
Advancing patient mobility.
- Complications of immobility lead to patient harm including cardiovascular, respiratory and musculoskeletal deterioration.
- The Bedside Mobility Assessment Tool 2.0 (BMAT 2.0) addresses immobility using a simple functional assessment and selection of appropriate equipment to safely mobilize the patient.
- BMAT 2.0 aligns with the American Nurses Association (ANA) “Safe Patient Handling and Mobility: Interprofessional National Standards, Across the Continuum of Care,” Standard 6, focused on “initial and ongoing assessment or process to determine SPHM needs.”
Immobility compromises almost every system in the body. Studies show that adults who were ambulatory before hospital admission spend up to 83% of their time lying down while in the hospital, and more than a third of hospitalized adults 70 years and older are discharged with a major new disability that wasn’t present on admission.
Mobilizing patients safely and consistently is challenging. Accurately assessing mobility status allows healthcare providers to monitor improvements and deterioration and apply interventions to mobilize patients, even when deficits are present. The result can be progress toward physical independence; at a minimum, it maintains patients’ strength and decreases risks associated with bedrest.
The VIP treatment: A comprehensive post-fall assessment guideline
Preventing falls in hospitalized patients
This article introduces the Bedside Mobility Assessment Tool 2.0 (BMAT 2.0), revised from BMAT 1.0, which was created to identify patient mobility function deficits and guide the healthcare team in selecting equipment to safely handle and mobilize patients. BMAT 2.0 is most effective when documented in the electronic health record (EHR) and clearly communicated with all staff.
BMAT aligns with the American Nurses Association’s (ANA’s) Safe Patient Handling and Mobility: Interprofessional National Standards Across the Care Continuum by promoting mobilization techniques. The tool promotes healthcare worker safety and early and frequent mobilization, which improves patient safety.
BMAT origin
In 2003, Boynton (lead author of this article) saw the need for a mobility assessment tool and began searching for one nurses could use to determine patients’ current mobility status and would help standardize safe patient handling and mobility (SPHM) equipment (especially patient lifts) use. Development included networking with nurses from different hospitals and piloting the tool to assess its feasibility and utility.
Validation
In 2012-2013, BMAT 1.0 was validated for content and construct, and for inter-rater reliability by a healthcare team at Banner Baywood Medical Center in Mesa, AZ. The tool was created in the Banner Health system EHR and linked to the fall risk assessment (Morse Fall Scale) on the Adult Mobility and Fall Risk Assessment screen and to the skin assessment (Braden Scale).
Nurses who completed an early BMAT 1.0 pilot study on a 60-bed medical telemetry unit found that the tool took the guesswork out of determining a patient’s mobility status and choosing SPHM equipment. Findings included decreased nurse injuries and patient falls. Nurses reported increased awareness of changes in patients’ status during a shift and improved confidence using SPHM lifts and getting patients out of bed more frequently because they no longer relied on physical and occupational therapists.
BMAT 1.0 has been implemented at many hospitals throughout the United States and internationally. Nursing implications include timely referrals to rehabilitation services; improved communication among nurses, aides, physical and occupational therapists, and ancillary services (radiologists, transporters) regarding SPHM practices and safe patient transfer methods; and better implementation of ANA SPHM Standard 6 (integrate patient-centered SPHM assessment, plan of care, and use of SPHM technology).
BMAT 2.0
BMAT 2.0 incorporates new knowledge developed over 5 years of BMAT 1.0 use. It clarifies how to perform assessments and determine pass or fail; the nurse’s role in assessing, strengthening, and progressing patients; progression from Level 3 to Level 4; and the use of walkers, canes, crutches, and prosthetic legs and progressing patients who use these aids. BMAT 2.0 also addresses bilateral nonweight-bearing patients and bed rest orders and focuses on previous level of function (PLOF), discharge planning, and goals for ambulating patients who pass all four assessments.
BMAT 2.0, which takes about 2 minutes to complete, typically is performed by nurses on patient admission, once per shift, and with any significant change in a patient’s status. It empowers caregivers to ACT:
- Assess for mobility level in “safe mode.”
- Coordinate strategies for strengthening.
- Target the right piece of equipment to advance mobility.
The tool defines four levels of mobility. Each level has a physical task aimed at assessing a patient’s strength, coordination, balance, tolerance, and ability to follow directions. When patients can perform the task, they advance to the next level; if they can’t, they stay at the current level. If the patient is responsive, the assessment can be completed as part of routine physical and cognitive screenings. (Download the full BMAT 2.0 here.)
Level 1 assessment
Level 1 evaluates core strength, sitting tolerance, balance, and hemodynamic stability in response to sitting upright.
