Embrace evidence-based tools to empower nurses.
- Early mobilization involves the early application and intensification of physical therapy within the first 2 to 5 days of a critical illness.
- As a result of the unknown duration of ECMO and the known consequences of prolonged immobilization, organizations should implement early mobilization protocols.
- Practical, evidence-based guidelines (including visual confirmation tools, documented mobility goals, continuous feedback, and education) can help nurses embrace mobilization of patients receiving ECMO therapy.
Answers to the top 10 ECMO questions
The Bedside Mobility Assessment Tool 2.0
Understanding end-tidal CO2 monitoring
Learning Objectives
- Explain extracorporeal membrane oxygenation (ECMO) therapy.
- Describe immobility relative to ECMO and post-intensive care syndrome.
- Identify barriers and enablers of mobilization in patients receiving ECMO therapy.
No relevant financial relationships were identified for any individuals with the ability to control
content of the activity.
Expiration: 2/1/27
Although physical and occupational therapists can provide insight into the degree to which a patient receiving ECMO therapy can be mobilized safely, continuous supervision from these professionals isn’t always feasible. With evidence-based practice and clinical practice guidelines, nursing leaders can encourage nurses to embrace mobilization using a visual confirmation tool, documented mobility goals, continuous feedback mechanisms, and education.
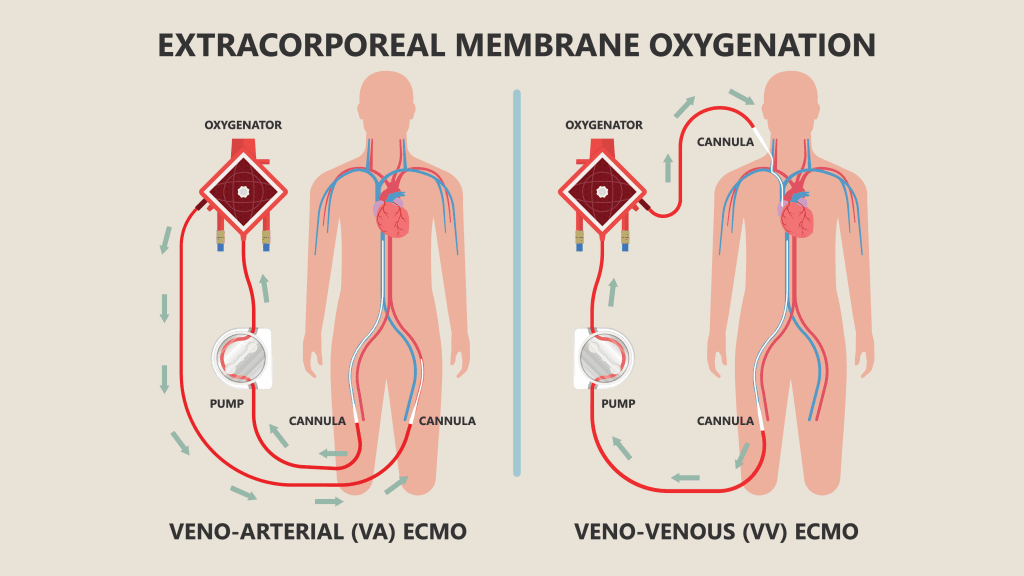
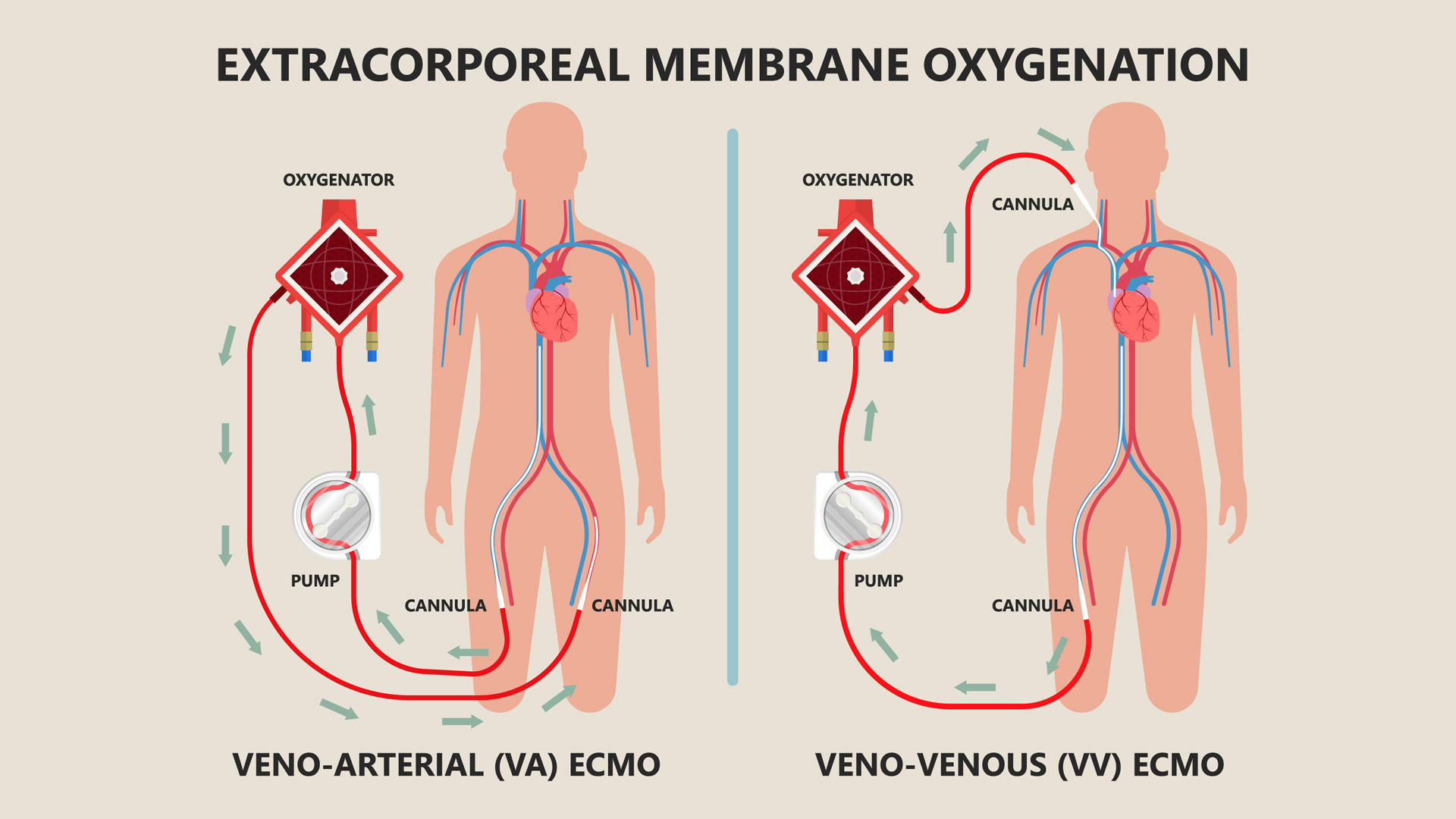
ECMO explained
The extracorporeal membrane oxygenation (ECMO) circuit contains four main components: drainage (access) cannula, blood pump, membrane oxygenator, and return cannula. Blood, which is drained through the access cannula under negative pressure, flows to a blood pump. The pump then pushes the blood through the membrane oxygenator under positive pressure and ultimately returns it to the patient through an artery or vein.
Oxygenator mechanics
The oxygenator, arguably the most important component of the ECMO circuit, has thousands of small hollow fibers filled with “sweep gas,” a mixture of medical air and oxygen; blood flows exterior to the fibers. The fibers allow for gas to diffuse through the membrane wall but prevent translocation of liquid so that blood and gas remain compartmentalized. By the principles of diffusion, oxygen and carbon dioxide diffuse between the gas and the blood as a direct function of the gas gradient, with partial pressure of a gas contributing to the transfer. Essentially, the oxygenator serves as the patient’s lung but with a smaller surface area for gas exchange, warranting higher blood flow rates to achieve optimal gas exchange.
