
This is the third in a series of articles on promoting professionalism.
Consider this scenario: Over the past 28 months, clinical colleagues have reported the following about your nursing colleague Pat*:
• She went to a code lasting 20 minutes, but was gone for over an hour, delaying patient assessments. The unit manager shared this concern with Pat in a Cup of Coffee conversation.
• She didn’t complete wound care on a quadriplegic patient during her shift, putting the patient at risk for infection. Another nurse reported the incident to the charge nurse, who encouraged the coworker to initiate a Cup of Coffee conversation with Pat.
• She left the unit before administering a patient’s morning medication, which upset Dr. Stewart because the patient wasn’t given timely care.
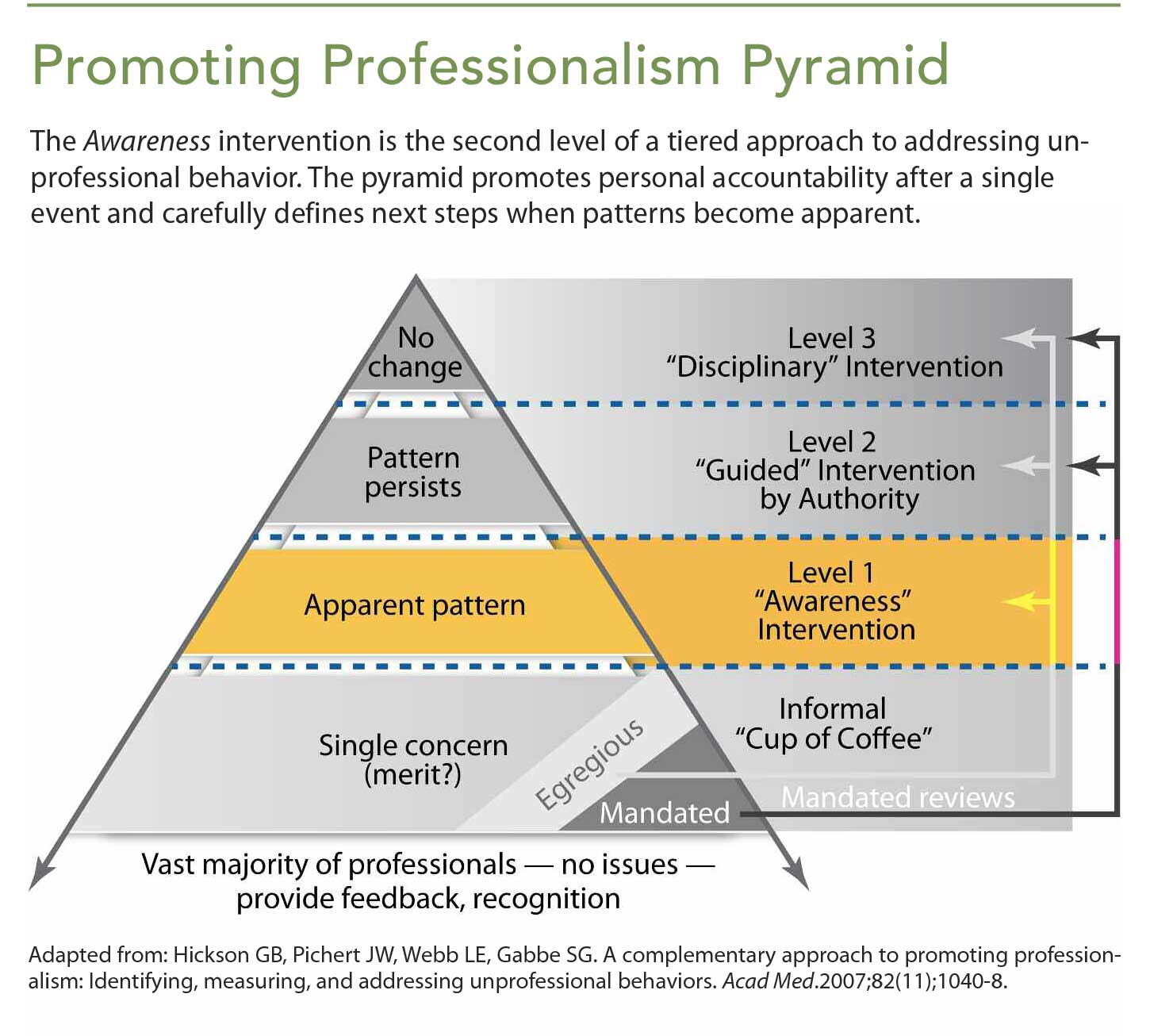
The first article in this series introduced the Promoting Professionalism Pyramid, a tiered intervention process for fostering professionalism and accountability. The second article focused on the Cup of Coffee conversation, which provides a way to informally discuss with a colleague how his or her observed behavior seems to undermine the organization’s culture of safety and respect. This third article highlights the next tier of the pyramid—the Awareness intervention. This level suggests that a colleague has a pattern of multiple concerns that makes him or her stand out from peers. (See Promoting Professionalism Pyramid.)
What’s an Awareness intervention?