Sit and shake: Ask the patient to pivot from a semireclined position (head of bed ≥ 30 degrees) to the edge of the bed and maintain an unsupported seated balance for up to 1 minute (to allow fluid shifts and other compensatory changes to occur). Then ask the patient to reach across the midline with one hand and shake your hand; have the patient repeat with the other hand.
Assess: Can the patient maneuver to an upright seated position and maintain unsupported seated balance while reaching across the midline?
- Unsupported sitting engages core muscles and back extensors.
- Sitting upright assists with fluid shifts (with bedrest, about 1 L of fluid moves from the legs to the chest).
- Sitting upright aids ribcage expansion and breathing.
Patients who sit without getting tachycardic, diaphoretic, or light-headed, and can reach across and shake your hand can proceed to Level 2 assessment.
Note: Patients who are nonresponsive or have a strict bedrest order are automatically Level 1 and should be mobilized following progressive mobility protocols. A provider’s “strict bedrest” or “bedrest” order may require clarification if the order is inconsistent with nursing responsibility expectations. Patient mobilization is within the scope of nursing practice, and nurses are expected to evaluate patients’ needs and advance mobility to avoid immobility risks and complications.
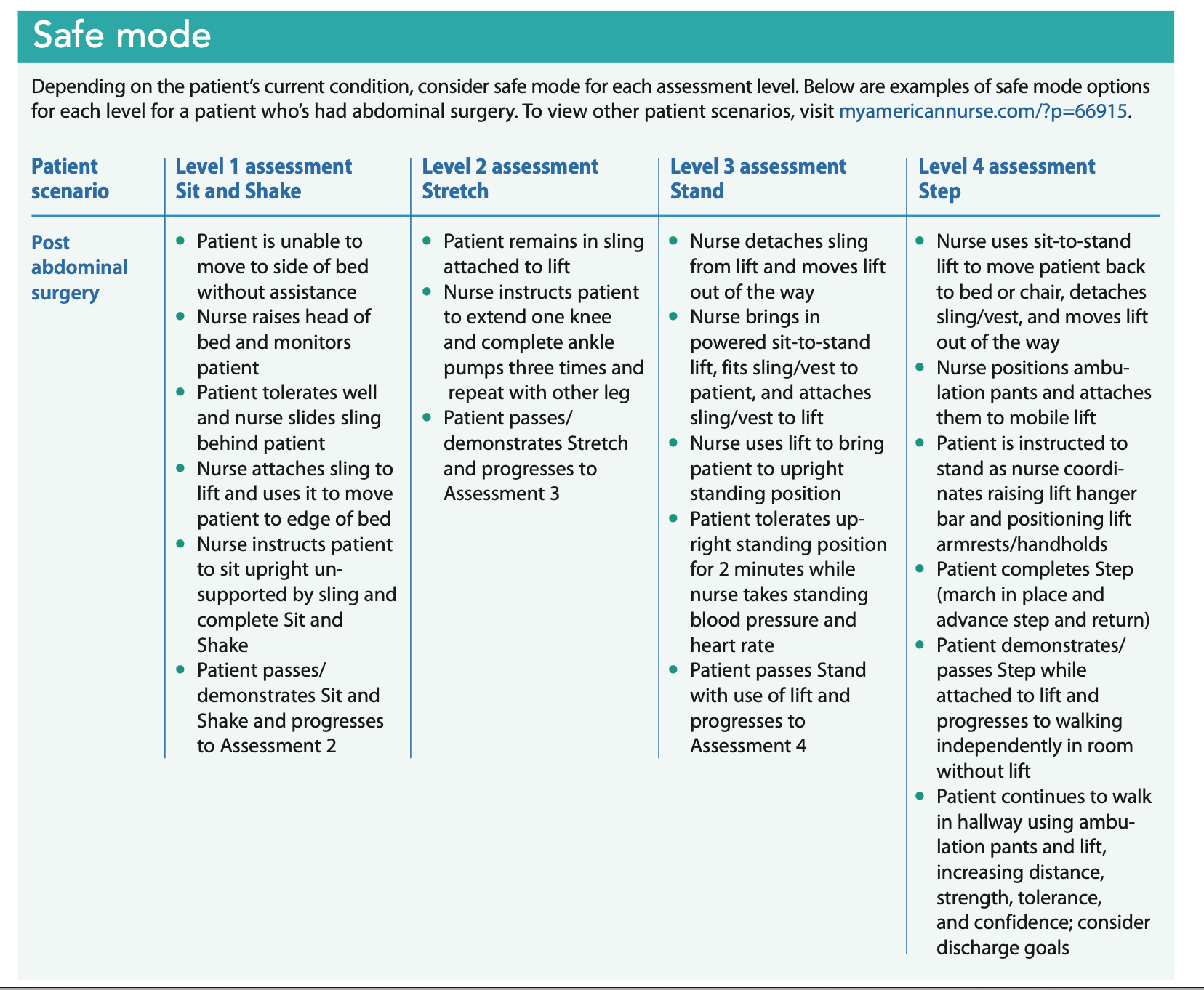
Safe mode: Consider safe mode for patients who can’t perform Sit and Shake (for example, a patient with a large abdominal incision), for patients you’re not sure can independently maneuver to a seated position at the edge of bed and sit unsupported, and for patients who may slide off the bed. (See Safe mode.)
