Follow the evidence for best practice.
- Positive urine cultures among older patients living in long-term care facilities frequently lead to antibiotic prescriptions because of an association between urinary tract infections and falls, confusion, anxiety, and agitation.
- Without relevant clinical symptoms, a positive culture typically indicates asymptomatic bacteriuria, which doesn’t require antibiotic treatment.
- As the clinicians most likely to first detect changes in a patient, nurses play a significant role in curbing the unnecessary use of antibiotics.
Antibiotic stewardship has gained much awareness, but inappropriate prescribing of these medications continues. For example, many patients, caregivers, and clinicians associate urinary tract infection (UTI) with falls, confusion, anxiety, and agitation among older patients, especially those living in long-term care (LTC) facilities. As a result, positive urine cultures frequently lead to an antibiotic prescription. However, a positive urine culture doesn’t necessarily require antibiotic treatment. Without relevant clinical symptoms, a positive culture typically indicates asymptomatic bacteriuria (ASB). (See ASB defined.)
As described by Nicolle and colleagues, the Infectious Diseases Society of America clinical practice guideline for managing ASB doesn’t recommend screening for the condition in older patients living in LTC facilities; screening may benefit only specific populations, such as pregnant women and those undergoing certain urologic procedures. As a result, providers working in these facilities frequently face the challenge of appropriate UTI identification and management, adherence to evidence-based guidelines, and antibiotic stewardship.
Asymptomatic bacteriuria (ASB) refers to significant bacteria (one or more species) in the urine without symptoms of active infection. More specifically, it’s defined as a bacterial count of ≥100,000 colony-forming units per milliliter (CFU/mL) in the urine of a patient without signs and symptoms of urinary tract infection (UTI).
In men who aren’t catheterized, one specimen yielding at least 100,000 CFU/mL of an organism indicate ASB. In women who don’t have a catheter, the threshold is two consecutive voided specimens yielding at least 100,000 CFU/mL. In patients with a catheter who don’t have UTI symptoms, one specimen that yields 100,000 CFU/mL meets the definition of ASB.
ASB incidence
The incidence of ASB, which is uncommon in younger adults, increases with age. Changes in the genitourinary tract secondary to aging combined with comorbid conditions create a predisposition for developing bacteriuria. For example, bowel and bladder incontinence, which may be present in older patients living in LTC facilities who also have stroke or dementia, is associated with ASB and symptomatic UTI. Residents with prostate enlargement accompanied with urine flow limitations and incomplete bladder emptying also have a higher prevalence of ASB. Benton and colleagues report that rates of ASB in LTC facilities can reach 25% to 50% in women and 15% to 40% in men. However, in residents with urinary catheters, this number reaches almost 100%.
Although guidelines advise against antibiotic treatment of ASB, providers in LTC facilities frequently prescribe antibiotics for older residents who don’t meet the minimum criteria for UTI. A UTI diagnosis requires the presence of positive urinalysis and urine culture findings and genitourinary tract symptoms (for example, dysuria, hematuria, suprapubic pain, costovertebral angle tenderness, and abdominal pain).
Unnecessary urine testing
Unnecessary and excessive urine testing may play a role in antibiotic overuse in patients living in LTC facilities. The presence of cloudy or foul-smelling urine frequently leads to urinalysis and culture, which results in antibiotic treatment for UTI. However, cloudy or foul-smelling urine also occurs with noninfectious causes, such as ASB or dehydration.
Concern about falls also may prompt urine testing in LTC facilities. However, in the absence of clinical symptoms, clinicians must evaluate the many other reasons for falls in this population, including comorbid conditions such as Parkinson’s disease and dementia, gait and balance impairments, medications, dehydration, poor vision, and environmental hazards. In cognitively impaired patients with ASB who experience a fall, the current guidelines recommend observation over treatment. Although mental status changes, lethargy, and fever also may be present in urinary infections, they’re not specific to UTI.