Types of ECMO
- Venoarterial ECMO. The venoarterial (V-A) ECMO circuit provides artificial cardiac and pulmonary support. Patients who require V-A ECMO have cardiac dysfunction, with or without concomitant pulmonary dysfunction. During V-A support, the reperfused blood returning from the ECMO circuit mixes in the aorta with the left ventricular blood, which has previously passed through the lungs. Therefore, the oxygen content in the patient’s arterial blood represents a combination of blood from the patient’s native cardiopulmonary function and the ECMO circuit.
- Venovenous ECMO. Venovenous (V-V) ECMO differs from V-A ECMO in that the reperfused blood returns to venous circulation and mixes with venous blood draining from the systemic organs, resulting in higher oxygen content and decreasing the carbon dioxide content in the right atrial blood. The mixed blood passes through the right ventricle and lungs and then into systemic circulation.
The volume of blood removed is exactly proportionate to the volume of blood reinfused; therefore, no net effect occurs to central venous volume, right or left ventricle filling, or hemodynamics. Patients receiving V-V ECMO typically have isolated pulmonary dysfunction with mild to moderate right ventricular function. However, myocardial improvement may occur as the concomitant reduction in mechanical ventilator support allowed from improved gas exchange reduces right ventricular afterload and subsequently improves right ventricular function.
Early, progressive mobilization
Early mobilization involves the application and intensification of physical therapy within the first 2 to 5 days of a critical illness. However, many patients receiving ECMO require heavy levels of sedation for safety and comfort. Sedation also helps to reduce the incidence of vasovagal episodes, which impair the return cannula’s ability to provide richly oxygenated blood to the patient.
Sedation delays progressive early mobilization, which can contribute to long-term physical dysfunction and increased duration of mechanical ventilation. Research has demonstrated that critically ill adults who receive progressive mobilization have better clinical outcomes than those who receive usual care in the intensive care unit (ICU). Time from admission to implementation impacts the effectiveness of mobilization; early mobility is associated with improved patient and clinical outcomes.
The clinical problem
Resource limitations in nursing staff and physical, occupational, and respiratory therapist groups may lead to inconsistent application of mobilization for patients receiving ECMO therapy. Staffing shortages (as well as limited staff on evening and night shifts, weekends, and holidays) can impact mobility frequency and vigor. In addition, many nurses lack the knowledge to effectively apply appropriate activities without input from physical and occupational therapy services. They may not be aware of current evidence-based practice recommendations (including suggested frequency of mobilization), and they may believe that patients receiving ECMO therapy are “too sick” to be mobilized.
As the volume of patients receiving ECMO increases at many organizations with the addition of new extracorporeal life support programs, critical care teams must prioritize early progressive mobilization in the plan of care. However, nurses may feel hesitant to independently evaluate a patient for mobility readiness and subsequently initiate mobilization therapy.
The culture of immobility
Historically, suspended animation of critically ill patients occurred as a result of sedative agents administered during mechanical ventilation. As patient acuity increased, overriding a patient’s homeostatic processes became a widely accepted practice. With heavy sedation and intentional immobilization, complete control of patient derangements evolved to include normalization of aggressive vasoactive drip titration and I.V. volume replacement to optimize circulation and renal function while maintaining mechanical ventilation. To maintain a clinically docile patient, respiratory failure management began to include deep anesthesia and paralysis comparable to the operating room environment.
Research has disproven the theories supporting immobilization of critically ill patients. Rehabilitation specialists have challenged the existing culture with a new model that supports patient mobilization in high-acuity areas, although translation of this evidence into practice has been delayed.
Research also has demonstrated the importance of implementing the mobility component of the ICU Liberation Bundle to prevent patients from developing post-intensive care syndrome (PICS). The bundle, a set of clinical practice guidelines implemented along the critical care continuum, promotes sedation weaning, pain management optimization, delirium reduction, shortened mechanical ventilation duration, and family engagement. Ongoing care coordination and collaboration help interprofessional team members strategize to mitigate competing priorities and strategically implement all elements of the bundle. (See What is PICS?)