How do I mobilize and progress patients who can’t perform Sit and Shake?
Level 1 patients require appropriate SPHM equipment for tasks such as repositioning/boosting, turning, limb holding, and bed-to-chair transfers. Consider calf pump exercises to help progress these patients, prepare them for the Level 2 assessment, assist with circulation, and prevent contractures.
Level 2 assessment
Level 2 evaluates a patient’s ability to engage leg and foot muscles. It assesses leg strength and foot-drop contracture deformity and is a precursor to weight-bearing.
Stretch: While the patient is sitting upright and unsupported on the side of the bed or in a chair, instruct the patient to extend one leg, straighten the knee (knee remains below hip level), pump the ankle (dorsiflexion/plantar flexion) at least three times, and repeat with the other leg and ankle.
Assess: Can the patient straighten the knees and pump the ankles?
- This maneuver evaluates patient control and leg muscle (quadriceps and calf muscles) strength.
- Pumping the ankles engages the calf muscles, which assists with venous blood return (leg muscles, especially calf muscles when they contract, play an important role in compressing major leg veins and ensuring adequate blood return to the heart). When done before the patient stands, calf pump exercises can decrease the risk of orthostatic hypotension and falls.
- Achilles tendon shortening is one of the most common contractures that occurs with bedrest. Pumping the ankle assesses for this contracture and ability to move the ankles.
- Extensor muscles (for example, quadriceps, which have a primary postural role) are one of the first groups of muscles compromised by bedrest. These muscles are necessary for both standing and walking. Patients who can’t perform Stretch won’t be able to safely stand or walk. Assessing can prevent a possible fall.
Patients who sit without getting tachycardic, diaphoretic, or light-headed, and can extend their leg/straighten their knee and pump their ankle three times (one leg/ankle and then the other) can proceed to Level 3 assessment.
Safe mode: Consider performing Stretch with the bed in chair position or by supporting the patient in a walking/ambulation vest or pants and a lift at the edge of the bed.
How do I mobilize and progress patients who can’t perform Stretch?
Level 2 patients typically require the same type of SPHM equipment as Level 1 patients; however, because they have adequate seated balance, Level 2 patients can participate to a greater extent than Level 1 patients. When working to progress Level 2 patients, a powered sit-to-stand lift, which allows the patient to safely assume an upright position and bear weight through one or both legs, may be appropriate. Other leg-strengthening exercises can be incorporated into the patient’s care plan, along with increased calf pump exercise repetition.
Level 3 assessment
Level 3 evaluates the patient’s ability to stand, tolerate standing, and maintain standing balance, which are precursors to ambulation.
Stand: While the patient is sitting upright unsupported on the side of the bed or in a chair, with feet positioned about shoulder-width apart, instruct the patient to move from a seated position to standing upright. Patients should shift their weight forward while raising the buttocks from the surface and rising.
Assess: Can the patient shift forward, rise, and maintain standing balance for up to 1 minute?
- Stand evaluates the patient’s leg muscle control, dynamic balance, and strength to rise.
- Standing upright for up to 1 minute allows fluid to shift and other compensatory changes to occur. Most patients who exhibit orthostatic hypotension do so in the first minute of standing, which is the rationale for standing for up to 1 minute for this assessment.
- Guide patients who become light-headed or can’t tolerate standing to sit down.
Patients who can stand without becoming tachycardic, diaphoretic, or light-headed, and who have the cognitive ability to stand can proceed to Level 4 assessment.
Safe mode: To assess Stand in safe mode and progress the patient, consider using a sit-to-stand lift to determine how the patient tolerates moving from sitting to standing and weight-bearing.
- If the patient tolerates standing with the use of a sit-to-stand lift, consider repeating Level 3 assessment without the lift or consider further strengthening exercises and referral to physical therapy (PT).
