
Since its emergence, Zika virus has been a source of concern and confusion for many people worldwide, particularly in today’s era of instant messaging and misinformation. However, because nurses spend more time with patients and their families than any other healthcare professionals, they are in a unique position to act as an effective communication hub for accurate information on Zika—and to help dispel ongoing myths.
Rise of Zika virus
In September 2015, Brazilian health officials noted an increase in infants born with microcephaly, a congenital condition in which the infant’s head is smaller than normal and often is associated with anomalies in brain development. In May of that year, the Pan American Health Organization had issued an alert concerning the first confirmed Zika virus infection in Brazil. Brazilian local health authorities also had observed an increase in Guillain-Barré syndrome (GBS), which coincided with Zika virus infections in the general public. In a retrospective review of a similar outbreak in French Polynesia in 2013-2014, national health authorities had reported potential neurologic and congenital complications associated with Zika. As the virus spread rapidly throughout the Americas, world health agencies became increasingly alarmed about its global impact. On February 1, 2016, the World Health Organization (WHO) declared Zika virus a public health emergency of international concern.
Public health emergency of international concern
The term “public health emergency of international concern” is defined by the International Health Regulations (2005) as “an extraordinary event which is determined…to constitute a public health risk to other States through the international spread of disease; and to potentially require a coordinated international response.” This definition implies a situation that is serious, unusual, or unexpected; carries implications for public health beyond the affected state’s national border; and may require immediate international action.
Myths persist
In spite of intense international focus and reporting on Zika, recent surveys by the Annenberg Public Policy Center of the University of Pennsylvania and the Harvard T. H. Chan School of Public Health indicate significant misconceptions about the virus.
Myth : Zika virus can be transmitted through coughing or sneezing
Zika virus primarily is transmitted by the bite of an infected Aedes species mosquito (A. aegypti or A. albopictus), which also can spread dengue, chikungunya, and yellow fever viruses. Zika also can spread through the semen of a symptomatic man to his sexual partners. To date, no transmission has occurred from men who do not exhibit symptoms. Zika survives longer in semen than in blood, although the actual infective period is unknown.
No cases have been reported of women transmitting the virus sexually. Infected women who are pregnant, however, run the risk of transmitting the virus to the fetus, resulting in microcephaly and other neurologic anomalies. Also, Brazilian health officials have reported multiple Zika transmissions by blood transfusion, which are being investigated. In the United States, no confirmed cases of blood-transfusion transmission have been reported. Zika does not spread through coughing or sneezing the way some other viruses (such as the common cold) can.
Myth : Nonpregnant women who are infected with Zika virus run risks of birth defects in future pregnancies
No evidence exists to suggest a nonpregnant woman infected with Zika virus, whether symptomatic or not, is at risk of Zika-related birth defects in future pregnancies. The virus usually remains in the blood of an infected person for about 1 week in the overwhelming majority of cases. Also, once a person has been infected, he or she is likely to be protected from future infections.
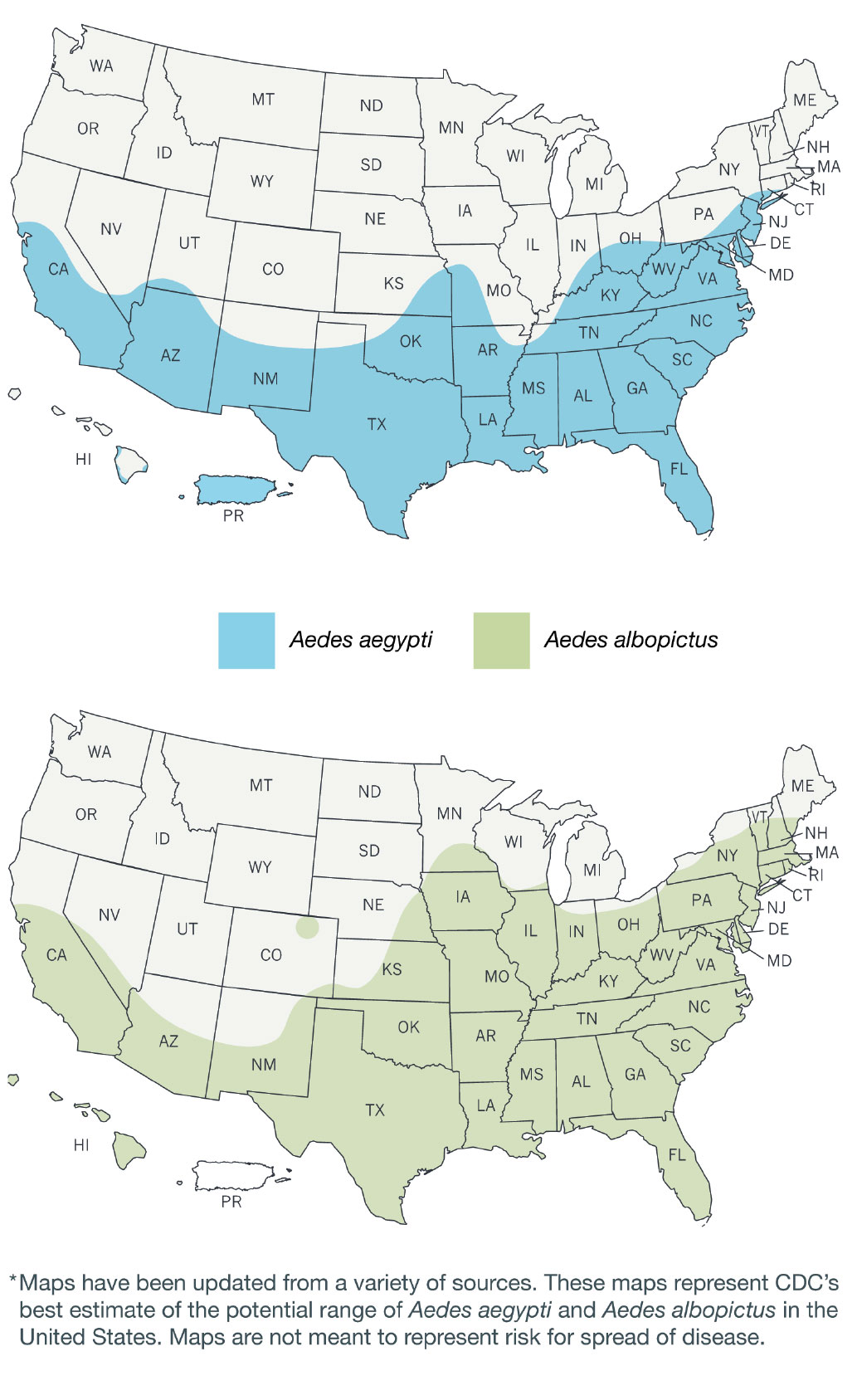
Myth : The Aedes species mosquito can travel around the world and is prevalent throughout all of the United States
