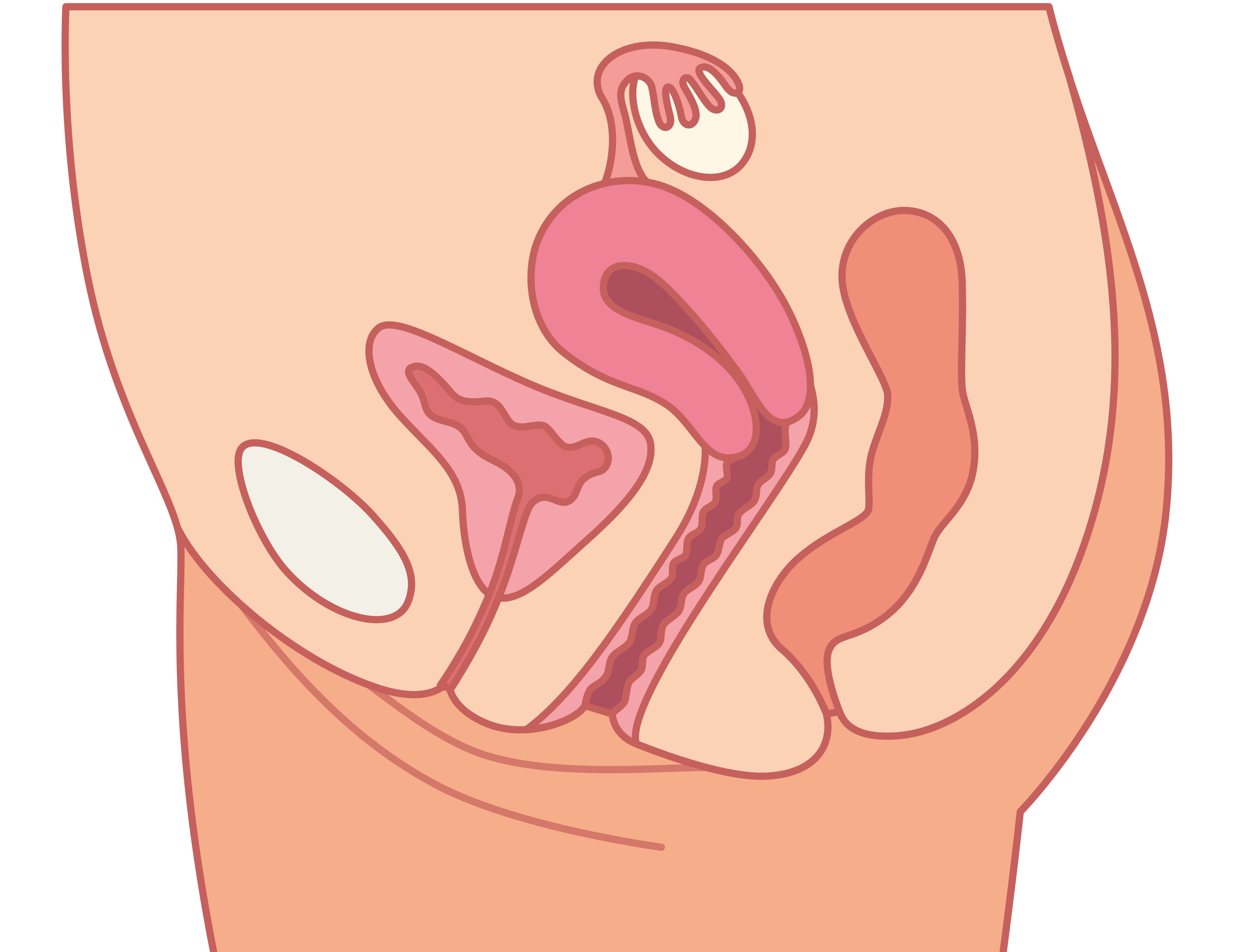
Pelvic organ prolapse (POP) is the protrusion of the pelvic organs against the vaginal walls towards or through the vaginal opening. The number of women suffering with POP is difficult to determine, but reports indicate that symptoms affect up to 50% of females as they age.
Despite the fact that direct costs related to surgical procedures to alleviate symptoms are reported to be over $1 billion annually, POP is often referred to as a silent disease. Many women never seek treatment, viewing their symptoms as a normal part of aging and something they have to “put up with.” Their reluctance to address the issue also may be fueled by a lack of information and the fear that surgery is the only treatment option available, which is far from accurate. Although surgical interventions do benefit many women, nearly one-third of those who do have surgery will experience a recurrence of their symptoms within 5 years. These failure rates are significant enough to highlight the need for more practical and user-friendly nonsurgical options.