- Consider use of the patient’s walker, cane, crutches, or prosthetic leg(s) consistent with best practice and safe use guidelines during the standing assessment.
How do I mobilize and progress patients who can’t perform Stand?
Level 3 patients may require the same type of SPHM equipment as Level 2 patients for tasks such as quick transfers from bed to toilet. Consistent with best practice guidelines, use the patient’s walker, cane, crutches, and prosthetic leg(s) to complete stand. If the patient passes Stand, continue to Level 4 Assessment using aides as needed.
Level 4 assessment
Level 4 evaluates the patient’s ability to step in two parts: march in place and advance step and return with one foot then the other. This is a precursor to ambulation.
Step: While the patient is standing at the side of the bed or by a chair, ask the patient to march in place using small steps (not lifting knees up high) for three repetitions. If the patient successfully completes marching in place, ask the patient to step forward with the right foot then return to the starting position; repeat with the left foot.
Assess: Can the patient shift weight from one foot to the other and maintain balance side-to-side and forward and back?
- Step assesses patient leg muscle control and dynamic balance.
- Step allows fluid to shift and other compensatory changes to occur.
- Guide patients who become light-headed or can’t tolerate the Step maneuvers to sit.
- Patients who can pass marching in place but can’t perform advance step and return with one or both feet should be guided to sit; request a PT consult. To avoid potential falls, keep the patient close to the bed or chair; patients shouldn’t independently leave the side of the bed or chair until they demonstrate the ability to back up.
Patients who can Step without becoming tachycardic, diaphoretic, or light-headed, and who have the cognitive ability to Step can proceed to activities to improve endurance and ambulation confidence.
Safe mode: To assess Step in safe mode and progress the patient, consider positioning the bed in chair position and use end-of-bed egress after fitting the patient with a walking vest or pants with a mobile lift. Another option is having the patient sit at the side of the bed and using a walking/ambulation vest or pants and ceiling lift. Using either technique, instruct the patient to complete Step.
How do I mobilize and progress patients who can’t perform Step?
Level 4 patients may require the same type of SPHM equipment (for example, a stand aid) as those used with Level 3 patients for tasks such as quick transfers from bed to toilet during the night. Following good practice guidelines, initially complete Step in safe mode using a walking/ambulation vest or pants and a lift; consistent with best practice, use the patient’s walker, cane, crutches, or prosthetic leg(s) to complete the maneuver.
Patients who perform and pass both portions of Step, with or without an aid, can progress through discharge planning.
How do I mobilize and progress patients who have passed all four assessment levels?
To meet discharge goals, patients who have passed all four assessment levels may still need to use a lift with a walking/ambulation vest or pants to increase endurance and distance walked and to reduce fall risk. In addition:
- Continue to address medical issues and stability as needed while improving or maintaining mobility; evaluate other medical conditions and treatment plans before discharge.
- Coordinate with PT and the care coordination team when considering discharge planning goals, destination, and equipment needs. (Remember, discharge planning begins on the day of admission.)
- Compare preadmission/prior status, including ability to perform activities of daily living, to discharge status; i.e., PLOF compared to post-acute functional status.
- Use a multidisciplinary approach to review rehabilitation goals and ensure they’ve been met.
- Continue to complete BMAT 2.0 assessments per protocol. With any change in the patient’s ability to complete an assessment level, adjust mobility level and goals as needed.
Vital indicator
Mobility is a vital indicator of patient deterioration or improvement. Proper assessment using BMAT 2.0 can help predict mobility changes early so they can be addressed. In addition, it encourages evaluating patients’ pre-admission status and setting functional mobility goals, as well as promoting discharge planning that begins on the day of admission.
Standardizing nursing practice, processes, and procedures for SPHM equipment use promotes caregiver safety, reduces nursing care variability, results in better patient outcomes, and aligns with ANA’s standards.
Teresa Boynton is a clinical consultant at Mobility Consulting and Presentations, LLC, based in Loveland, Colorado. Dee Kumpar is the clinical marketing manager for patient support systems at Hill-Rom. Catherine VanGilder is a senior manager of medical affairs for patient support systems at Hill-Rom.
References
American Nurses Association. Safe Patient Handling and Mobility: Interprofessional National Standards Across the Care Continuum. Silver Spring, MD: American Nurses Association; 2013.
Boynton T, Kelly L, Perez A, Miller M, An Y, Trudgen C. Banner Mobility Assessment Tool for Nurses: Instrument validation. Am J SPHM. 2014;4(3):86-92.
