
Experts weigh in on what nurses need to know
New evidence raises concerns about how nurses are preparing and administering I.V. push medications. A 2018 survey published by the Institute for Safe Medication Practices (ISMP) revealed that practitioners are frequently using unsafe practices.
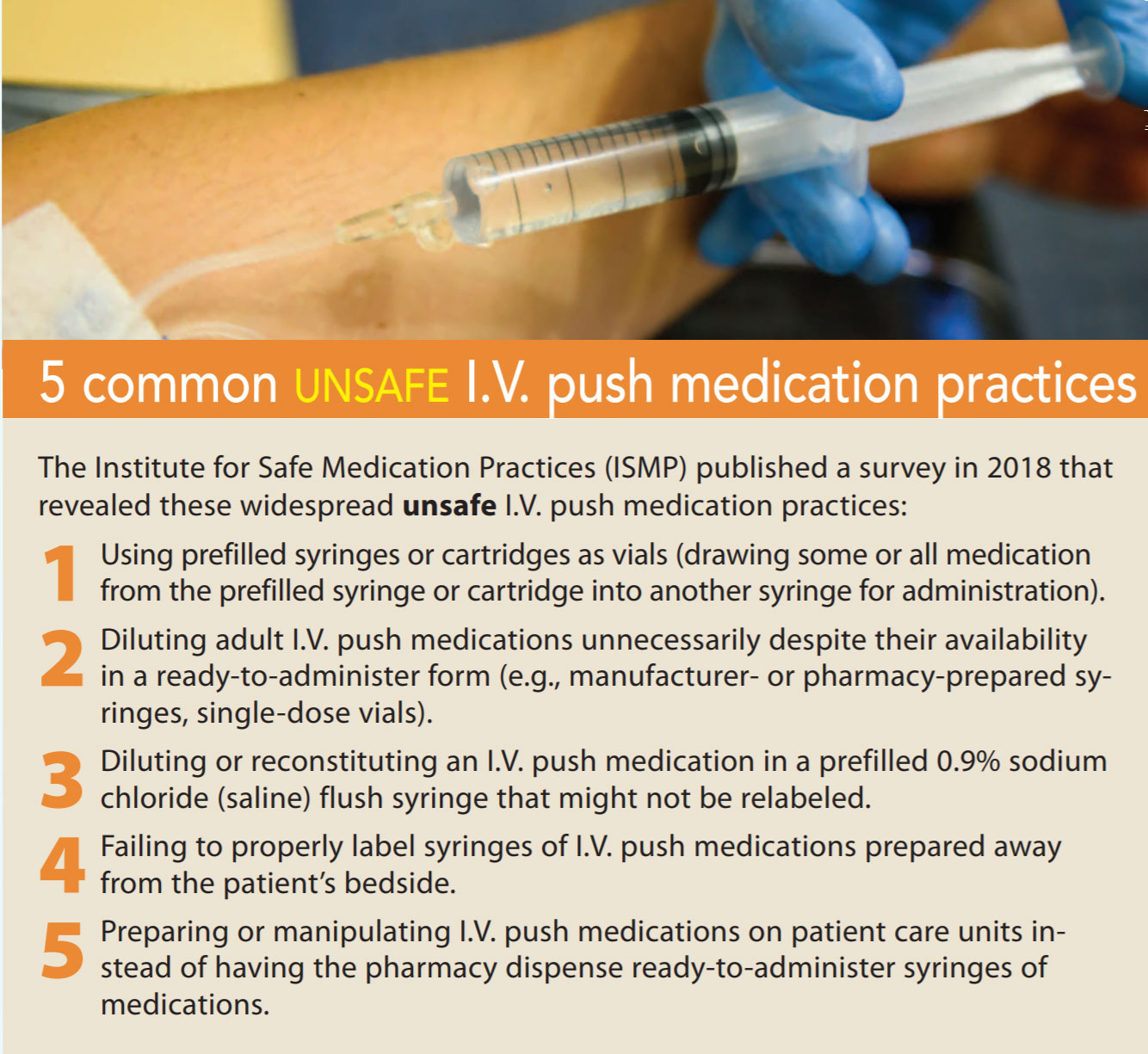
The 2018 survey is a follow-up to a similar ISMP survey published in 2014. The current survey reveals five major unsafe practices related to I.V. push medications that have persisted or worsened in the past decade. (See 5 common unsafe I.V. push medication practices.) Survey participants included 977 clinicians; 93% were nurses and 4% were advanced practice nurses.
To shed light on this challenging and multifaceted issue, American Nurse Today is presenting this special section, “I.V. Push Medication Administration,” which focuses on evidence-based practice. The section begins with an overview of the problem from three clinical experts’ perspectives, followed by articles on dilution and the myths of I.V. push administration. It concludes with a checklist of key recommendations that nurses can use to ensure they’re practicing based on the latest evidence.
We asked three clinicians to share their expertise and insight into the issue of I.V. push medication administration:
 | Elizabeth Campbell, MSN, RN, CRNI, is past-president of the Infusion Nurses Society New England Chapter and a clinical scholar at Massachusetts General Hospital in Boston. |
 | Steven Jarrett, PharmD, is the medication safety officer in the quality division for Atrium Health in Charlotte, North Carolina. |
 | Susan Paparella, MSN, RN, is vice president of the Institute for Safe Medication Practices. |
Q: What are the concerns about the major findings of the survey?