What is PICS?
Post-intensive care syndrome (PICS) may manifest as ICU acquired weakness (ICUAW) or cognitive dysfunction. According to the Society of Critical Care Medicine, ICUAW may occur in as many as 33% of patients on a ventilator and 50% of patients who have an ICU length of stay of a week or more. Patients with ICUAW may experience difficulty performing activities of daily living for at least a year, and 30% to 80% may experience cognitive dysfunction for at least a year. Some individuals may never return to their baseline. Cognitive dysfunction results in substantial impairments in performing daily tasks that involve concentration and organization, including balancing a checkbook or returning to work. To reduce the risk of developing PICS, providers may embrace recommendations for early, progressive mobilization.
ICUAW contributing factors and consequences
Contributing factors
- Inflammatory states
- Malnutrition
- Medications
- Neuromuscular blockades
- Steroids
- Muscle atrophy
- Muscle catabolism
Consequences
- Accelerated skeletal muscle atrophy
- Disturbance of peripheral nerves
- Higher hospital costs
- Increased delirium days
- Increased ICU and hospital lengths of stay
- Increased sedation levels
- Membrane inexcitability
- Neuromuscular weakness despite full supportive care
- Poor functional independence at time of discharge
- Prolonged mechanical ventilation
Sources: Brock et al., da Cunha Ferreira et al., Fraser et al., Hodgson et al. (2013), Jolley et al., Nydahl et al., Salna et al., van Dyk
Mobilization in the critical care setting
Mobility, a highly modifiable intervention, can be individualized for specific patient needs. In the ICU, it includes functional positioning, active and passive extremity range of motion, sitting, bedside standing, walking with support, and assisted exercise. Respiratory benefits of mobilization include postural drainage, clearance of airway secretions, and improved respiratory function and residual capacity. The cumulative benefits provide evidence to support augmenting mobilization with respiratory exercises. Other physiologic benefits of mobilization include stimulation of peripheral blood flow, production of anti-inflammatory cytokines, and increased uptake of glucose in muscle tissue.
Mobilization also decreases cumulative sedation administration. Excessive sedation contributes to increased delirium and delays mobilization implementation in the plan of care. The Society of Critical Care Medicine offers strong recommendations for sedation minimization strategies, daily sedation interruptions, nurse-driven sedation protocols, and intermittent sedation. Mobilization offers opportunities for sedation vacations, which can help decrease delirium days and improve activity participation.
Mobilization considerations
Current evidence supports mobilization of patients receiving ECMO therapy with careful consideration of patient- and circuit-specific factors to aid success, as well as potential risks and contraindications to mobilization. The most critical consideration involves the potential dislodgement or disconnection of cannulas during mobilization. Despite wire reinforcement within cannulas, activities involving hip flexion in patients with femoral cannulation or other cannula manipulation may result in kinks that interrupt blood flow. Shorter reinfusion cannulas pose the greatest risk for dislodgement.
Patients receiving ECMO therapy may experience worsening gas exchange or hemodynamics depending on mobilization vigor and their underlying concomitant organ dysfunction. Ultimately, all ECMO patients should be included in a mobilization protocol unless contraindications exist. Red-flag contraindications may prompt a pause in therapy to discuss the patient’s readiness with the provider, but they may not require a hard stop to mobilization.
Safe mobilization requires sufficient staff training and thorough patient assessment (including cardiovascular, respiratory, and neurologic status). Evaluation should include collaboration among the nurse, provider, and rehabilitation specialists. In addition, the nurse must understand what clinical events warrant immediate mobilization termination, including the development of new clinical instability or dislodgement of critical lines and medically necessary devices.
Relative contraindications to mobilization may include decreased level of consciousness, pain, fatigue, hypothermia or hyperthermia, increased mechanical ventilation requirements, changes in clinical assessment and hemodynamics, and increasing doses of inotropes or vasopressors. Patients with contraindications should undergo daily (or more frequent) reassessment to determine activity readiness. Patients not yet ready for high-level mobilization may be appropriate candidates for in-bed exercises or passive range of motion.
