
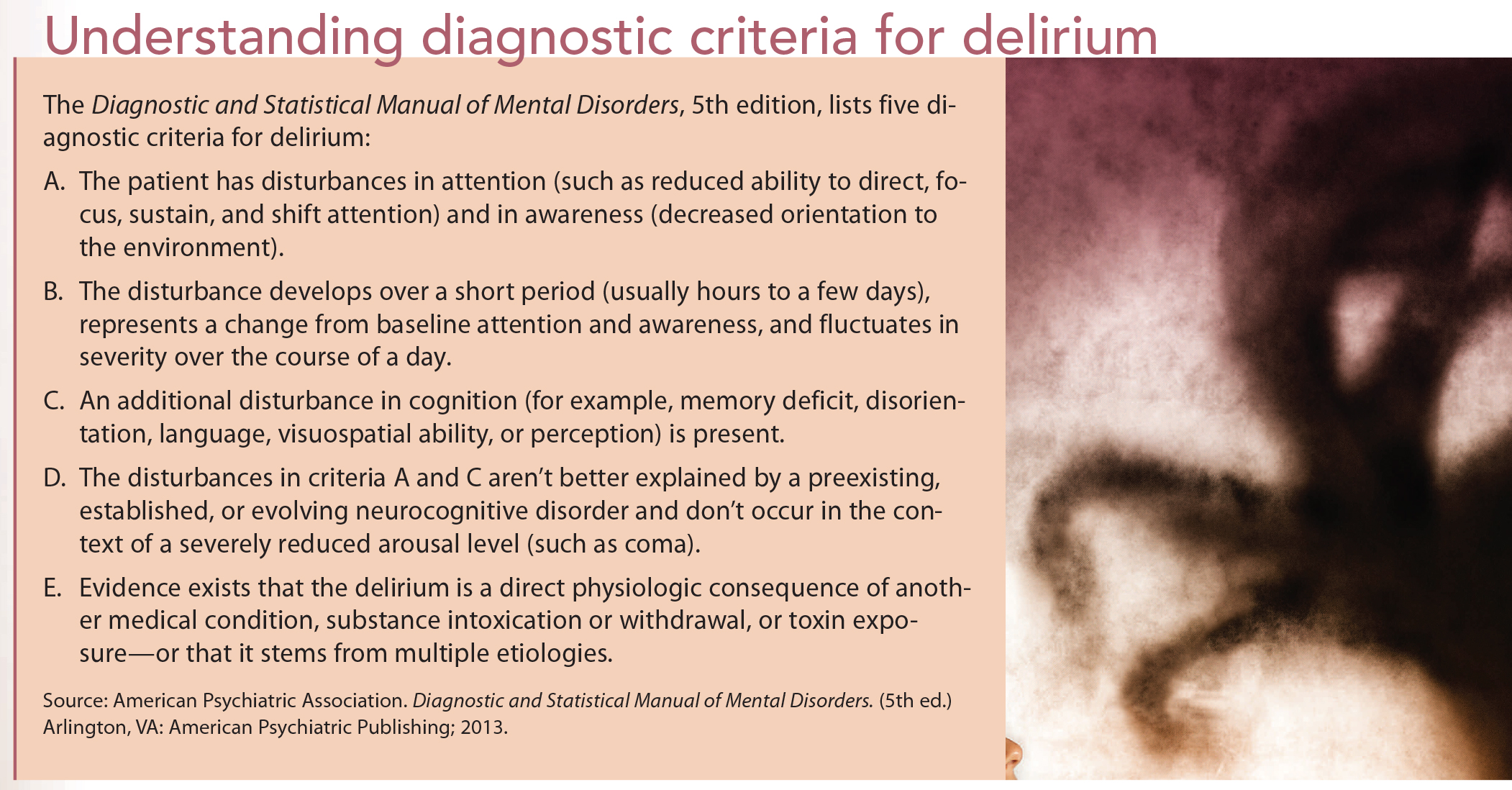
A syndrome of acute brain dysfunction, delirium causes observable changes in behavior. A hallmark of delirium is a disturbance of consciousness and cognition, with inattention that develops acutely and fluctuates over time. (See Understanding diagnostic criteria for delirium.)
In critically ill adults, delirium can lead to more ventilator days, more intensive care unit (ICU) days, longer hospital stays, longterm cognitive problems, and an increased mortality risk. Adults have described delirium as a frightening experience with periods of confusion and hallucinations, plus a sense that they’re in a horrific dream they can’t escape.
