
Give the right side of the heart the attention it’s due.
Takeaways:
- In right-sided heart failure, ventricular independence (between the right and left ventricles) can lead to systemic hypoperfusion (from reduced left ventricular filling), systemic venous congestion (from elevated central venous pressure), and fluid retention.
- Acute right-sided heart failure is associated with hemodynamic instability, especially when it’s due to massive pulmonary embolus, right ventricular myocardial infarction, or postcardiotomy shock after cardiac surgery.
- Volume management with loop diuretics and vasoactive therapies are the cornerstones of both acute and chronic right-sided heart failure treatment.
Heart failure management: Updated guidelines
Caring for patients with a left ventricular assist device
CNE
1.5 contact Hours
Learning Objectives
- Describe physiologic changes associated with right-sided heart failure (HF).
- Discuss clinical findings of right-sided HF.
- Discuss management of right-sided HF.
The authors and planners of this CNE activity have disclosed no relevant financial relationships with any commercial companies pertaining to this activity. See the last page of the article to learn how to earn CNE credit.
Expiration: 5/1/24
Right-sided heart failure (HF) doesn’t get the attention that left-sided HF receives, but it’s an important factor in HF symptom severity and mortality. Right-sided HF, which can cause or worsen pulmonary hypertension and left-sided HF, is defined as a structural or functional abnormality of the right heart circulatory system that impedes blood delivery to the pulmonary system or elevates venous pressures at rest or with exercise. Right ventricular dysfunction is the terminology used when a structural or functional abnormality that affects the right side of the heart is present, but patients are asymptomatic. Understanding right-sided HF pathophysiology, causes, and medical management can help nurses facilitate evidence-based care for their patients.
How the right ventricle works
The right ventricle is a thin-muscled, crescent shaped, low-pressure chamber that can accommodate large volumes of blood, which it ejects across the low resistance of the pulmonary circuit (the circulation between the heart and the lung).
Blood enters the ventricle from the venous circulation (systemic venous return) and exits to the pulmonary circuit. The right ventricle’s workload is much lower than the left (its contraction has lower peak systolic pressure and higher steady-state volume than the left ventricle), linking right ventricle function to its preload (circulating blood volume) and afterload (the force against which the right ventricle needs to generate enough pressure to overcome the pressure in the pulmonary vasculature), with afterload being the primary determinant of normal right ventricular function.
When pulmonary artery pressure rises (even slightly), right ventricle stroke volume decreases. The right ventricle becomes inefficient and uses more energy to maintain the balance between ventricular load and pulmonary arterial pressure. Unlike the left ventricle, which is perfused primarily during diastole, right ventricle coronary perfusion occurs during systole and diastole. If the right ventricle becomes pressure-overloaded, right ventricle coronary perfusion pressure (blood flow) decreases, increasing the risk for right ventricular ischemia. Ultimately, the right ventricle works best when the energy needed to produce contraction (to eject blood) occurs under low pressure.
Causes of right-sided HF
Right-sided HF has many causes. In adults without congenital heart diseases, it can occur after myocarditis, right ventricular myocardial infarction, cardiac surgery or transplantation, acute pulmonary embolus, tricuspid valve regurgitation, pulmonary valve disease, and arrhythmogenic right ventricular cardiomyopathy (a rare genetic disease of cardiac myocytes). Primary pulmonary arterial hypertension causes pulmonary vasculature alterations that lead to increased pulmonary resistance and right-sided HF, and alterations in pulmonary vasculature (for example, chronic thromboembolic disease) may lead to increased pulmonary vascular resistance, pulmonary embolus, and, ultimately, right-sided HF.
More commonly, though, right-sided HF occurs as left-sided HF advances and secondary pulmonary hypertension becomes prominent. Secondary pulmonary hypertension can occur in HF with reduced ejection fraction (HFrEF) and in HF with preserved ejection fraction (HFpEF), including restrictive cardiomyopathies. When HFpEF is associated with right-sided HF, distinguishing whether the cause is a primary right ventricular pathology or secondary pulmonary hypertension can be difficult because the right ventricle is afterload-dependent (it depends on pressure in the pulmonary artery). Secondary hypertension that results from chronic lung conditions (such as adult respiratory distress syndrome and chronic obstructive lung disease) also can lead to right-sided ventricular dysfunction and HF.