If a patient is receiving infusions of vasoactive medications or has femoral access devices, nurse consultation with the provider or physiotherapist to determine eligibility for mobilization is warranted. Conditions that may exclude a patient from mobilization include new or worsening bleeding, continuous infusion of paralytics, status postcardiotomy with an open sternum, status postcardiotomy with central ECMO cannulation, a drop in ECMO flows >1.0 L/min with movement, active seizures, hemodynamic instability, and uncontrolled GI bleeding. Generally, safe mobilization requires absence of the following clinical signs: new or symptomatic arrhythmias, unstable spinal injury, and increased intracranial pressure. The interprofessional team should regularly evaluate individual patient mobilization readiness.
Mobilization barriers
Reviews by Marhong and colleagues and Bakhru and colleagues suggest that structured mobility programs suffer from implementation lag due to ongoing conservative management of patients in the ICU, which parallels a culture of bed rest. The most common barriers to mobilization fall into the following four contextual categories: patient, clinician, organization, and ICU.
Patient-related barriers.
Patient-related barriers include diagnosis and illness severity, hemodynamic concerns, adverse response to treatment, physiologic patient issues, comorbidities, delirium, sedation level, and pain. Less-common barriers include patient inability to follow instructions and refusal to participate. For patients receiving ECMO, additional physiologic considerations include level of dependence on mechanical circulatory support, which can impact oxygen consumption and may lead to an increased need for ECMO during mobilization.
Clinician-related barriers.
Clinician-related barriers include the level of motivation to implement mobilization techniques and beliefs regarding the benefits and harm of mobility interventions. Clinicians may lack knowledge and awareness of mobility protocols, disagree with guidelines, lack self-efficacy and confidence in implementing protocols and procedures, resist change, worry about the safety of catheters and other tubes and wires, or believe that rest generates healing. In some cases, clinicians have workloads that limit their availability to oversee mobility therapy or leadership hasn’t successfully recruited unit staff buy-in. According to a cross-sectional survey study by Jolley and colleagues, concern regarding overall work stress and prolongation of the workday when usual care is delayed due to mobilization also contribute to immobility.
Organization-related barriers.
Organization-related barriers include lack of funding and access to mobilization services as well as limited availability of equipment, resources, and staffing. Other considerations include unclear protocol criteria, a need for clarity as to team member responsibility for mobilization initiatives, and lack of confidence in screening tools used to guide patient selection for mobility.
ICU-related barriers.
Barriers related to the ICU environment include poor unit culture; lack of interprofessional teamwork, expertise, and skill training; and the need for provider orders before initiating mobilization. Insufficient interprofessional communication, low prioritization among competing priorities, scheduling conflicts, disengaged team members, and staff turnover play significant roles in delayed or absent delivery of mobility treatments. Several studies show an association between RN-to-patient ratios and mobilization efficacy, as well as heavier patient workloads and unsatisfactory patient outcomes. Similarly, lack of dedicated nursing and physical therapy staff, especially on weekends and off-shifts, contributes to unsuccessful mobilization implementation.
Mobilization enablers
Research has identified several interventions as mobility enablers in the critical care setting. They include implementing daily goals, creating visual goal targets, using continuous feedback mechanisms to illustrate progress toward daily goals, and providing nurse education.
Nurse knowledge of daily patient goals plays a critical role in improving mobilization practices. When nurses understand these goals, they can anticipate the daily plan of care to avoid competing priorities. Visible goal targets (displayed tools that illustrate patient progress) can positively influence mobilization levels.
ICU nurses typically focus on acute needs (such as airway maintenance, breathing, and circulation), which provide immediate feedback. Mobility feedback, on the other hand, may be inconsistent, especially with regard to ambulation—one of the most frequently missed types of nursing care. A unit can achieve continuous mobility feedback with the use of a visual confirmation tool.