In pediatric patients, delirium often goes unrecognized, despite its prevalence. One study found delirium occurs in more than 30% of children ages 2 to 5 and more than 50% of critically ill children younger than age 2. Another study uncovered delirium in 20% of patients from birth to age 21 in the study population.
In yet another study, among 515 hospitalized pediatric patients who received psychiatric consultations for various symptoms, only six occurred because the medical team identified delirium symptoms. Of the 515 patients, 53 were diagnosed with delirium by psychiatrists, including the six referred by the medical team. That team missed 87% of patients with delirium.
Newly available diagnostic tools
Like many nurses, you may have witnessed patients with signs or symptoms of delirium or acute brain dysfunction but couldn’t identify the condition because you lacked diagnostic tools. Now that valid, reliable tools are available and delirium is known to significantly contribute to morbidity and mortality, several practice guidelines (such as the Society of Critical Care Medicine’s ABCDEF bundle) have been issued to help caregivers diagnose, manage, and preventive delirium in critically ill adults.
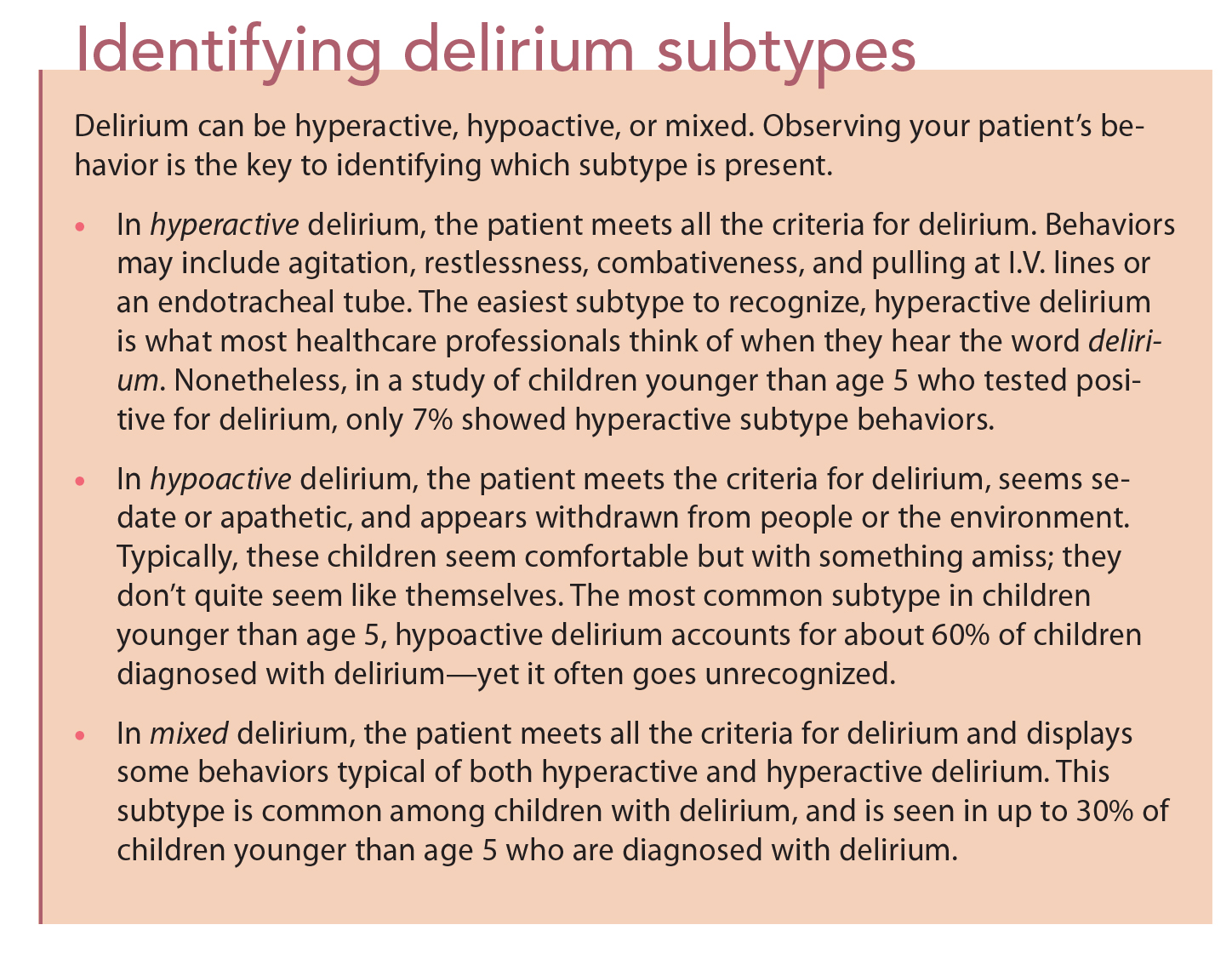
More recently, diagnostic tools have been developed to diagnosedelirium in children, helping caregivers identify the condition early in critically ill children. Easily used at the bedside even by clinicians who aren’t specialists in psychiatry, these tools can detect all three subtypes of delirium—hyperactive, hypoactive, and mixed. (See Identifying delirium subtypes.)