Three reports signal an increasing concern about Pat’s pattern of behavior. By comparison, more than 80% of nurses at Pat’s medical center had no reports of unprofessional behavior over the same period; 15% had only one report. When a pattern of concerns suggests that a colleague stands out from his or her peers, the Promoting Professionalism Pyramid calls for an Awareness intervention, which also can be used to address a single egregious (but nonmandated) event.
Messengers (a trained leader or designated peer with the right to know the data) provide receivers (those whose unprofessional conduct has been observed or reported) with evidence of a pattern of behavior or performance inconsistent with organizational values or goals, along with meaningful comparative data. The data can include quantitative metrics (days late to work), semiquantitative observations (incomplete documentation), or qualitative reports (staff or patient complaints). Training is essential for any- one who plans to have an Awareness intervention. (See Who, what, where, when, why, and how.)
Benefits of Awareness interventions
Unsafe and disrespectful behavior patterns stem from both individual and system considerations, including fatigue, productivity and cost-containment demands, limited resources, interpersonal conflicts, and personal problems. However, none of these factors excuses unprofessional behavior. Most professionals are similarly pressed, but they provide safe, respectful care.
Unprofessional behavior persists when it’s permitted, often because of inadequate infrastructure supports. But it also goes unreported because of fear of retaliation, unwillingness to be a “tattletale,” reluctance to share uncomfortable stories, and concerns about offending people with special status or skills.
Estimates suggest 2% to 3% of staff display persistent unprofessional behavior. The question is whether and how you and your organization’s leaders address these individuals. When patterns are identified and addressed, Awareness interventions can be effective with individuals and entire units (for example, when addressing hand hygiene).
Success in promoting professionalism depends on:
• committed leadership, management, and peer professionals
• a goal-driven, fair model and process to guide graduated interventions
• multilevel, system-wide training in intervention-related skills.
When Awareness doesn’t work
Unfortunately, a small number of professionals seem unable or unwilling to respond to one or more Awareness interventions. These nurses, physicians, and other healthcare team members represent a threat to quality and safety, and they require Guided Interventions by authorities (for example, the clinician’s manager, supervisor, or other leader in the organization’s chain of command). In these situations, leaders develop improvement and evaluation plans with ongoing accountability. Despite the sincere desire to restore these clinicians to fully functioning professional performance, failure to respond to Guided interventions—either failing to follow the agreed upon plan or continuing to accumulate more concerning data—should lead to disciplinary action, the tip of the pyramid. (The last two steps of the pyramid will be discussed in the July issue of American Nurse Today.)
Consistent accountability
Most clinicians respond positively to Cup of Coffee and Awareness conversations. Promoting professional accountability consistently and reliably enhances awareness, reinforces core values, and builds rather than undermines a culture of safety and respect.
All authors work at Vanderbilt University Medical Center in Nashville, Tennessee. Marilyn Dubree is the executive chief nursing officer in clinical enterprise administration; April Kapu is associate chief nursing officer of advanced practice; Michelle Terrell is the director of advanced practice at Monroe Carell Jr. Children’s Hospital; James W. Pichert is professor of medical education and administration at the Vanderbilt Center for Patient and Professional Advocacy; William O. Cooper is professor and vice chair in the department of pediatrics, professor in the department of health policy, and director of the Vanderbilt Center for Patient and Professional Advocacy; Gerald B. Hickson is senior vice president for quality, safety and risk prevention, clinical enterprise administration, center for quality, safety and risk prevention.
*Names and scenarios are fictitious.
Selected References
Cooper WO, Guillamondegui O, Hines OJ, et al. Use of unsolicited patient observations to identify surgeons with increased risk for postoperative complications [published online ahead of print February 15, 2017]. JAMA Surg.
Donley, J. Defusing lateral violence and abuse. Am Nurs Today. 2012; 7(9):66,68.
Dubree M, Kapu A, Terrell M, et al. Nurses’ essential role in supporting professionalism. Am Nurs Today. 2017;12(4):6-8.
Dubree M, Kapu A, Terrell M, et al. Promoting professionalism by sharing a cup of coffee. Am Nurs Today. 2017;12(5):18-19.
Hickson GB, Moore IN, Pichert JW, Benegas M Jr. Balancing systems and individual accountability in a safety culture. In: Berman S, ed. From Front Office to Front Line: Essential Issues for Health Care Leaders. 2nd ed. Oakbrook Terrace, IL: Joint Commission Resources; 2012: 1-36.
Pichert JW, Moore IN, Karrass J, et al. An intervention model that promotes accountability: Peer messengers and patient/family complaints. Jt Comm J Qual Patient Saf. 2013;39(10):435-46.
Talbot TR, Johnson JG, Fergus C, et al. Sustained improvement in hand hygiene adherence: Utilizing shared accountability and financial incentives. Infect Control Hosp Epidemiol. 2013;11(34):1129-36.
Wahr JA, Prager RL, Abernathy JH III, et al. Patient safety in the cardiac operating room: Human factors and teamwork: A scientific statement from the American Heart Association. Circulation. 2013;128(10): 1139-69.
Webb LE, Dmochowski RR, Moore IN, et al. Using coworker observations to promote accountability for disrespectful and unsafe behaviors by physicians and advanced practice professionals. Jt Comm J Qual Patient Saf. 2016;42(4):149-64.
















{kind=link}
{kind=link}