How a correctional facility engages all staff in QI
Takeaways:
- The purpose of continuous quality improvement (QI) programs is to improve healthcare by identifying problems, implementing interventions, and monitoring and maintaining improvements over time.
- University Correctional Health Care has incorporated a QI model and developed an accompanying step-by-step training program so all staff can learn how to bridge the gap between “what is” and “what should be.” Use its experience to guide your own QI programs.
Editor’s note: This is a web exclusive article for the April 2021 issue of American Nurse Journal.
If organizations want to create healthcare that the Institute of Medicine describes as “safe, effective, patient centered, timely, efficient and equitable,” quality improvement (QI) is essential for everyone in every setting. For example, in the rapidly changing environment of correctional healthcare, we face challenges and competing priorities each day. Early problem identification and resolution make a difference in the lives of the patients we serve and the people we work with. At Rutgers University Correctional Health Care (UCHC), we created a practical approach to QI training so all staff can learn to bridge the gap between “what is” and “what should be,” no matter where they are in the organization.
Everyone’s business
Since 2008, UCHC has contracted with the New Jersey Department of Corrections to deliver mental, physical, and dental care to 19,212 inmates within 13 adult prisons. UCHC, like other systems, uses evidenced-based practices and continuous QI activities to ensure measurable healthcare delivery improvements are achieved, while at the same time satisfying contractual and accreditation obligations. To promote an excellence mindset, UCHC adopted the motto “QI is everyone’s business!” QI training is required for all staff, and new employees sign up for training within the first 90 days of hire to give them onsite experience before joining a performance improvement team. Monthly emails sent to all staff provide additional assistance with new or existing projects. The blend of new hires and seasoned staff participating in each QI project results in creative solutions.
Training begins with staff introductions, an overview of how QI is organized and incorporated into day-to-day work activities, and a description of the committees at each facility. Participants are asked about their own background and experience with QI. A brief QI definition is provided, and we explain the importance of using a structured QI model recommended by accrediting organizations, such as the National Commission on Correctional Health Care. The focus then turns to an overview of the QI model UCHC uses, which includes the four-step circular model: Plan/Design, Measure, Assess, and Improve. (See A model for QI.)
A model for QI
When using the Plan/Design, Measure, Assess, and Improve quality improvement (QI) model, teams may move back and forth between the steps until they achieve their goal.
QI Marg APlan/design
Plan/design, the most important step in the model, outlines the team’s “road map,” which governs the rest of the project. Activities focus on questions such as: What do we want to improve? How do we know improvements are needed? Are there data we can point to or feedback we can quantify? How do we define success? What are the team’s goals? Are they SMART goals (Specific, Measurable, Achievable, Realistic, and Timely)? How is the improvement initiative related to the mission and values of the organization? Have other correctional facilities faced the same issue and, if so, how did they remedy it? Did they face any obstacles and, if so, how did they overcome them?
The plan is developed by interprofessional teams consisting of staff closest to the identified problem, which helps ensure buy-in and a grassroots approach to problem solving. The team taps leaders and site administrators as needed to remove barriers and provide additional resources as the project progresses.
Next, the team seeks to determine the probable causes of the problem and potential interventions. They choose data collection methods and set a timeframe for meeting their goals. We’ve found that sufficient time spent in this step brings a tremendous pay off in the last steps. Many projects sink or fade away because the teams didn’t spend enough time in project planning and design.
Step 2. Measure
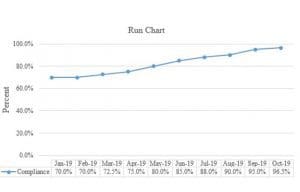
Data, which can be quantitative or qualitative, must be measured before and after an intervention to determine whether the project was successful. An example of a quantitative indicator is the number of times an intake screen was completed within 4 hours of arrival. A qualitative measure might be identifying common causes of patient accidents or unexpected deaths. Pre-intervention data provide a baseline. Setting a threshold for success helps set intervals between each data collection period. Teams can use run charts, such as the one below, to visualize trends, changes, and patterns over time as well as compare measures before and after an intervention. However, the team must determine a threshold (for example 97%) to monitor performance. If performance falls below the threshold, the team can re-examine the intervention and adjust as necessary.
Step 3: Assess
Assessment involves analyzing data to determine whether the intervention worked and the direction the team will take as a result. Team members can continue testing the intervention, modify a previous step if changes didn’t occur as expected, or decide the intervention was successful. This step also involves benchmarking, which compares outcome data against other resources, such as published research, other facilities, best practices, and past performance.
Step 4: Improve
If the intervention is successful, wider implementation is the next step, beginning with staff education. This also is the time to spread the word about the project’s success. Another department or facility may be able to adopt the intervention for QI. For example, a new workflow for a process that spans different departments within an organization, such as patient transfers from one level of care to another, ensures consistent care. Positive outcomes also should be shared with local and statewide QI committees, at staff meetings, and with leadership staff. If your state has a newsletter for nurses, submit a project summary for publication.