Perceptions of mobilization
Nurses describe differing mobilization practices based on experience levels; senior staff tend to be more proactive in mobilizing critically ill patients. Reluctance of novice nurses to perform mobilization may be related to a cumulative lack of knowledge and confidence and the sense of feeling burdened by the critical care environment and competing priorities. Nurses describe wanting more support from physical therapy, increased interprofessional communication, and mobilization education. Overall, the literature doesn’t clearly define the nurses’ role in mobilization and how nurses assist with identifying appropriate patients. Ultimately, the team role of mobility necessitates participation from interprofessional staff.
Implications for nursing practice
Translating evidence into current practice will improve both the quality and frequency of mobility therapy for adult patients receiving ECMO therapy who have a low threshold for developing immobility complications. Critical care settings require prompt implementation of nurse-led mobility interventions and recruitment of staff buy-in to make early progressive mobilization a widely accepted standard of care.
Engaging the nursing team and promoting enthusiam for mobility require consistent daily rounding with intentional conversations among team members regarding specific daily mobility goals, reinforcement of an interprofessional approach to mobility, and mobility implementation monitoring during times of increased census. Interprofessional discussion of daily mobility goals is critical, even when planning low-level mobility interventions. Adopting an evidence-based tool, such as the Johns Hopkins Highest Level of Mobility Score, can aid mobility goal discussion and promote consistent and uniform quantification of mobilization across various disciplines. A dedicated mobility champion can help ensure observation of these practices and implementation of new protocols. (See Johns Hopkins score.)
Johns Hopkins score
The Johns Hopkins Highest Level of Mobility (JH-HLM) Score serves as a standard language when interprofessional stakeholders discuss and categorize mobilization activities. The tool, which has been used in ICUs and progressive care units for over 5 years, aids increasing patient mobility in hospital settings.
The JH-HLM score (determined using the Johns Hopkins Mobility Goal Calculator) has eight levels of mobility, with higher levels representing greater mobility achievement.

Mobility champion
Consistent rounding by a mobility champion may increase the likelihood of frequent, intensive mobilization practices implemented in high-risk patients in the ICU. The nurse in this role may oversee various evidence-based initiatives for improving mobilization and modify interventions to ensure workflow appropriateness for their individual organization. For example, strategies for improving mobilization frequency may include deploying explicit safety screens, conducting interprofessional rounds wth a focus on mobility, and providing positive reinforcement for early mobility practices. In addition, writing a thorough mobility protocol may help improve education and targeted goal planning with the primary objective of early mobilization.
Role models
The mobility champion serves as an effective role model for the ideal state of clinical practice and should be prepared to train additional unit-based champions to oversee and encourage mobility practices on all shifts. Role modeling from seasoned nurses also can help increase new nurse participation in mobility protocols and initiatives.
Broadcast patient success
Witnessing patient success, which demonstrates the validity and importance of a practice in real time, can serve as a team motivator. When rounding and speaking to nurses, a mobility champion may inquire about patient triumphs and accomplishments, including length of time spent performing vertical bed therapy or the number of times passive range of motion was implemented. The champion can publicize these examples via bulletin boards, emails, and team huddles to motivate and inspire. Some patients may want to visit the ICU after discharge and offer a testimony to the importance of mobilization and the positive impact it had on their mental and physical health. These patient successes (especially if observed by other patients) serve as motivation.
Empowered to improve care
Although progressive mobilization of patients receiving ECMO is clinically proven to drive positive patient outcomes, implementation lag and resistance to change continue to create barriers. Nurses should feel empowered to change the trajectory of care for patients receiving ECMO therapy by applying various strategies to enable mobilization, including mobility protocols, site-specific screening guidelines, visible goal targets, documented mobility goals, continuous feedback mechanisms, and nurse education.
Rachael Alexis Jividen is the Cleveland Clinic Health System ECMO coordinator and an acute care clinical nurse specialist at the Cleveland Clinic Main Campus in Cleveland, Ohio.
