
Universal violence precautions in acute care
Takeaways:
- Workplace violence can surprise and overwhelm nurses, leaving them unable to safely provide patient care.
- A multi-component intervention is needed to effectively prevent and mitigate workplace violence and its effects on patients, workers, and employers.
- A federal “standard” for workplace violence has the potential to provide consistency in hospital workplace violence prevention and management.
Zeke*, an emergency department (ED) nurse, hears yelling coming from room D7. He knocks on the room’s glass door, but the yelling continues. He attempts to push the door open, but it’s blocked. Behind the glass door is a closed curtain; under the curtain he sees someone lying on the floor. Zeke immediately calls for security and staff assistance. As security arrives, the patient door swings open and the patient’s parent exits the room throwing an object at Zeke saying, “Get out of my way!” De-escalation interventions are ineffective. The patient’s parent says very slowly and deliberately, “If you touch me, I swear I’ll follow you home tonight and kill you—kill your family and kill your pets.” Later during the shift, Zeke has difficulty focusing on patient care. On his next shift, he asks to be assigned to a different area of the ED so he won’t have to go back into room D7 again.
This true story is just one example of the increase in workplace violence (WPV) by patients and visitors.
The prevalence of WPV by patients and visitors is increasing. It’s particularly pervasive in emergency and psychiatric departments, but it also occurs in medical/surgical and other hospital units. The Government Accountability Office (GAO) reported that WPV in hospitals is approximately five times greater than in all private industries, and healthcare-related WPV fatalities comprise 3% of WPV fatalities across all private industries. About one-third of WPV incidents are significant enough to warrant physical intervention. Violence that nurses experience at work can surprise and overwhelm them, leaving them unable to safely provide patient care.
Workplace assault model
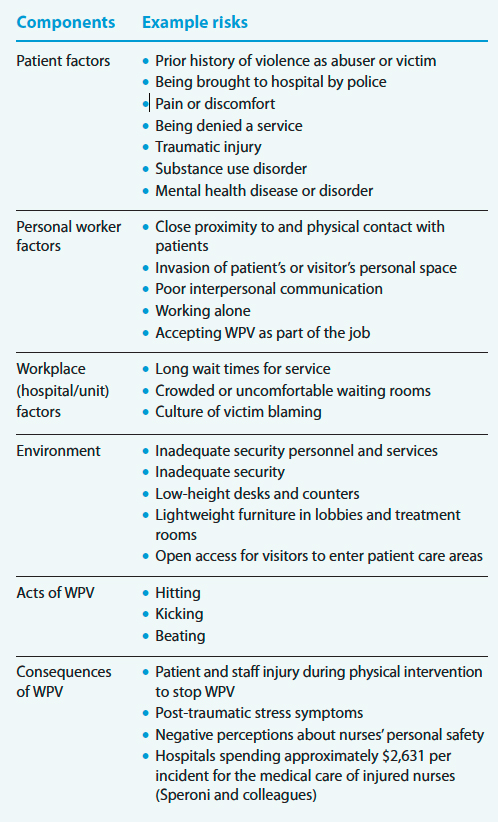
The Ecological Occupational Health Model of Workplace Assault can help nurses identify risk factors and outcomes linked to WPV and ultimately develop prevention strategies. The model includes six components: patient factors, personal worker factors, workplace (hospital/unit) factors, work environment, acts of WPV, and WPV consequences. (See WPV risks.)
WPV risks

The Ecological Occupational Health Model of Workplace Assault outlines six components related to workplace violence (WPV). They’re listed below with examples of risks for each.
Patient factors
Organizations can leverage electronic health records to prevent WPV by flagging a history of violence (for example, assault of a healthcare worker, domestic violence, brought to hospital by police) and linking the patient care plan to the flagged chart so patient-centered care can be provided to reduce the likelihood of a future incident. To prevent flagging bias from nurses responding to a violent incident, a hospital social worker or risk manager should assign the flag. Administrators should periodically assess whether continuing to flag a patient’s chart is needed.
The flag, depending on software capability, guides healthcare workers who care for the patient in the future. For example, the flag might direct nurses to contact security for relevant details during the next hospital visit or instruct nurses to always have a second employee in the room when care is delivered.