Paparella: In 2015, ISMP published the ISMP Safe Practice Guidelines for Adult I.V. Push Medications. Despite this, the 2018 survey found wide variations in practice and at-risk behaviors. For example, 66% of survey participants reported using prefilled syringes as vials. This involves drawing medication from a manufacturer-prepared, ready-to-administer syringe into another syringe. This practice increases the risks of contamination and dosage alteration. These products are developed to promote safety, and if you manipulate them, you’re negating that.
Campbell: Nurses have been trained about the importance of following the five rights of medication administration: the right medication, patient, dose, route, and time. However, the results of this survey show a rise in unsafe I.V. medication practices that fall outside the five rights. The five rights alone aren’t going to keep patients safe. It’s just as important to administer medications in the right form prepared in the right way. Otherwise, you put patients at risk for complications, such as infections, reactions, interactions, and medication errors. I.V. therapy can cause many injuries and complications and is heavily litigated.
Jarrett: The elephant in the room is that many nurses aren’t following evidence-based practice. Rather than using pharmacy dispensed ready-to-administer, manufacturer-prepared medication syringes, survey participants report that they’re frequently preparing or manipulating I.V. push medications on patient care units. This practice increases the risk of contamination from bacteria, particulates, and other impurities. Only 50% of participants say they always label self-prepared I.V. push medications. Another safety issue is the unnecessary dilution of I.V. push medications. Many nurses also are diluting or reconstituting medications using a prefilled 0.9% sodium chloride (saline) flush syringe, which is an unsafe practice. (For more information about dilution, see page 22.)
Q: Why is there a discrepancy between evidence-based practice and what nurses are doing?
Paparella: Nurses don’t always have clear direction and policies about diluting and administering I.V. push medications. They may have conflicting references, learn incorrect information from coworkers, or make up their own methods. They may drift into unsafe behaviors because they don’t perceive the risk or believe that the risk is justified.
Campbell: Although nearly every patient admitted to the hospital today has an I.V., insufficient education about I.V.s and infusion therapy is provided in nursing schools. In addition, when hospital budgets get tight, specialized I.V. teams may be cut. This can lead to higher rates of I.V.-related complications because of the gap in skill and knowledge between specialist infusion nurses and other nurses.
Jarrett: Everyone develops their practice based on their experience, what they were taught, preconceived notions, and what they think is the right thing to do. If nurses aren’t aware of any complications, they may feel comfortable continuing unsafe practices.
Another issue is the intermittent shortages of 100 mL bags of 0.9% normal saline and D5W [5% dextrose in water]. Shortages create confusion about administration because nurses must give some medications I.V. push that they were accustomed to administering via I.V. piggyback.
Q: How can organizations change unsafe behaviors?
Campbell: The infusion world changes quickly with new products, standards, discoveries, and drug shortages. The best thing for patients is to have a dedicated I.V. team of experts who are up-to-date on best practices. Education also needs to go beyond a facility’s I.V. team. Every unit should have an educated I.V. champion who helps ensure all nurses know best practices.
In addition, all incidents of medication infiltration should be documented, and managers should hold monthly staff meetings to discuss issues that have occurred and how to prevent them with safe practices.
Paparella: Effecting change is a multilayered process that includes creating awareness, providing the right products, ensuring that managers understand practice guidelines, and educating nurses about best practices.
ISMP guidelines state that facilities should provide I.V. push medications in a ready-to-use form as often as possible. This highest-level strategy practice limits the possibility of error. Another tactic is to create easy-to-reference tables that identify the most commonly given I.V. push medications, how to administer them, and how to dilute them, if necessary. Organizations also can use the free ISMP Gap Analysis Tool to evaluate their I.V. push medication practices. (See Resources.)
Jarrett: Nurses have valid concerns that explain why they do what they do. Listening to their concerns is important to understand why unsafe practices occur in your setting. Then present evidence-based standards and the reasons nurses need to follow them. Once you get the evidence out there, nurses will respond.
Catherine Spader is an author and healthcare writer based in Littleton, Colorado. Note: Campbell and Jarrett are members of the Fresenius-Kabi Advisory Board
Resources
Access these resources to learn more about safe I.V. medication administration practices.
Infusion Nurses Society infusion therapy standards of practice: ins1.org/Default.aspx?TabID=251&productId=113266
Institute for Safe Medication Practices (ISMP) safe practice guidelines for adult I.V. push medication: ismp.org/guidelines/IV-push
ISMP gap analysis tool for safe I.V. push medication practices: ismp.org/resources/gap-analysis-tool-safe-IV-push-medication-practices

















1 Comment.
Thank you for sharing this. As a nurse educator we are having discussions on how to help students prepare better for medication safety best practices. As a patient I had a new grad almost kill me with an undiluted IV push med she slammed in my IV (which should have been diluted and a slow push). The problem is not always over-dilution. Good discussion.