The A. aegypti mosquito evolved with humans and is the more likely variant to transmit Zika virus. It prefers humans to other blood sources and can feed as often as every other day. It typically breeds in domestic water-holding containers. An aggressive daytime biter, it feeds both indoors and outdoors near dwellings. That said, it is a weak flyer, traveling only about 1,300 feet during its 30-day life cycle.
Its eggs, however, are quite resistant to environmental factors, remaining viable (and being transported) for months even in the absence of water. Mosquitoes prefer warm, wet environments and rarely survive at altitudes higher than 1 mile (5,280 feet) or in colder climates. For that reason, seasonal fluxes of Zika virus outbreaks are expected.
The maps (from the Centers for Disease Control and Prevention) show the estimated range of A. aegypti and A. albopictus mosquitoes in the United States.
Myth: Zika virus is fatal in most infected people
Only 20% to 25% of individuals who become infected with Zika virus are symptomatic, and symptoms usually are mild. Clinical manifestations can occur 2 to 14 days after exposure and include fever with maculopapular rash, arthralgia, headache, and conjunctivitis. Because the Aedes mosquito also is a vector for dengue, whose symptoms resemble those of Zika, infected individuals should avoid nonsteroidal anti-inflammatory drugs to minimize the risk of dengue-associated hemorrhage.
Myth: No association exists between Zika virus and GBS
GBS is a disorder in which the innate immune system attacks parts of the peripheral nervous system. It is an ascending disorder: Initial symptoms include varying degrees of weakness or tingling sensations in the legs and symmetrical weakness; in many cases, abnormal sensations spread to the arms and upper body. These symptoms may increase in intensity until certain muscles cannot be used at all. In these critical cases, the disorder is life threatening, potentially interfering with respiration, blood pressure, or heart rate. However, most individuals have a good recovery even in the most severe cases, although some will continue to have some degree of weakness.
No one knows why GBS (which is not contagious) strikes some people and not others, or what sets the disease in motion. The syndrome is rare, afflicting only about one person in 100,000. Usually, GBS occurs a few days or weeks after the patient has had symptoms of a respiratory or GI viral infection. GBS likely is triggered by Zika in a small proportion of infections, much as it is after certain other infections.
WHO reports at least 13 countries or territories have documented an increase in GBS cases associated with Zika virus. At least six U.S. cases of GBS associated with Zika currently are being investigated.
Keeping abreast of the most current evidence-based guidelines on Zika and other emerging health crises is a hallmark of a true professional. The American Nurses Association supports registered nurses with up-to-date resources on its Zika information website.
Sharon Morgan is a senior policy advisor in Nursing Practice and Work Environment at ANA.
Selected references
Annenberg Public Policy Center of the University of Pennsylvania. More than 4 in 10 mistakenly think zika is fatal, symptoms are noticeable. March 10, 2016.
Augenbraun E. Zika virus hitches a ride with human-loving mosquitoes. Sci Am. February 1, 2016.
Centers for Disease Control and Prevention. Zika Virus. Updated May 20, 2016.
Harvard T.H. Chan School of Public Health. Many U.S. families considering pregnancy don’t know Zika facts. March 29, 2016.
Malteser International, Order of Malta Worldwide Relief. Dispelling Zika virus rumors with factual information. April 21, 2016.
National Institutes of Health, National Institute of Neurological Disorders and Stroke. Guillain-Barré syndrome fact sheet. Updated November 19, 2015.
World Health Organization. Zika virus. Fact sheet. Updated April 15, 2016.

















{kind=link}