome or lupus). Studies have found an increase in serum autoantibodies at receptor sites in patients with this subtype.
- Excessive mast cell activation POTS involves inappropriate release of histamine and other mast cell mediators in response to physical activity. Diagnosis is based on increased levels of histamine metabolites in the urine or elevated plasma tryptase levels.
Other possible causes of POTS have been related to vaccination, genetic predisposition, or from another disease process such as cancer, joint hypermobility, Lyme disease, or diabetes. Some patients may have overlapping subtypes and symptoms.
Symptoms
Most POTS symptoms stem from changes in blood flow and the body’s compensation for these changes. They include dizziness, syncope, tachycardia, blurred vision, headache, poor concentration or memory, fatigue, GI symptoms, shortness of breath, chest discomfort, urinary frequency, tremors, excessive sweating, and anxiety. In some people a reddish-blue discoloration of the legs occurs when they’re placed in a dependent position (lower than the heart). (See Signs and symptoms.)
Signs and symptoms
Signs and symptoms of postural orthostatic tachycardia syndrome include the following:
- Acrocyanotic (reddish-blue discoloration) legs
- Anxiety
- Bloating
- Blurred/tunnel vision
- Chest discomfort
- Diarrhea/constipation
- Dizziness
- Excessive sweating
- Exercise intolerance
- Fainting (syncope)
- Fatigue
- Flushing
- Headache/migraines
- Impaired memory (“brain fog”)
- Nausea
- Palpitations
- Poor sleep
- Shortness of breath
- Stomach pain/cramping
- Tachycardia (rapid heart rate)
- Tremors
- Urinary frequency
- Weakness
Risk factors
Although POTS can affect men and women of any age (up to 3 million Americans a year), it’s most common in women between the ages of 15 and 50. Episodes have been reported after major surgery, trauma, viral illness, or with other disease processes. Some people experience POTS after pregnancy, and symptoms may worsen right before menstruation. Although most cases of POTS occur in people with no family history of the condition, a small number of people report a family history of orthostatic intolerance. This finding suggests that genetics may play a role. Recently, Kanjwal and colleagues and Miglis and colleagues reported some cases of POTS that appear to be linked to those who’ve recovered from COVID-19.
Diagnostic studies
Diagnosing POTS presents challenges because symptoms affect a wide range of body systems and may mimic other conditions, such as chronic fatigue syndrome, fibromyalgia, Ehlers-Danlos syndrome, vasovagal syncope, anxiety, panic disorder, or inflammatory bowel disease. Many patients wait months or even years before they’re diagnosed with POTS. Delays in diagnosis may stem from the various symptoms, no definitive diagnostic test, and limited understanding of the disease process. In a study by Flack and Fulton, nearly half of patients waited more than 4 years before receiving a diagnosis.
Typically, the healthcare provider performs a physical assessment and health history, orthostatic BP measurements, blood tests (to rule out other disease processes), and a head-up tilt table test. Blood tests may include a complete blood count, comprehensive metabolic panel, thyroid profile, liver function test, and catecholamine levels. A 24-hour urine test also may be ordered to measure for catecholamines and urine sodium levels.
A 24-hour Holter monitor or echocardiogram may be ordered to rule out cardiac dysrhythmias or structural heart disease. Some providers may order a Valsalva maneuver test or quantitative sudomotor axon reflex test to assess autonomic function or magnetic resonance imaging to rule out a tumor or other abnormalities.
POTS may be suspected if all of the following criteria are met when performing the head-up tilt table test:
- Abnormal increase in HR when changing to an upright position (≥30 bpm within 10 minutes)
- Symptoms (lightheadedness, dizziness, palpitations) worsen when moved to an upright position
- No orthostatic hypotension in the first 3 minutes (defined as BP decreases ≥20/10 mmHg)
Before making the final diagnosis based on results of the head-up tilt table test, the provider must rule out other possible causes of orthostatic hypotension (such as medications) and ensure the patient has no acute dehydration or blood loss. POTS diagnosis also should be considered if orthostatic intolerance symptoms last more than 6 months and when symptoms improve after returning to a recumbent position.
Treatment
Because of the condition’s various causes and symptoms, no single POTS treatment option exists. Management aims to improve blood volume, decrease symptoms, and correct any underlying heart or blood vessel issues. Most patients can be managed with lifestyle changes or medications.
Nonpharmacologic management
Treatment should begin with lifestyle changes. Adding extra salt to the diet and increasing fluid intake can help increase blood volume. In addition, wearing elastic compression stockings that extend to the waist can help prevent venous pooling of blood, which may decrease symptoms. Instruct patients to sleep in an upright position and to rise slowly from a lying to a standing position. Also, teach patients to return to a reclined position if they became lightheaded or feel faint. Promote good sleep habits to help decrease fatigue, and encourage patients to avoid factors—such as stress, dehydration, prolonged standing, large meals, extreme heat, caffeine, and alcohol—that can worsen symptoms.
A regular, structured exercise program should focus on reconditioning and resistance training. According to Fu and Levine, patients with POTS who engage in exercise have fewer symptoms and overall improved well-being and quality of life. Those with moderate-to-severe symptoms should begin with non-upright exercises (such as rowing machines, recumbent bikes, or swimming) to reduce stress on the heart. They can then gradually increase activity based on their tolerance.