Healthcare providers, especially nurses, are well placed to identify and break down the physical and emotional barriers that impede the proper screening, diagnosis, and treatment of this common condition.
Barriers to getting help
Ramifications of POP are not life-threatening but can be significantly life-altering. Though the number of women experiencing these discomforts is widespread, there is often reluctance to discuss this awkward topic. The fear of incontinence or the sensation of something “coming down” may cause women to avoid social activity and exercise, both of which can have a negative impact on overall health.
Sexual dysfunction and changes in body image are often associated with prolapse. For some women, intercourse can be painful or the belief that their anatomy is “abnormal” may make them too embarrassed or ashamed to have sex. Women also may fear that sexual activity will cause harm to the organs involved in the prolapse.
All women should be screened, and if experiencing symptoms, offered earlier and less aggressive treatment. Conservative treatments can control, improve, and even eliminate symptoms related to POP. Given that the risks to patients are few, conservative measures should be the first line of treatment offered to women experiencing symptoms. Nurses have a critical role in the initial assessment, management, and ongoing support of women with POP.
Signs and symptoms
POP occurs when the muscles and ligaments supporting the pelvic organs stretch or weaken, causing organs to slip out of place. Prolapse can involve any pelvic organ, but most commonly involves the bladder. Symptoms associated with prolapse can include backache, pelvic pressure, vaginal bulge, or as described by many women as a feeling that something “is coming down” or “falling out.” Bladder, bowel, and sexual dysfunction are also associated with prolapse, with urinary incontinence (UI) the most common complaint. (See Signs and symptoms of pelvic organ prolapse.)
Signs and symptoms of pelvice organ prolapse
|
The International Continence Society identifies several types of UI: urgency urinary incontinence (UUI), loss of urine associated with urgency; stress UI (SUI), loss of urine on effort or physical exertion, such as sneezing or coughing; and mixed UI (MUI), loss of urine associated with urgency and exertion.
UI is not just bothersome; it’s a condition that negatively affects multiple aspects of a woman’s health as well as her quality of life.
Diagnosis
The questions nurses can ask to assess the presence of prolapse are simple and include: “Do you feel a bulge or something coming out of your vagina?” and “Do you feel like something is coming down or falling out of your vagina?” An easy and quick tool nurses can use to screen for symptoms of incontinence is the 3 Incontinence Questions questionnaire (3IQ), which can help in distinguishing urge from stress incontinence.
The 3 Incontinence Questions Questionnaire (3IQ)
Source: Horng M. Diagnosing urinary incontinence with 3 simple questions. J Clin Outcomes Manage. 2006;13(7):364-5. |
While doing a pelvic exam, the clinician can ask the patient to bear down and/or cough to observe for signs of prolapse and urine leakage. While performing a bimanual exam, the patient can be asked to contract the pelvic muscles and perform a Kegel exercise, and the clinician can assess muscle tone and also teach correct performance of the exercise.
Treatment
Treatment options for pelvic organ prolapse include lifestyle changes, pelvic floor muscle training, vaginal pessaries, and surgical correction. The risks of complications and the long-term risk of recurrence make undergoing surgery undesirable for many women. For older women with significant comorbidities, surgery may not be an option.
Management of pelvic organ prolapse depends on the woman’s individual motivation. For example, if the prolapse or stress incontinence is not very bothersome to her, clinical observation or watchful waiting with lifestyle changes is an appropriate treatment approach.
Lifestyle changes
The prevalence of incontinence and prolapse increases with age and number of pregnancies and deliveries a woman has experienced, but other factors also influence the severity of symptoms. The chance of developing POP is 50% higher in overweight and obese women. Constipation, smoking (which leads to chronic coughing), heavy lifting, and high impact exercise also are associated with pelvic organ prolapse.
Women being counseled about treatment options should be instructed on lifestyle modifications that will reduce intra-abdominal stress and ease the downward pressure on the prolapsed area:
- Lose weight as indicated.
- Stop smoking.
- Avoid constipation and straining by changing diet.
- Avoid heavy lifting.
- Avoid high-impact exercise; instead, switch to low- or no-impact exercise such as swimming.
To control urinary symptoms, women should be counseled to void at regular, timed intervals and to avoid bladder irritants such as caffeine, carbonated beverages, and alcohol.
Pelvic floor muscle training
A recent Cochrane review concluded that pelvic floor muscle training was effective and should be considered as the first-line management of any type of urinary incontinence. Teaching a patient how to perform these exercises can be as simple as giving brief instructions in the office accompanied by a handout with guidelines and illustrations. For some women, referring to websites with appropriate information and on-line instructions can be helpful.