Assessment tools
Brain dysfunction caused by delirium leads to certain observable behaviors. Although the key features of delirium pertain to both pediatric and adult patients, symptoms in an 8-month-old infant may manifest differently than in an adult. To identify delirium in pediatric patients, you can use the assessment tools described below.
Cornell Assessment of Pediatric Delirium (CAPD)
Background: Adapted from the Pediatric Anesthesia Emergence Delirium tool to include screening for hypoactive delirium Sensitivity/specificity: Overall sensitivity of 94.1% and specificity of 79.2% in diagnosing delirium compared to the reference standard (psychiatrist)
Age range: 0-21 years
Description: The patient must have a Richmond Agitation and Sedation Scale (RASS) score of -3 or higher to warrant use of the CAPD. Two nurses assess the patient over a 24-hour period and answer eight questions about the patient’s cognition and mental status (using a Lickert scale) by answering never, rarely, sometimes, often, or always. Using developmental anchor points helps identify normal developmental activities for each question for patients younger than age 2. The nurse should assess the patient during the middle of the shift, scoring the answers to the eight questions. Delirium is present if the score is 9 or higher.
Bottom line: This tool doesn’t require direct verbal interaction with the patient. Also, the patient doesn’t have to demonstrate inattention (a cardinal feature of delirium) because this tool doesn’t directly test for it.
Pediatric Confusion Assessment Method for the Intensive Care Unit (pCAM-ICU)
Background: Developed for children at least ages 5 and older in developmental age; adapted from the Confusion Assessment Method for the Intensive Care Unit (CAMICU) for adults
Sensitivity/specificity: Overall sensitivity of 83% and specificity of 99% in diagnosing delirium compared to the reference standard (psychiatrist).
Age range: Ages 5 and older (developmental age)
Description: The patient must have a RASS score of -3 or higher. This tool uses the same four delirium features as the CAM-ICU—(1) acute change or fluctuation from baseline mental status, (2) inattention, (3) acute altered level of consciousness, and (4) disorganized thinking.
• Features 1 and 2 must be present for the patient to have delirium.
• If feature 1 isn’t present, stop the assessment; the patient is negative for delirium.
• If feature 1 is present, assess feature 2 by showing a series of pictures and asking the patient to remember them, or by asking the patient to squeeze your hand when he or she hears the letter “A” in a sequence of letters spoken aloud. If feature 2 isn’t present, stop the assessment; the patient is negative for delirium.
• If both features 1 and 2 are present, assess for feature 3—an acute altered level of consciousness. If the patient isn’t alert and calm, stop the assessment; the patient has delirium.
• If the patient is alert and calm, assess for feature 4 (disorganized thinking) by asking five questions and having the patient complete one command. If features 1, 2, and either 3 or 4 are present, the patient has delirium.
Bottom line: This objective and rapid assessment tool requires interaction with the patient because it assesses for delirium at a specific moment. It can be performed throughout the shift if the patient experiences mental-status changes.
Preschool Confusion Assessment Method for the Intensive Care Unit (psCAM-ICU)
Background: Developed to assess for delirium in children 6 ages months to 5 years in developmental age
Sensitivity/specificity: Overall sensitivity of 75% and specificity of 91% in diagnosing delirium compared to the reference standard (psychiatrist).
Age range: Ages 6 months to 5 years (developmental age)
Description: This tool was adapted from the pCAM-ICU to suit children with developmental ages of 6 months to 5 years. (Features 2 and 4 in pCAM-ICU aren’t developmentally appropriate for this age range.)
• For assessment of inattention in feature 2, show a series of 10 pictures and determine how long the pictures hold the child’s attention. The total possible score is 10.