In addition, using counter-pressure maneuvers—squeezing a rubber ball, crossing the legs, tensing the arms, and contracting leg muscles—can help increase BP and reduce dizziness. Frequent rest breaks and gradually increasing activity will prevent extreme fatigue.
Pharmacologic management
Currently, no Food and Drug Administration–approved POTS treatments exist. However, depending on the subtype and symptoms, some medications may be beneficial. Fludrocortisone, a mineralocorticoid, has been used as first-line therapy for some patients. It promotes sodium retention by the kidneys, which helps retain fluid to expand blood volume and improve BP. Desmopressin, a natural antidiuretic, reduces tachycardia and increases fluid retention in some people. Midodrine, an alpha-adrenergic agonist, causes blood vessels to constrict, which decreases reflex tachycardia and increases BP.
Octreotide, a somatostatin analog, may help maintain venous return by causing vasoconstriction of the splanchnic circulation. For some patients, a nonselective beta blocker (such as propranolol) may block the sympathetic nervous system response and lower HR. However, side effects of beta blockers can lead to increased fatigue and dizziness in patients with POTS. Other patients may experience improved muscle strength with pyridostigmine, a cholinesterase inhibitor, which slows the breakdown of acetylcholine at nerve endings so that more is available at muscle receptors.
Some patients benefit from selective serotonin reuptake inhibitors. These medications can enhance nerve communication and stimulate the standing vasoconstriction reflex, which may reduce blood pooling and improve orthostatic tolerance.
Prognosis
Prognosis for patients with POTS varies. Those with mild symptoms may require only a few lifestyle changes to ensure undisrupted lives, whereas patients with moderate-to-severe symptoms may be unable to work or perform activities of daily living without assistance. Some patients report significant improvement within a year with or without treatment, but for others their symptoms worsen over time.
Several organizations and support groups (such as the Dysautonomia Support Network dysautonomiasupport.org) work to help patients and their families connect with others who have POTS. Many of these organizations have medical advisors or provide lists of doctors and clinics.
The sooner the better
Many causes and underlying conditions, including COVID-19, can lead to POTS. Early diagnosis, treatment, education, and support can help people living with the condition improve their quality of life.
Annette Ferguson is an associate professor and director of the undergraduate prelicensure BSN program at Marshall University in Huntington, West Virginia.
References:
Bryarly M, Phillips LT, Fu Q, Vernino S, Levine BD. Postural orthostatic tachycardia syndrome: JACC focus seminar. J Am Coll Cardiol. 2019;73(10):1207-28. doi:10.1016/j.jacc.2018.11.059
Dahan S, Tomljenovic L, Shoenfeld Y. Postural orthostatic tachycardia syndrome (POTS)—A novel member of the autoimmune family. Lupus. 2016;25(4):339-42. doi:10.1177/0961203316629558
Flack T, Fulton J. Quality of life in postural orthostatic tachycardia syndrome (PoTS): Before and after treatment. Br J Cardiol. 2018;25:140-2. doi:10.5837/bjc.2018.031
Fu Q, Levine BD. Exercise and non-pharmacological treatments of POTS. Auton Neurosci. 2018;215:20-7. doi:10.1016/j.autneu.2018.07.001
Ganesh R, Bonnes SLR, DiBaise JK. Postural tachycardia syndrome: Nutrition implications. Nutr Clin Pract. 2020;35(5):818-25. doi:10.1002/ncp.10564
Heyer GL. Postural tachycardia syndrome: Diagnosis and management in adolescents and young adults. Pediatr Ann. 2017;46(4):e145-54. doi:10.3928/19382359-20170322-01
John Hopkins Medicine. Postural orthostatic tachycardia syndrome (POTS).
Kanjwal K, Jamal S, Kichloo A, Grubb BP. New-onset postural orthostatic tachycardia syndrome following coronavirus disease 2019 infection. J Innov Card Rhythm Manag. 2020;11(11): 4302-4. doi:10.19102/icrm.2020.111102
Miglis MH, Prieto T, Shaik R, Muppidi S, Sinn D-I, Jaradeh S. A case report of postural tachycardia syndrome after COVID-19. Clin Auton Res. 2020;30(5):449-51. doi:10.1007/s10286-020-00727-9
Olshansky B, Cannom D, Fedorowski A, et al. Postural orthostatic tachycardia syndrome (POTS): A critical assessment. Prog Cardiovasc Dis. 2020;63(3):263-70. doi:10.1016/j.pcad.2020.03.010
Zadourian A, Doherty TA, Swiatkiewicz I, Taub PR. Postural orthostatic tachycardia syndrome: Prevalence, pathophysiology, and management. Drugs. 2018;78(10):983-94. doi:10.1007/s40265-018-0931-5

















2 Comments.
Thank you so much for this article. I was diagnosed 18 years ago after 2.5 years of searching and provider hopping. Finally, a nurse, yes a nurse, realized my hypotension and heart rate were not normal. She was a certified MS specialty nurse and she and the neurologist she worked for had seen several cases of POTs. They got me the best care and I was able to start nursing college and receive my BSN because of them. It is so important for us to understand this disease/syndrome so we can be advocates for those out there still waiting for the diagnosis. Thank you again.
What did you do for treatment?