American Nurse Journal. 2024; 19(2). Doi: 10.51256/ANJ022406
References
Agency for Healthcare Research and Quality. Nurse-driven early mobility protocols: Facilitator guide. January 2017. www.ahrq.gov/hai/tools/mvp/modules/technical/nurse-early-mobility-protocols-fac-guide.html
Anekwe DE, Kin-Yue Koo K, de Marchie M, Goldberg P, Jayaraman D, Spahija J. Interprofessional survey of perceived barriers and facilitators to early mobilization of critically ill patients in Montreal, Canada. J Intensive Care Med. 2019;34(3):218-26. doi:10.1177/0885066617696846
Bakhru RN, McWilliams DJ, Wiebe DJ, Spuhler VJ, Schweickert WD. Intensive care unit structure variation and implications for early mobilization practices. An international survey. Ann Am Thorac Soc. 2016;13(9)1527-37. doi:10.1513/AnnalsATS.201601-078OC
Barber EA, Everard T, Holland AE, Tipping C, Bradley SJ, Hodgson CL. Barriers and facilitators to early mobilisation in intensive care: A qualitative study. Aust Crit Care. 2015; 28(4):177-82. doi:10.1016/j.aucc.2014.11.001
Bartlett RH, Conrad SA. The physiology of extracorporeal life support. In: Lequire L, Lorusso R, MacLaren G, Peek G, eds. Extracorporeal Life Support: The ELSO Red Book. 5th ed. Ann Arbor, MI: Extracorporeal Life Support Organization; 31-47.
Brock C, Marzano V, Green, M, et al. Defining new barriers to mobilisation in a highly active intensive care unit—Have we found the ceiling? An observational study. Heart Lung. 2018;47(4):380-5. doi:10.1016/j.hrtlng.2018.04.004
Costa DK, White MR, Ginier E, et al. Identifying barriers to delivering the awakening and breathing coordination, delirium, and early exercise/mobility bundle to minimize adverse outcomes for mechanically ventilated patients: A systematic review. Chest. 2017;152(2):304-11. doi:10.1016/j.chest.2017.03.054
da Cunha Ferreira D, Marcolino MAZ, Macagnan FE, Della Méa Plentz R, Kessler A. Safety and potential benefits of physical therapy in adult patients on extracorporeal membrane oxygenation support: A systematic review. Rev Bras Ter Intensiva. 2019;31(2)227-39. doi:10.5935/0103-507X.20190017
Davidson JE, Hopkins RO, Louis D, Iwashyna TJ. Post-intensive care syndrome. Society of Critical Care Medicine. 2013. bit.ly/3tij58s
Desai SV, Law TJ, Needham DM. Long-term complications of critical care. Crit Care Med. 2011;39(2):371-9. doi:10.1097/CCM.0b013e3181fd66e5
Devlin JW, Skrobik Y, Gélinas C, et al. Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. 2018;46(9):e825-73. doi:10.1097/CCM.0000000000003299
Engel HJ, Needham DM, Morris PE, Gropper MA. ICU early mobilization: From recommendation to implementation at three medical centers. Crit Care Med. 2013;41(9 suppl 1):S69-80. doi:10.1097/CCM.0b013e3182a240d5
Fraser D, Spiva L, Forman W, Hallen C. Original research: Implementation of an early mobility program in an ICU. Am J Nurs. 2015;115(12):49-58. doi:10.1097/01.NAJ.0000475292.27985.fc
Hickmann CE, Castanares-Zapatero D, Deldicque L, et al. Impact of very early physical therapy during septic shock on skeletal muscle: A randomized controlled trial. Crit Care Med. 2018;46(9):1436-43. doi:10.1097/CCM.0000000000003263
Hiser S, Chung CR, Toonstra A, et al. Inter-rater reliability of the Johns Hopkins Highest Level of Mobility Scale (JH-HLM) in the intensive care unit. Braz J Phys Ther. 2021;
25(3):352-5. doi:10.1016/j.bjpt.2020.07.010
Hodgson CL, Berney S, Harrold M, Saxena M, Bellomo R. Clinical review: Early patient mobilization in the ICU. Crit Care. 2013;17(1):207. doi:10.1186/cc11820