For patients who are victims of violence (intimate partner violence, community or gang violence), an alias, such as “Trauma Ohio,” can be used in lieu of the patient’s real name to prevent an aggressor from locating a patient victim and causing more harm. At discharge, the Trauma Ohio chart, which generates a new medical record number, is merged with the patient’s health records.
Personal worker factors
Reduce your risk of being assaulted by maintaining an appropriate distance from patients, not invading a patient’s personal space, watching for cues of potential WPV, and maintaining situational awareness. Train unlicensed assistive personnel to identify and report signs of escalation using STAMPEDAR (staring, voice tone and volume, anxiety, mumbling, pacing, emotions, disease process, assertive/nonassertive behavior, and resources). Reporting prompts nurses to implement de-escalation and violence prevention strategies.
One strategy is to stand or sit at the patient’s eye level, maintaining a 4- to 6-foot distance. Sitting or standing at eye level improves interpersonal communication and balances any power differential that might occur if you or the patient is standing above the other. Distance protects you from being hit, kicked, or beaten. It also reduces the chance of being struck by objects or body fluids (such as spit or urine). Of course, maintaining this distance isn’t always possible when conducting physical exams and providing care. In all cases, explain to the patient what you’re going to do before performing any care, and ask a second healthcare worker to be in the room with you to monitor patients with a history of violence for signs of escalation and intervene if needed.
At shift change, inform the team about tense situations or individuals who acted violently or are at risk of escalating. Provide similar information when you go on break or leave the unit. This process can help ensure aggressors have an opportunity to state their needs, which can help prevent further WPV.
Workplace factors
Establish a WPV prevention team of nurses from all areas and levels of the hospital to implement a multicomponent strategy for addressing WPV. A team co-led by a staff nurse and a high-level administrator, combined with a policy that includes multilevel strategies for preventing and managing WPV, will demonstrate management’s commitment to violence prevention. Hospital administrators, staff nurses, security personnel, and other members of the WPV prevention team should conduct regular hazard assessments (such as walk throughs, staff interviews, WPV trend analyses, identification of jobs and departments with high WPV rates), survey employees about WPV, and provide annual training for all employees and quarterly training for those working in high-risk departments and roles.
Use the assessment results to identify and mitigate risk factors, such as long wait times, crowded or uncomfortable waiting rooms, and a culture of victim blaming. Augment online and self-study training with active learning strategies, such as role-play, simulations, and drills.
The policy should include no tolerance for WPV; mandatory and nonpunitive reporting of assaults, threats, and significant verbal abuse; WPV discussions at staff meetings; and post-incident reviews immediately after WPV occurs. Successful workplace interventions require adequate staffing (or human resources) to effectively manage patient care and prevent WPV onset.
Work environment
A workplace environment designed to protect nurses requires a variety of strategies. Security devices such as metal detectors, closed-circuit television (CCTV), panic buttons, and personal alarms are common in many organizations. A CCTV monitor that’s periodically watched by clerical staff and the security department can help expedite staff response in departments or units with a high WPV prevalence. Random drills help assess security and safety team response to activated panic buttons and personal alarms. Timely responses require adequate numbers of security personnel around the clock.
When you’re in a patient room, position yourself between the patient and an unblocked exit door so you can easily escape if necessary. Security officers should be visible in lobby areas and outside treatment rooms to deter WPV escalation.
The physical design of departments and rooms can help prevent or mitigate WPV. Shatterproof glass panels on patient room doors and draw curtains set about one foot from the floor increase visibility, which enables others to see violent encounters and intervene. Tall, deep counters reduce the chances that an aggressive person will jump them to gain access to restricted areas or reach across and grab at nurses and other hospital personnel. All pieces of furniture in lobbies and patient treatment areas should be heavy enough that they can’t be picked up and thrown. In addition, permanently mounted wall plaques and pictures will prevent them from being used as projectiles.
Visitor restriction policies help control entry into a unit, and department design can prevent access by unauthorized individuals. The ability to implement a lockdown in the event of a significant threat, such as a patient or visitor with a knife or firearm, is critical to safety. Lockdown procedures vary based on the nature of the event. For an active shooter event, a total lockdown should create a perimeter of closed and secured doors to prevent anyone from entering or exiting. Each door should be guarded by an employee, preferably security or police personnel.