Right-sided HF prevalence can be as high as 50% of patients who are hospitalized for acutely decompensated HFrEF because decompensation frequently is coupled with pulmonary hypertension. According to Amsallem and colleagues, Harjola and colleagues, and Ponikowski and colleagues, prevalence varies with HFrEF etiology. For example, 60% of patients with dilated cardiomyopathy and 16% with ischemic cardiomyopathy have right-sided HF. In patients with HFpEF, 33% to 50% had right-sided HF. For patients who are in the early postoperative phase after receiving a left ventricular assist device, 20% develop right-sided HF.
Acute right-sided HF
Acute right-sided HF occurs when right ventricular afterload abruptly increases (caused by pulmonary embolus, hypoxia, or acidosis) or right ventricle contractility decreases (frequently caused by ischemia, myocarditis, or postcardiotomy shock from perioperative myocardial ischemia or injury). The right ventricle can handle volume changes (except excessive transfusion), but a sudden change in pressure can abruptly decrease right ventricular stroke volume. If contractility is impaired by an abrupt event, the right ventricle dilates, prompting tricuspid regurgitation, which exacerbates right ventricular dilation.
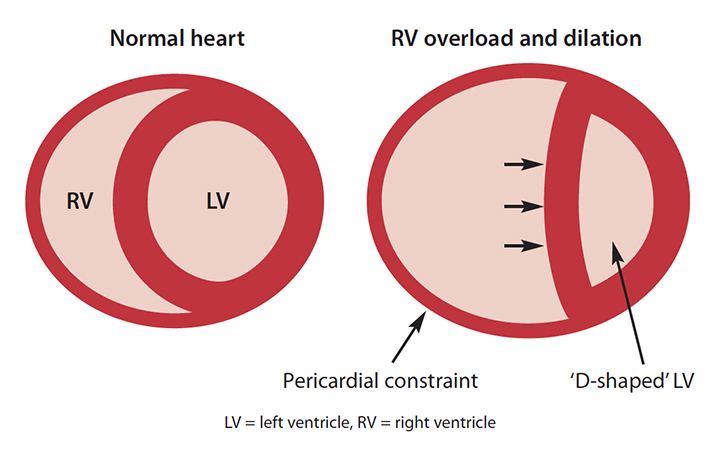
Pericardial constraint that prevents the right ventricle from enlarging outward creates ventricular interdependence, which disrupts left ventricular filling. (See Ventricular interdependence.) As left ventricular end-diastolic pressure increases and transmural filling pressure decreases, diastolic filling is impeded. Because less blood is available during left ventricular systole, systemic hypoperfusion results. As right heart filling pressures increase, systemic venous congestion increases, leading to hepatic congestion and impaired renal function, which can aggravate fluid retention and worsen right-sided HF.
Ventricular interdependence
Ventricular interdependence causes the interventricular septum to shift to the left and flatten, which causes the left ventricle cavity to become compressed and “D”-shaped, rather than maintaining its normal “O” shape.
Chronic right-sided HF
Chronic right-sided HF is associated with increased right ventricular afterload caused by pulmonary hypertension, which typically is caused by left-sided HF. Another common cause is chronic volume overload from left ventricular remodeling, as seen in HFrEF and HFpEF. If the right ventricle has myocyte loss or becomes hypertrophied and fibrotic, right ventricular systolic pressure increases and decompensation leads to a rise in peripheral vascular resistance and right atrial pressure. Over time, cardiac output declines.
If declining cardiac output is accompanied by declining pulmonary artery pressure in the presence of high pulmonary vascular resistance, mortality risk increases. In patients with an intact pericardium and right ventricular dilation, ventricular interdependence can lead to reduced cardiac output, impaired coronary blood flow, and increased peripheral and abdominal congestion.
Clinical characteristics and evaluation
Clinical characteristics of right-sided HF are caused by increased pressure in the right atrium (central venous pressure) and reduced left ventricular filling as a result of the effect of ventricular interdependence. Elevated central venous pressure impedes lung lymphatic drainage, so in patients with pulmonary hypertension resulting from left-sided heart diseases, lung fluid clearance decreases and excessive pulmonary edema can lead to pleural effusion. (See Signs and symptoms.)
Signs and symptoms
Signs and symptoms of acute and chronic right-sided heart failure (HF) worsen as right ventricular function worsens.