Boynton T, Kelly L, Perez A. Implementing a mobility assessment tool for nurses. Am Nurse Today. 2014;9(suppl):13-6. myamericannurse.com/wp-content/uploads/2014/09/ant9-Patient-Handling-Supplement-821a_Implementing.pdf
Devlin JW, Skrobik Y, Gélinas C, et al. Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. 2018;46(9):e825-73.
Dickinson S, Taylor S, Anton P. Integrating a standardized mobility program and safe patient handling. Crit Care Nurs Q. 2018;41(3):240-52.
Dregne R, Koehne K. House-wide safe patient handling program to mobilize patients early and often: One organization’s journey. Int J Nurs Crit Care. 2018;2(1). scientonline.org/open-access/house-wide-safe-patient-handling-program-to-mobilize-patients-early-and-often-one-organizations-journey.pdf
Fox MT, Sidani S, Brooks D, McCague H. Perceived acceptability and preferences for low-intensity early activity interventions of older hospitalized medical patients exposed to bed rest: A cross sectional study. BMC Geriatr. 2018;18(1):53.
Goodson CM, Friedman LA, Mantheiy E, et al. Perceived barriers to mobility in a medical ICU: The patient mobilization attitudes & beliefs survey for the ICU. [Epub ahead of print]. J Intensive Care Med. 2018:885066618807120.
Hester JM, Guin PR, Danek GD, et al. The economic and clinical impact of sustained use of a progressive mobility program in a neuro-ICU. Crit Care Med. 2017;45(6):1037-44.
Hoyer EH, Friedman M, Lavezza A, et al. Promoting mobility and reducing length of stay in hospitalized general medicine patients: A quality-improvement project. J Hosp Med. 2016;11(5):341-7.
Klein K, Mulkey M, Bena JF, Albert NM. Clinical and psychological effects of early mobilization in patients treated in a neurologic ICU: A comparative study. Crit Care Med. 2015;43(4):865-73.
Klein KE, Bena JF, Mulkey M, Albert NM. Sustainability of a nurse-driven early progressive mobility protocol and patient clinical and psychological health outcomes in a neurological intensive care unit. Intensive Crit Care Nurs. 2018;45:11-7.
Knight J, Nigam Y, Jones A. Effects of bedrest 1: Introduction and the cardiovascular system. Nursing Times. 2018;114(12):54-7. nursingtimes.net/clinical-archive/cardiovascular-clinical-archive/effects-of-bedrest-1-introduction-and-the-cardiovascular-system-26-11-2018
Knight J, Nigam Y, Jones A. Effects of bedrest 5: The muscles, joints and mobility. Nursing Times. 2019;115(4):54-7. nursingtimes.net/clinical-archive/orthopaedics/effects-of-bedrest-5-the-muscles-joints-and-mobility-18-03-2019/
Ljungqvist O, Scott M, Fearon KC. Enhanced recovery after surgery: A review. JAMA Surg. 2017;152(3):292-8.
Nelson AL. Evidence-based guidelines for patient assessment, care planning, and caregiving practices in safe patient handling and movement. In Safe Patient Handling and Movement: A Practical Guide for Health Care Professionals. New York City: Springer Publishing; 2006.
Pandullo SM, Spilman SK, Smith JA, et al. Time for critically ill patients to regain mobility after early mobilization in the intensive care unit and transition to a general inpatient floor. J Crit Care. 2015;30(6):1238-42.
Parry SM, Puthucheary ZA. The impact of extended bed rest on the musculoskeletal system in the critical care environment. Extrem Physiol Med. 2015;4:16. ncbi.nlm.nih.gov/pmc/articles/PMC4600281
Üstün TB, Chatterji S, Kostanjsek N, et al. Developing the World Health Organization Disability Assessment Schedule 2.0. World Health Organization. May 20, 2010. who.int/bulletin/volumes/88/11/09-067231/en
Wald HL, Ramaswamy R, Perskin MH, et al. The case for mobility assessment in hospitalized older adults: American Geriatrics Society white paper executive summary. J Am Geriatr Soc. 2019;67(1):11-6.


















2 Comments.
Are there references available to shop for items for safe handling re: mobility for homebound clients and S.O.? I wanted to know more about assisted devices to assist with those who have significant bilateral lymphedema in lower extremities. With that said, I am interested in exploring benefits of devices similar to the ceiling lift mentioned in the article that might assist the client in sitting upright from a lying position in bed to sitting upright with more ease independently and from a sitting position at the side of the bed to standing before applying the use of a walker etc. Also, where can I find these machinery and assistive devices online? Thank you and best wishes to all for the upcoming new year.
Great article and so needed during COVID health care crisis.