Acts of WPV
When de-escalation techniques aren’t effective and a person’s behavior escalates to physical violence, you must act quickly. Increase the distance between you and the aggressor. They may perceive you as less of a threat as you back away or leave the area. Call for assistance, preferably from a specialized team trained to respond to acts of physical violence. Enlist other team members to stand by but maintain an appropriate distance. If possible, identify and remove the trigger for the violent event. Frequently, patients have needs that aren’t being met (their pain isn’t being effectively managed, they want to be discharged, their preferred treatment isn’t being offered or provided). Addressing the trigger may increase the chances of de-escalating the situation. If possible, someone not involved in the patient’s daily care should assume all interactions with the patient until the violence is resolved.
Only as a last resort should physical restraints be used. Apply restraints humanely using a coordinated team approach to prevent injury to the patient and healthcare team. For example, each team member can be assigned an extremity before attempting a physical intervention, with a fifth team member responsible for head immobilization and airway maintenance.
WPV consequences
Immediately after a WPV incident, medical care should be provided to anyone injured, including the aggressor. Nurses also may require a medical screening in the employee health department or ED, even if they don’t have an apparent injury.
The nurse who was assaulted and other witnesses to the event should complete an incident report before the end of their shifts. Risk managers can use data from incident reports, screening examinations, and medical care expenses to develop practices to reduce future WPV. A debriefing, led by an administrator or another designated individual (such as a member of the WPV prevention team or a mental health worker), with the patient and care team will help everyone understand why the event occurred and discover safe methods to ensure patient and family needs are met in the future. Nurses can be trained to provide defusing techniques to coworkers who are WPV victims. Defusing is similar to critical incident stress debriefing, but it’s shorter and less formal and can take place during the same shift as the incident.
Nurses who’ve been victims of WPV should be assessed for psychological injury. They can be referred to an employee assistance program (EAP), but these programs aren’t always effective in WPV situations because of stigma associated with formal mental health counseling. Hospital chaplains and EAP counselors can regularly visit nurses to assess their mental health and provide recommendations for overall stress reduction. Support from unit managers and other leaders should include encouraging nurses to seek mental health care services.
If a physical assault occurs, nurses can be encouraged and supported to file a police report documenting the WPV.
Health policy recommendations
According to Richard Mereu, JD, MBA, of the Emergency Nurses Association, in 31 states WPV against a healthcare worker is a felony. These laws vary and aren’t consistently enforced, warranting the need for a federal Occupational Safety and Health Administration (OSHA) standard for WPV in healthcare settings.
In response to a 2015 request from the U.S. Congress, the GAO delivered a report with three recommendations calling for OSHA to take the following steps:
- Provide examples and additional information for inspectors to consider during inspections in relation to issuing a citation for WPV.
- Follow up with hospitals to ensure they’re addressing the problems noted in warning (hazard alert) letters.
- Assess efforts to reduce WPV and whether a standard is needed.
In 2017, OSHA held a public meeting inviting healthcare stakeholders to comment on whether a WPV standard is needed. To date, an OSHA standard hasn’t been adopted. In February 2019, U.S. Representative Joe Courtney introduced HR 1309 Workplace Violence Prevention for Health Care and Social Service Workers Act. This bill was never discussed by the U.S. Senate.
Although OSHA doesn’t require employers to implement WPV programs, it provides voluntary guidelines and may cite employers for failing to provide a workplace free from recognized serious hazards. Some states have legislated that employers develop a WPV prevention program, and many states have designated penalties for assaults on nurses. Learn more at nursingworld.org/practice-policy/advocacy/state/workplace-violence2/.
Nurses have a professional obligation to work with policymakers to adopt laws with meaningful protections. Demonstrate your support by encouraging OSHA to complete its planned assessment of WPV program effectiveness to reduce assault rates in healthcare settings. Contact your U.S. Representative and Senators to cosponsor the new bill when it’s introduced, which when passed will initiate the process toward a national WPV management program standard. If passed, the bill will require employers to
- investigate WPV incidents, risks, or hazards as soon as practical
- provide training and education to employees who may be exposed to WPV hazards and risks
- meet record-keeping requirements
- prohibit acts of discrimination or retaliation against employees for reporting WPV incidents, threats, or concerns.