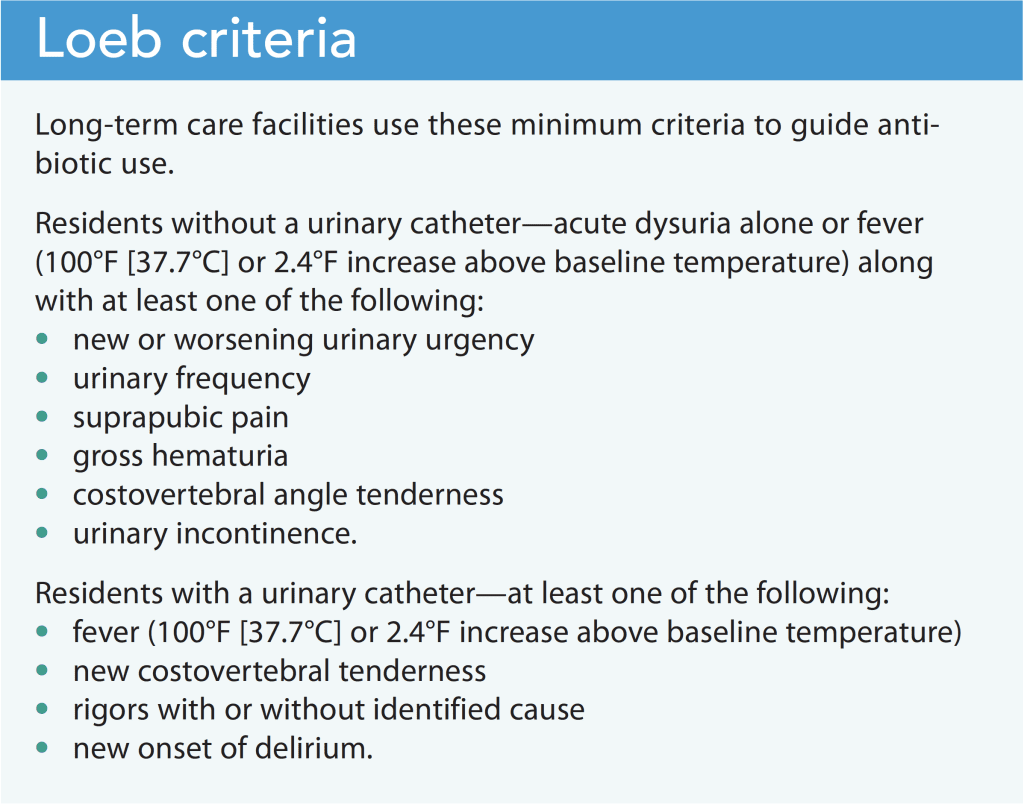
Sloane and colleagues studied the practice of urine testing and treatment of ASB in 31 community nursing homes in North Carolina. They observed that urine cultures led to antibiotic use 89% of the time for colony counts of ≥100,000 CFU/mL. However, no significant difference was found between those treated and those untreated in terms of temperature, frequency of urinary tract symptoms, or antibiotic initiation using Loeb criteria (a minimum set of criteria that provides guidance for initiating antibiotics in LTC facilities). (See Loeb criteria.)
Consequences of antibiotic overuse
Antibiotic overuse can lead to adverse drug reactions, drug–drug interactions, development of resistant organisms, and infections caused by overgrowth of organisms such as Clostridioides difficile. Treatment costs also should be contemplated.
Drug-to-drug interactions are a serious consideration since many elderly residents of LTC facilities have multiple underlying medical conditions, which can result in polypharmacy. Polypharmacy contributes to poorer outcomes for older patients and exposes them to additional interactions with each new medication.
Elderly residents also are prone to the adverse effects of the antibiotics themselves, including diarrhea, which may lead to dehydration and electrolyte abnormalities. Many elderly patients have one or more drug allergies, so adding new medications puts them at increased risk for an allergic reaction.
In addition, erroneous diagnosis of UTI impedes proper identification and treatment of the actual underlying condition.
Diagnostic challenges
Distinguishing between UTI and ASB presents challenges in the LTC setting. Many older patients with conditions such as advanced dementia may not be able to communicate the presence of localized genitourinary symptoms. Mental status changes frequently are associated with the presence of infection in older patients; however, in those with advanced dementia, this is a nonspecific symptom since they already experience significant cognitive deficits.
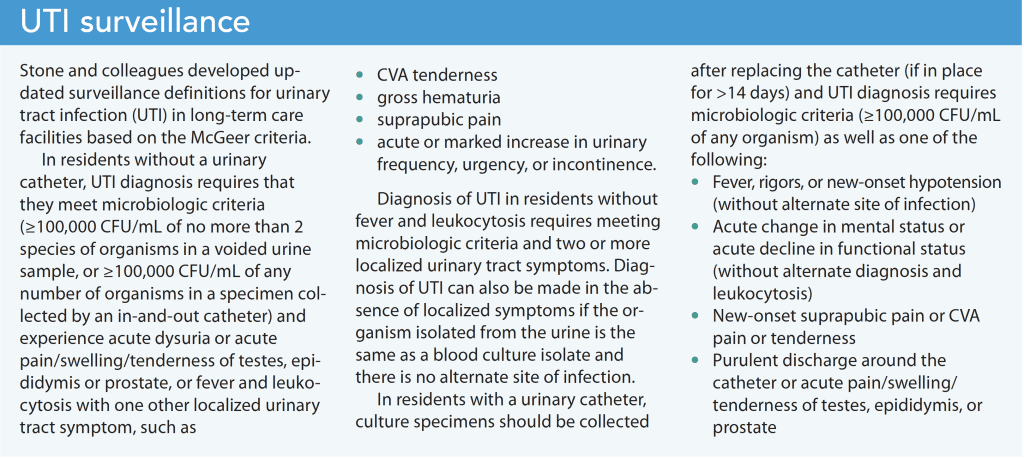
Genitourinary tract symptoms warrant workup for infection and can help guide treatment. It’s also reasonable to initiate broad-spectrum antibiotics in older adults with bacteriuria who have a fever and other signs of sepsis. McGeer criteria (originally issued in 1991 and then revised) have been widely accepted in LTC settings as a standard for surveillance and diagnosis. They also have proven beneficial in ASB management. (See UTI surveillance.)