Successful project outcome doesn’t signify the end of the project. Continued measuring and monitoring at regularly scheduled intervals must be part of the plan to ensure improvements can be sustained. Change isn’t always easy, and some staff may revert back to old processes. Re-education, training, and policy revision may be necessary to create a new normal.
Training tools
After each step is reviewed in training, we conduct activities for the plan and design phase to give participants the experience of what it’s like to serve on a QI team. Based on the size of the training group, staff join teams with one or two trainers appointed to each. We ask staff to identify their roles, which can include a team facilitator who maintains the team’s momentum, a co-facilitator, a scribe, a meeting minutes taker, a data collector, and someone assigned to apprise the facility QI committees of the project’s status. The team works through a series of questions and activities using various QI tools (brainstorming, multi-voting, Pareto diagrams, fishbone diagrams, workflow diagrams, and success indicators).
What areas need improvement at your site?
To generate ideas and encourage participation, the team is instructed to brainstorm. Each team member shares an idea until all ideas are exhausted. The scribe writes the ideas on a flip chart. Staff are encouraged to focus on ideas rather than to discuss and debate. To ensure all staff members are included, no matter their role in the organization, trainers remind teams that no right or wrong suggestions exist and that everyone has an equal say in identifying problems.
Which problem is most important?
The team participates in multi-voting to help them narrow down the list of brainstormed ideas. Here’s an example of this tool in action: Each member uses a Post-it note to rank the top five ideas from a list of 10 they identified through brainstorming. A scribe collects the Post-it notes, tallies the votes, and lists the results on a flip chart. If the results indicate that one idea has the most support, the team moves forward with that idea. If a consensus isn’t clear, the process is repeated. (The team also can use a Pareto diagram to display the voting results from highest to lowest.)

What are the probable causes? Which should you address first?
Brainstorming and multi-voting are used to identify why the problem is happening and which probable cause to focus on first. The team won’t be able to work on all of them at one time, so limiting the team’s initial focus will help make their work manageable and ensure momentum.
Can you put the causes into categories?
To create a snapshot of collective knowledge around the problem and continue focusing on the main issues, the team completes a fishbone diagram. (See Fishing for causes.)
The problem is printed at the head of the diagram with each probable cause listed under appropriate categories, which are determined by the QI team based on the problems identified. Some problems will fit into multiple categories.
How would you fix the problem?
Using brainstorming again, the team identifies potential feasible interventions and then conducts multi-voting to make final determinations. Many interventions will require reviewing and revising existing workflows, an important step in QI. All steps in a process and the staff involved in performing each step must be outlined in a workflow diagram to identify issues in the “as it is” process and then establish the “as it should be” process. (See Improving a process.)
How will you know interventions worked?
Based on the QI goals, success indicators are defined so the team will know whether their intervention was successful. Teams can choose several areas to measure, including increased production, time efficiency, and staff or patient satisfaction surveys. The team must establish baseline thresholds that measure current indicators (“as it is”) and performance thresholds that measure indicators after the intervention has been applied to determine how much change, if any, has occurred. For example, if the QI project focuses on increasing the number of completed ECGs, the success indicators might include monthly audit compliance improvement, all staff trained on the updated workflow, all staff able to complete the workflow, improvement between pre- and post-intervention test results, decreased emergency department trips, decreased incomplete ECGs, and improved provider documentation.
Communication tips
Large and small organizations look for ways to communicate more effectively with their staff. At UCHC, we created QI Tips, which are emailed to all staff members periodically to reinforce what was learned in training. For example, in our tip for selecting an effective QI project, we emphasize that the process in need of improvement should be data-driven and prioritized based on one or more of the following:
- relates to the organization’s mission and values
- involves a high-risk process
- involves a high-volume process
- based on client needs
- based on staff views
- provides opportunities for savings.
Celebrate QI success
QI program sustainability emerges from empowering and reinforcing the importance of everyone working to identify areas for improvement and participating in activities to make improvements happen. In addition to reinforcing the importance of QI, we celebrate it. In 2006, UCHC adapted UBHC’s annual QI fair, where staff publicly display their projects and are congratulated for their efforts and contributions. Everyone is motivated and encouraged to engage in QI. After all, QI is everyone’s business.
Lisa Debilio is the quality improvement director, Christine Prestien-La Penta is the administrator of nursing services, and Jennifer VanEmburgh is the staff assistant at Rutgers University Correctional Health Care in Trenton, New Jersey. At the time this article was written, Marci Mackenzie was director of health operations and accreditation at the facility.
References
Institute of Medicine Committee on Quality of Health Care in America. Improving the 21st -century health care system. In: Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academies Press; 2001. ncbi.nlm.nih.gov/books/NBK222265
National Commission on Correctional Health Care. Standards for Health Services in Prisons. Chicago, IL: National Commission on Correctional Health Care; 2018.