Share WPV program success
Nurses shouldn’t be expected to care for patients in an unsafe, violent work environment. They’re at risk for physical and emotional injury, and hospitals are responsible for the costs associated with WPV. Given the limited lack of literature on interventions shown to prevent WPV, an urgent need exists to test the effectiveness of WPV programs and publish results so other healthcare organizations can adopt similar practices. This dissemination can help legislators and OSHA adopt a meaningful standard to protect nurses.
*Name is fictitious.
Access references at myamericannurse.com/?p=72933.
Gordon Lee Gillespie is a professor and associate dean for research at the University of Cincinnati College of Nursing in Cincinnati, Ohio. Steven J. Palazzo is an associate professor and associate dean for academic affairs at the University of Nevada Las Vegas School of Nursing.
References
American Nurses Association. Issue brief: Reporting incidents of workplace violence. 2019. nursingworld.org/globalassets/practiceandpolicy/work-environment/endnurseabuse/endabuse-issue-brief-final.pdf
American Nurses Association. Violence, incivility, & bullying. nursingworld.org/Bullying-Workplace-Violence
Arbury S, Hodgson M, Zankowski D, Lipscomb J. Workplace violence training programs for health care workers: An analysis of program elements. Workplace Health Saf. 2017;65(6):266-72.
Gillespie GL, Fisher B, Kennebeck S, et al. Leveraging a public health framework and community advisory board to innovate workplace violence intervention strategies. Adv Emerg Nurs J. 2019;41(4):357-71.
Hamblin LE, Essenmacher L, Luborsky M, et al. Worksite walkthrough intervention: Data-driven prevention of workplace violence on hospital units. J Occup Environ Med. 2017;59(9):875-84.
Havaei F, MacPhee M, Lee SE. The effect of violence prevention strategies on perceptions of workplace safety: A study of medical-surgical and mental health nurses. J Adv Nurs. 2019;75(8):1657-66.
International Association of Healthcare Security and Safety. Healthcare Security Industry Guidelines. Chicago, IL: International Association of Healthcare Security and Safety; 2018.
Lamont S, Brunero S. The effect of a workplace violence training program for generalist nurses in the acute hospital setting: A quasi-experimental study. Nurs Educ Today. 2018;68:45-52.
Levin PF, Hewitt JB, Misner ST, Reynolds S. Assault of long-term care personnel. J Gerontol Nurs. 2003;29(3):28-35.
Lipscomb J, London M. Not Part of the Job: How to Take a Stand Against Violence in the Work Setting. Silver Spring, MD: American Nurses Association; 2015.
Occupational Safety and Health Administration. Guidelines for Preventing Workplace Violence for Healthcare and Social Service Workers. 2016. osha.gov/Publications/osha3148.pdf
Peek-Asa C, Casteel C, Rugala E, Holbrook C, Bixler D, Ramierz M. The threat management assessment and response model: A conceptual plan for threat management and training. Security J. 2017;30(3):940-50. doi:10.1057/sj.2015.14
Registered Nurses’ Association of Ontario. Preventing Violence, Harassment and Bullying Against Health Workers. 2nd ed. Toronto, Ontario: Registered Nurses’ Association of Ontario; 2019.
Ridenour ML, Hendricks S, Hartley D, Blando JD. Workplace violence and training required by new legislation among NJ nurses. J Occup Environ Med. 2017;59(4):e35-40.
Schoenfisch AL, Pompeii LA. Security personnel practices and policies in U.S. hospitals: Findings from a national survey. Workplace Health Saf. 2016;64(11):531-42.
Speroni KG, Fitch T, Dawson E, Dugan L, Atherton M. Incidence and cost of nurse workplace violence perpetrated by hospital patients or patient visitors. J Emerg Nurs. 2014;40(3):218-28.
U.S. Government Accountability Office. Workplace Safety and Health: Additional Efforts Needed to Help Protect Health Care Workers from Workplace Violence. March 2016. gao.gov/assets/680/675858.pdf

