Nursing implications
Frequently, nurses are the first clinicians to detect changes in a patient, so they can play a significant role in curbing the unnecessary use of antibiotics. Carefully observe patients with functional or cognitive impairment. Perform medication reconciliation to determine if the changes you observe may be the result of new or recent medication modifications, assess vital signs, monitor fluid status, and note any alterations in the patient’s environment or stimuli that may contribute to cognitive impairment.
Familiarize yourself with evidence-based protocols for UTI and ASB and learn about interventions to manage ASB. To reduce the risk of UTI in patients with ASB, encourage fluid intake, provide perineal cleansing, and promote a toileting schedule. For those with a urinary catheter, follow proper care protocols.
If the provider does prescribe antibiotics to treat UTI, closely monitor patients for drug interactions.
Promote best practices
Many patients treated for UTI don’t actually meet the criteria established in most LTC settings. Studies indicate that antibiotic treatment doesn’t reduce morbidity and mortality. Prudent assessment of clinical UTI symptoms, specifically genitourinary tract symptoms, in elderly residents of LTC facilities can help decrease the rate of antibiotic use. Treating patients with antimicrobial therapy requires that providers ensure residents meet the minimum criteria for infection. When clinicians follow evidence-based practice, they not only help curb unnecessary antibiotic use in LTC facilities, they also establish accurate diagnoses, prevent patient harm, and promote best practices and outcomes.
Shantha Franks is an assistant professor of nursing at Ramapo College of New Jersey in Mahwah and an adult and gerontologic nurse practitioner at Cedar Medical in Oradell, New Jersey.
References
Benton TJ, Young RB, Leeper SC. Asymptomatic bacteriuria in the nursing home. Ann Longterm Care. 2006;14(7):17-22. hmpgloballearningnetwork.com/site/altc/article/5963
Datta A, Datta R, Elkins J. What factors predict falls in older adults living in nursing homes: A pilot study. J Funct Morphol Kinesiol. 2018;4(1):3. doi:10.3390/jfmk4010003
Gupta K, O’Brien W, Gallegos-Salazar J, Strymish J, Branch-Elliman W. How testing drives treatment in asymptomatic patients: Level of pyuria directly predicts probability of antimicrobial prescribing. Clin Infect Dis. 2020;71(3):614-21. doi:10.1093/cid/ciz861
Loeb M, Bentley DW, Bradley S, et al. Development of minimum criteria for the initiation of antibiotics in residents of long-term-care facilities: Results of a consensus conference. Infect Control Hosp Epidemiol. 2001;22(2):120-4. doi:10.1086/501875
McGeer A, Campbell B, Emori TG, et al. Definitions of infection for surveillance in long-term care facilities. Am J Infect Control. 1991;19(1):1-7. doi:10.1016/0196-6553(91)90154-5
Nicolle LE. Urinary tract infections in the older adult. Clin Geriatr Med. 2016;32(3):523-38. doi:10.1016/j.cger.2016.03.002
Nicolle LE, Gupta K, Bradley SF, et al. Clinical Practice Guideline for the Management of Asymptomatic Bacteriuria: 2019 Update by the Infectious Diseases Society of America. Clin Infect Dis. 2019;68(10):e83-110. doi:10.1093/cid/ciy1121
Sloane PD, Kistler CE, Reed D, Weber DJ, Ward K, Zimmerman S. Urine culture testing in community nursing homes: Gateway to antibiotic overprescribing. Infect Control Hosp Epidemiol. 2017;38(5):524-31. doi:10.1017/ice.2016.326
Stone ND, Ashraf MS, Calder J, et al. Surveillance definitions of infections in long-term care facilities: Revisiting the McGeer criteria. Infect Control Hosp Epidemiol. 2012;33(10):965-77. doi:10.1086/667743
Key words: bacteriuria, asymptomatic bacteriuria, urinary tract infection, UTI, long-term care facilities, geriatric patients, elderly patients


















1 Comment. Leave new
I had the pleasure of having Dr. Franks as a Professor at William Paterson Univ and clinical preceptor. She is an amazing provider and I had the opportunity to use the article as a guide and reference now that I am a clinician.