• Feature 4 indirectly evaluates for system dysregulation by assessing for sleep-wake cycle disturbances. As with the CAM-ICU series, the patient must have a RASS score of -3 or higher and both features 1 and 2 must be present, along with either feature
3 or 4, to qualify for the diagnosis of delirium.
Bottom line: This tool is largely objective and efficient for delirium screening.
Nursing actions
Because nurses are at the patient’s bedside more consistently than other clinicians, we’re likely to notice subtle changes before anyone else does. Now that we have tools for identifying delirium in pediatric patients, let’s use them. Keep the following in mind when caring for children with delirium.
• Recognize that delirium is acute and will resolve. Your patient is not crazy.
• Work with the pediatric ICU staff and faculty to educate yourself about pediatric delirium. Establish a delirium monitoring protocol using a valid, reliable monitoring tool.
• Collaborate with child and adolescent psychiatrists early and consistently. They can prove invaluable not only in diagnosing delirium but also in managing patients with the condition.
• If your patient is delirious, first check for common causes (such as hypoxia, brain hypoperfusion, sepsis, electrolyte imbalances, trauma, drug withdrawal, and pain). If correcting the cause will take time (as with acute respiratory distress syndrome), consider limiting iatrogenic causes known to worsen delirium (such as increased benzodiazepine use and sleep-wake cycle disturbances.)
• Use a recognized preventive strategy, such as promoting good sleep hygiene, managing pain, and recognizing and treating drug withdrawal.
• Know what sedative drugs your patient is receiving, and monitor the target sedation level to ensure his or her safety. One study found that as little as 20 mg lorazepam in a 24- hour period can increase the risk of delirium to almost 100% in critically ill adults. The study is significant for pediatric clinicians because if that dosage caused delirium in nearly all critically ill adults, it’s almost guaranteed to cause it in a child who receives the same dosage over the same period. As the link between delirium and benzodiazepines is investigated further, we may need to reconsider such current practices as benzodiazepine infusions.
• Realize that pharmacologic management of delirium may not always be appropriate. However, if the patient presents a danger to the self, an antipsychotic agent may relieve unwanted behavioral manifestations until the cause of delirium resolves. Don’t be afraid to use pharmacologic management if appropriate, but know that drugs aren’t meant to be used long term. Finally, keep in mind that an awake brain is the first step toward a healthy brain. A child with an awake brain is one who isn’t receiving sedating medication, has adequate perfusion, and doesn’t have sleep-wake cycle disturbances.
Stacey Williams is a nurse practitioner in the pediatric critical care unit at Monroe Carell Jr. Children’s Hospital at Vanderbilt in Nashville, Tennessee.
References
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. (5th ed.) Arlington, VA: American Psychiatric Publishing; 2013.
Edwards S, Simone S, Pustilnik S, Walker LK, Lardieri A. The pediatric TEAM (Training Education, Assessment, & Management of Delirium) program: an interprofessional collaboration in the critical care setting. Poster presented at: Interprofessional Care for the 21st Century: Redefining Education and Practice; Jefferson Center for InterProfessional Education 2014 Conference, October 10, 2014; Philadelphia, PA: Thomas Jefferson University.
Flaigle MC, Ascenzi J, Kudchadkar SR. Identifying barriers to delirium screening and prevention in the pediatric ICU: evaluation of PICU staff knowledge. J Pediatric Nurs. 2016;31(1):81-4.
Kelly P, Frosch E. Recognition of delirium on pediatric hospital services. Psychosomatics. 2012;53(5):446-51.
Pandharipande P, Shintani A, Peterson J, et al. Lorazepam is an independent risk factor for transitioning to delirium in intensive care unit patients. Anesthesiology. 2006;104(1):21-6.
Smith HA, Boyd J, Fuchs DC, et al. Diagnosing delirium in critically ill children: validity and reliability of the Pediatric Confusion Assessment Method for the Intensive Care Unit. Crit Care Med. 2011;39(1):150-7.
Smith HA, Gangopadhyay M, Goben CM, et al. The Preschool Confusion Assessment Method for the ICU: valid and reliable delirium monitoring for critically ill infants and children. Crit Care Med. 2016;44(3):592-600.
Traube C, Silver G, Kearney J, et al. Cornell Assessment of Pediatric Delirium: a valid, rapid, observational tool for screening delirium in the PICU. Crit Care Med. 2014;42(3):656-63.


















{kind=link}
{kind=link}