Acute right-sided HF
Signs
- Atrial and ventricular dysrhythmias
- High transaminase level
- Increased jugular venous pressure
- Prominent V wave during hemodynamic monitoring
- Right-sided third heart sound
- Tricuspid valve holosystolic murmur
Symptoms
- Cool extremities
- Diaphoresis
- Dyspnea (from diminished peripheral oxygen delivery)
- Hypotension
- Listlessness
- Pulmonary edema (if secondary to left-sided HF)
- Tachycardia
Chronic right-sided HF
Signs
- Atrial tachydysrhythmias (if elevated right atrial pressure)
- Hepatic congestion (right upper-quadrant discomfort) and reduced perfusion
- Hyperbilirubinemia (in patients with pulmonary hypertension)
- Moderate-to-severe tricuspid regurgitation (versus mild severity)
- Prolonged prothrombin time and elevated international normalized ratio
- Serum markers of cholestasis (elevated bilirubin and alkaline phosphate)
- Interstitial edema and increased inter-abdominal pressure
- Malnutrition and reduced absorption
- Peripheral edema (most prominent sign)
- Reduced serum albumin
- Visceral edema (caused by toxins in the gut lumen that leak into the bloodstream)
- Worsening renal function (due to increased central venous pressure and renal vein pressure)
- Decreased urine output
- Fluid retention
- Increased diuretic dosage
- Increased serum creatinine and blood urea nitrogen reflecting worsened status
Symptoms
- Exercise intolerance (due to reduced cardiac output)
- Fatigue (due to reduced cardiac output)
- Ventricular tachycardia/heart block (can lead to sudden cardiac death)
Acute-on-chronic left-sided HF signs and symptoms
- Ascites
- Hepatomegaly
- Peripheral edema
The kidneys, liver, and GI tract also are affected by chronic right-sided HF. Poor renal function and end-stage liver disease can increase mortality risk. In addition, renal function deterioration may be a marker of worsening cardiac function as a result of HF. If the patient is experiencing worsening renal function and elevated right-sided filling pressures, placing a pulmonary artery catheter may help determine true volume status and the need for loop diuretic therapy.
Patients with severe right-sided HF may be emaciated, tachypneic, and cyanotic, and they may have elevated jugular venous pressure. For patients with a noncompliant right ventricle, a Kussmaul’s sign may unmask venous hypertension. (See Kussmaul’s sign.) If pulmonary hypertension is the cause of right-sided HF, clinicians may hear a prominent pulmonic component of the second heart sound on auscultation. If coronary heart disease is part of the diagnosis, the pulmonic component of the second heart sound may be soft or absent.
Kussmaul’s sign
If a patient’s right ventricle is noncompliant, Kussmaul’s sign (increased right internal jugular venous pressure on inspiration) may be present. Check for this sign by performing the abdominojugular reflux test. Elevate the head of the bed to 45 degrees, and ask the patient to breath calmly. Note the pulsations in the internal jugular vein, then use the palm of your hand to apply firm pressure for at least 15 seconds (various sources list a range from 10 to 60 seconds) on the right upper-quadrant of the abdomen while you observe the vein. A positive Kussmaul’s sign is defined as an observed increase in internal jugular venous pressure (>3 cm) on inspiration that is sustained for more than 15 seconds.
Diagnostic testing
In addition to physical assessment, testing for right-sided HF consists of 12-lead ECG, echocardiogram (or alternative cardiac size and function tests, such as cardiac magnetic resonance imaging or positive emission tomography scan), and hemodynamic assessment.
ECG
Chronic right-sided HF is associated with a right-axis deviation and large P wave amplitude in leads II, III, and aVF. Sinus tachycardia is common, and the V1 lead may have a qR pattern. In addition, atrial fibrillation and atrial flutter are common.
Echocardiogram
The right ventricle’s retrosternal position, proximity to the chest wall, and complex nongeometric shape create inter-observer variability on echocardiograms. However, when using tissue Doppler, tricuspid annular plane systolic excursion (TAPSE) and right ventricular functional area change (RVFAC) are reproducible, feasible, easily obtained measures that reflect longitudinal right ventricular shortening. Reference limits of right ventricular function based on TAPSE and RVFAC are ≥1.8 cm (≥18 mm) and ≥35%, respectively.
Hemodynamic assessment
Right atrial pressure >15 mmHg is a marker of right ventricular dysfunction, especially when the elevation is disproportionate relative to the rise in pulmonary artery wedge pressure (normal right atrial/pulmonary artery wedge pressure ratio is about 0.5). In addition, elevated right atrial pressure will cause large atrial contraction waves (A waves) and large V waves, which signal a poorly compliant right atrium and tricuspid regurgitation.