Hodgson CL, Capell E, Tipping CJ. Early mobilization of patients in intensive care: Organization, communication and safety factors that influence translation into clinical practice. Crit Care. 2018;22(1):77. doi:10.1186/s13054-018-1998-9
Hoyer EH, Young DL, Klein LM, et al. Toward a common language for measuring patient mobility in the hospital: Reliability and construct validity of interprofessional mobility measures. Phys Ther. 2018;98(2):133-42. doi:10.1093/ptj/pzx110
Hsieh SJ, Otusanya O, Gershengorn HB, et al. Staged implementation of awakening and breathing, coordination, delirium monitoring and management, and early mobilization bundle improves patient outcomes and reduces hospital costs. Crit Care Med. 2019;47(7):885-93. doi:10.1097/CCM.0000000000003765
Johns Hopkins Medicine. Activity and mobility promotion (JH-AMP). hopkinsAMP.org
Jolley SE, Regan-Baggs J, Dickson RP, Hough CL. Medical intensive care unit clinician attitudes and perceived barriers towards early mobilization of critically ill patients: A cross-sectional survey study. BMC Anesthesiol. 2014;14:84. doi:10.1186/1471-2253-14-84
Kanejima Y, Shimogai T, Kitamura M, Ishihara K, Izawa KP. Effect of early mobilization on physical function in patients after cardiac surgery: A systematic review and meta-analysis. Int J Environ Res Public Health. 2020;17(19):7091. doi:10.3390/ijerph17197091
Krupp A, Steege L, King B. A systematic review evaluating the role of nurses and processes for delivering early mobility interventions in the intensive care unit. Intensive Crit Care Nurs. 2018;47:30-8. doi:10.1016/j.iccn.2018.04.003
Nydahl P, Sricharoenchai T, Chandra S, et al. Safety of patient mobilization and rehabilitation in the intensive care unit.
Systematic review with meta-analysis. Ann Am Thorac Soc. 2017;14(5):766-77. doi:10.1513/AnnalsATS.201611-843SR
Marhong JD, DeBacker J, Viau-Lapointe J, et al. Sedation and mobilization during venovenous extracorporeal membrane oxygenation for acute respiratory failure: An international study. Crit Care Med. 2017;45(11):1893-99. doi:10.1097/CCM.0000000000002702
Parry SM, Knight LD, Connolly B, et al. Factors influencing physical activity and rehabilitation in survivors of critical illness: A systematic review of quantitative and qualitative studies. Intensive Care Med. 2017;43(4):531-42. doi:10.1007/s00134-017-4685-4
Salna M, Abrams D, Brodie D. Physical rehabilitation in the awake patient receiving extracorporeal circulatory or gas exchange support. Ann Transl Med. 2020;8(13):834. doi:10.21037/atm.2020.03.15
Schweickert WD, Kress JP. Implementing early mobilization interventions in mechanically ventilated patients in the ICU. Chest. 2011;140(6):1612-7. doi:10.1378/chest.10-2829
Society of Critical Care Medicine. ICU liberation bundle (A-F). sccm.org/Clinical-Resources/ICULiberation-Home/ABCDEF-Bundles
Sommers J, Engelbert RHH, Dettling-Ihnenfeldt D, et al. Physiotherapy in the intensive care unit: An evidence-based, expert driven, practical statement and rehabilitation recommendations. Clin Rehabil. 2015;29(11):1051-63. doi:10.1177/0269215514567156
van Dyk M. Physiotherapy for ECMO patients. Egypt J Crit Care Med. 2018;6(3):147-9. doi:10.1016/j.ejccm.2018.12.013
Wells CL, Forrester J, Vogel J, Rector R, Tabatabai A, Herr D. Safety and feasibility of early physical therapy for patients on extracorporeal membrane oxygenator: University of Maryland Medical Center Experience. Crit Care Med. 2018;46(1):53-9. doi:10.1097/CCM.0000000000002770
Key words: extracorporeal membrane oxygenation, ECMO therapy, patient mobilization