Medical management
Managing acute right-sided HF focuses on reduced volume and preload, enhanced myocardial contractility, and reduced right ventricular afterload with pharmacologic therapies and mechanical circulatory support. (See Acute right-sided HF: Medical management.) In acute right-sided HF, the goal is decreased left atrial pressure to reduce congestion and central venous pressure to <12 mmHg (ideal is <8 mmHg) and reduced pulsatile right ventricular loading.
Acute right-sided HF: Medical management
Medically managing acute right-sided heart failure (HF) includes managing volume, improving systolic contraction, and decreasing pulmonary and systemic vascular resistance
Volume management
Manage volume using I.V. loop diuretics.
- Response may be suboptimal as a result of hypotension, elevated central venous pressure, renal venous congestion, low cardiac output, or oliguric acute kidney injury.
- Administer in patients with volume overload even if they’re hypotensive, but manage low blood pressure by repositioning (flat or flatter in the bed) or drug therapies that enhance contractility.
If the patient doesn’t respond to I.V. loop diuretics, consider these renal replacement therapies:
- Veno-venous hemofiltration
- Ultrafiltration (Assess blood pressure to ensure maintenance of optimal intravascular volume. Don’t remove fluid at a rate that exceeds the ability of extravascular fluid to shift into intravascular space.)
Vasoactive therapies
These therapies reduce afterload to enable more effective systolic contraction and to decrease pulmonary and systemic vascular resistance:
- I.V. vasodilators
- Nitroglycerin
- Sodium nitroprusside
- Oral vasodilators
- Phosphodiesterase-5 inhibitors
Enhance contractility with short-term infusions of I.V. inotropes, such as
- dobutamine, which has a short half-life with a rapid onset and offset and a lower risk of hypotension than milrinone
- milrinone (if the patient also is receiving beta-blocker therapy), which is less likely than dobutamine to cause drug tolerance but more likely to cause hypotension when administered as a bolus.
If the patient is hypotensive (systolic blood pressure <80 to 90 mmHg), optimal perfusion can be achieved using a combination drug with inotropic and vasopressor properties to improve coronary artery perfusion, augment arterial pressure, and reduce the risk of right ventricular myocardial ischemia.
- Alpha agonist (phenylephrine)
- Dopamine
- Norepinephrine
- Epinephrine
When medical therapies aren’t effective, temporary mechanical circulatory support with axial flow or extracorporeal centrifugal flow devices provide short-term right ventricular support. Surgical options (tricuspid and pulmonary artery procedures) offer intermediate-term support. When patients meet inclusion and exclusion criteria, total artificial heart, durable mechanical circulatory support (left ventricular assist) device, and cardiac transplantation offer long-term support.
Management goals for chronic right-sided HF include relieving congestion, inhibiting neuroendocrine stimulation with medications that block or inhibit the actions of hormones of the renin-angiotensin-aldosterone system and beta-adrenergic system, and increasing cardiac output and right-sided ejection fraction. If the patient has pulmonary arterial hypertension, management focuses on vasodilating the pulmonary vasculature. (See Chronic right-sided HF: Medical management).
Chronic right-sided HF: Medical management
Medically managing chronic right-sided heart failure (HF) includes volume management, beta blockade, and arterial vasodilation, as well as treating pulmonary arterial hypertension.
Volume management
Volume is managed using loop diuretics and sodium restriction.
- Loop diuretics
- Intensity of diuretic should be based on cause and severity of right-sided HF and coexisting renal disease.
- Serum laboratory monitoring is required to prevent development of prerenal azotemia.
- Large diuretic doses may be required due to upregulation of the renin-angiotensin-aldosterone system:
- Visceral edema reduces diuretic absorption and tubular drug delivery.
- Chronic sodium-potassium-chloride blockade from diuretic therapy can lead to hypertrophied distal nephron and rebound sodium absorption.
- Combination therapy of loop and thiazide diuretics may augment natriuresis (via sequential nephron blockade)
- The loop diuretic torsemide has consistent absorption (80% bioavailability) compared to furosemide (bioavailability ranges from 10% to 90%).
- Sodium restrictions (Recommendations are imprecise.)
- Restrict sodium to reduce congestion in bi-ventricular HF or isolated right-sided HF
- In 2013, the National Heart Failure guidelines from the American Heart Association/American College of Cardiology for dietary sodium restrictions were revised from <2,000 mg/day to <3,000 mg/day. The right-sided HF 2018 scientific statement also recommends <3,000 mg/day.
- Restricting fluid to 1.5 to 2.0 liters/day may reduce congestion and hyponatremia.
Renin-angiotensin-aldosterone system inhibitors and beta blockers
- Small-scale studies support the use of the following medications for patients who have chronic HF with reduced ejection fraction: an angiotensin-converting enzyme inhibitor or an angiotensin receptor blocker, beta-blocker, and mineralocorticoid receptor blocker.
Pulmonary arterial hypertension management
Pulmonary artery vasodilator therapy relieves right ventricular afterload.
- Prostacyclin analogs include
- I.V. epoprostenol
- inhaled iloprost
- inhaled treprostinil
- Phosphodiesterase-5 inhibitors include
- sildenafil
- tadalafil
- Endothelin receptor antagonists provide short-term hemodynamic benefits but don’t reduce morbidity and mortality.
- Right-sided HF is associated with hepatic congestion. Endothelin receptor antagonists increase hepatic aminotransferases, so the patient’s liver function should be monitored.
Nursing implications
Understanding the diverse pathophysiology of acute and chronic right-sided HF helps nurses recognize and identify these conditions and promptly communicate with providers to enhance right ventricular unloading (for example, avoiding excessive volume administration) and improve left ventricular function. Right ventricular unloading is important because it may minimize central and renal venous engorgement and reduce the risk or severity of cardiorenal syndrome.
Nurses also can provide patient education about sodium and fluid restriction goals; however, large-scale research study findings on these restrictions aren’t currently available. In addition, nurses can advocate for optimal medical therapies based on the cause of right-sided HF and provide psychological support to patients and families, given the poor prognosis.
Helping patients
Right-sided heart failure is associated with impaired renal and hepatic function that increases morbidity and mortality. Management is aimed at palliative support to relieve congestion, improve exercise tolerance, and reduce afterload. Nurses can help patients understand the pathophysiology of their symptoms and the importance of seeking care when symptoms worsen. AN
Nancy M. Albert is associate chief nursing officer of research and innovation at the Zielony Nursing Institute at the Cleveland Clinic in Cleveland, Ohio, and a clinical nurse specialist at the Kaufman Center for Heart Failure Treatment and Recovery, Heart, Vascular and Thoracic Institute at the Cleveland Clinic.
References
Amsallem M, Mercier O, Kobayashi Y, Moneghetti K, Haddad F. Forgotten no more: A focused update on the right ventricle in cardiovascular disease. JACC Heart Fail. 2018;6(11):891-903. doi:10.1016/j.jchf.2018.05.022
Gorter TM, Hoendermis ES, van Veldhuisen DJ, et al. Right ventricular dysfunction in heart failure with preserved ejection fraction: A systematic review and meta-analysis. Eur J Heart Fail. 2016;18(12):1472-87. doi:10.1002/ejhf.630
Gorter TM, van Veldhuisen DJ, Bauersachs J, et al. Right heart dysfunction and failure in heart failure with preserved ejection fraction: Mechanisms and management. Position statement on behalf of the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail. 2018;20(1):16-37. doi:10.1002/ejhf.1029
Harjola VP, Mebazaa A, Čelutkienė J, et al. Contemporary management of acute right ventricular failure: A statement from the Heart Failure Association and the Working Group on Pulmonary Circulation and Right Ventricular Function of the European Society of Cardiology. Eur J Heart Fail. 2016;18(3):226-41. doi:10.1002/ejhf.478
Konstam MA, Kiernan MS, Bernstein D, et al. Evaluation and management of right-sided heart failure: A scientific statement from the American Heart Association. Circulation. 2018;137(20):e578-622. doi:10.1161/CIR.0000000000000560
Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2015;28(1):1-39.e14. doi:10.1016/j.echo.2014.10.003
Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: The task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37(27):2129-2200. doi:10.1093/eurheartj/ehw128
Ryan JJ, Tedford RJ. Diagnosing and treating the failing right heart. Curr Opin Cardiol. 2015;30(3):292-300. doi:10.1097/HCO.0000000000000164
Soliman O, Muslem R, Caliskan K. Right heart failure syndrome. Aging (Albany NY). 2018;11(1):7-8. doi:10.18632/aging.101708
Thandavarayan RA, Chitturi KR, Guha A. Pathophysiology of acute and chronic right heart failure. Cardiol Clin. 2020;38(2):149-60. doi:10.1016/j.ccl.2020.01.009

















1 Comment.
this is an excellent article– I will use in my practice and to teach nursing students.