Some women may require more intensive instruction and need to work with a physical therapist (PT) who specializes in pelvic floor disorders and can assess if biofeedback or electrical stimulation of pelvic floor muscles is indicated. Resources for finding a PT with expertise in this area include:
Many women who receive pelvic floor physical therapy report significant improvement in their symptoms after an average of 8 to 12 treatments.
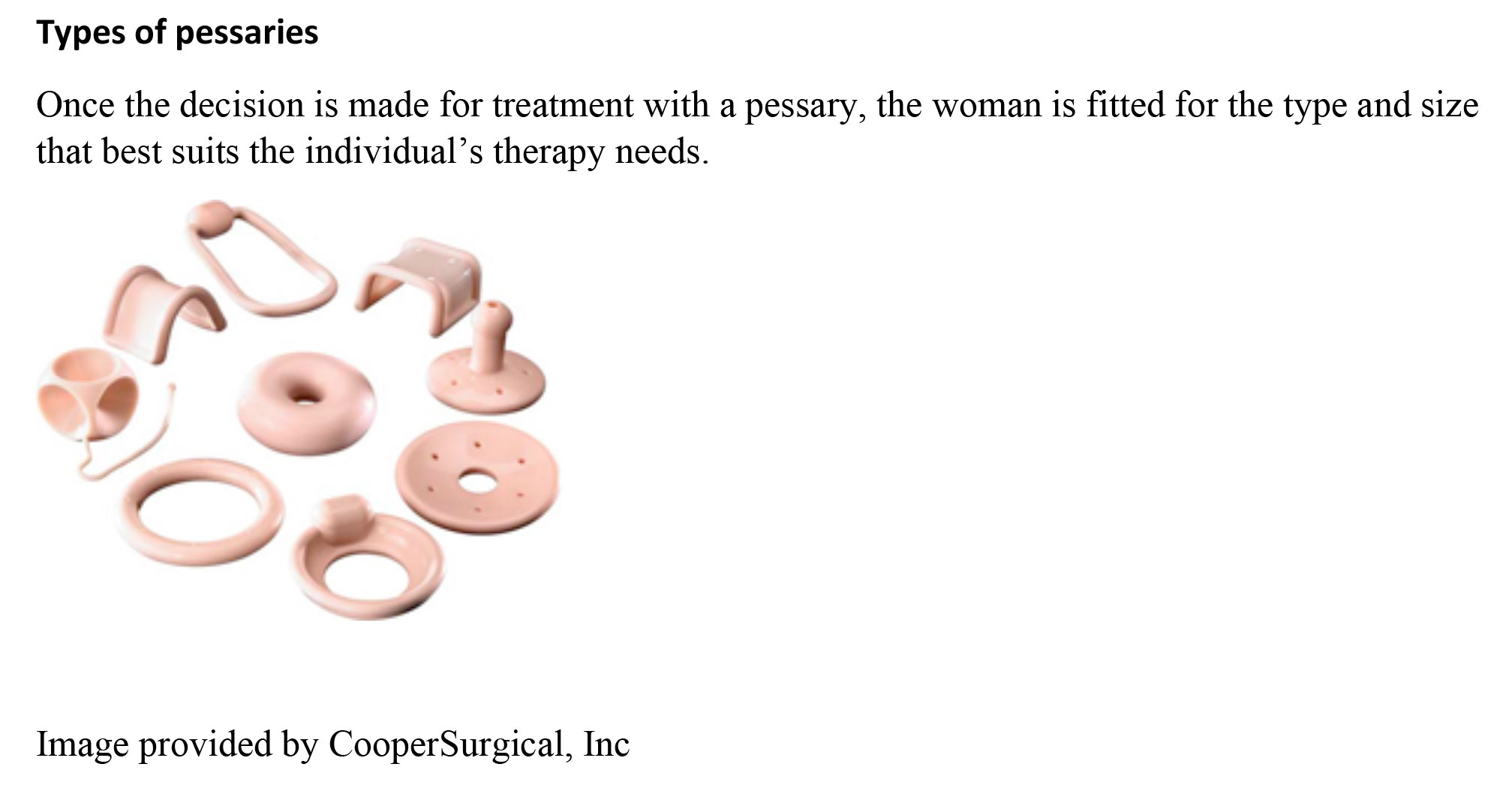
Pessaries
Pessaries are a mainstay of conservative treatment for women who experience bothersome symptoms of POP. Though they have been used for thousands of years and in many forms, the trend toward conservative treatment has caused a resurgence in their popularity. Pessaries are flexible, non-allergenic, odor repellant devices that come in many shapes and multiple sizes. (See Types of pessaries.)
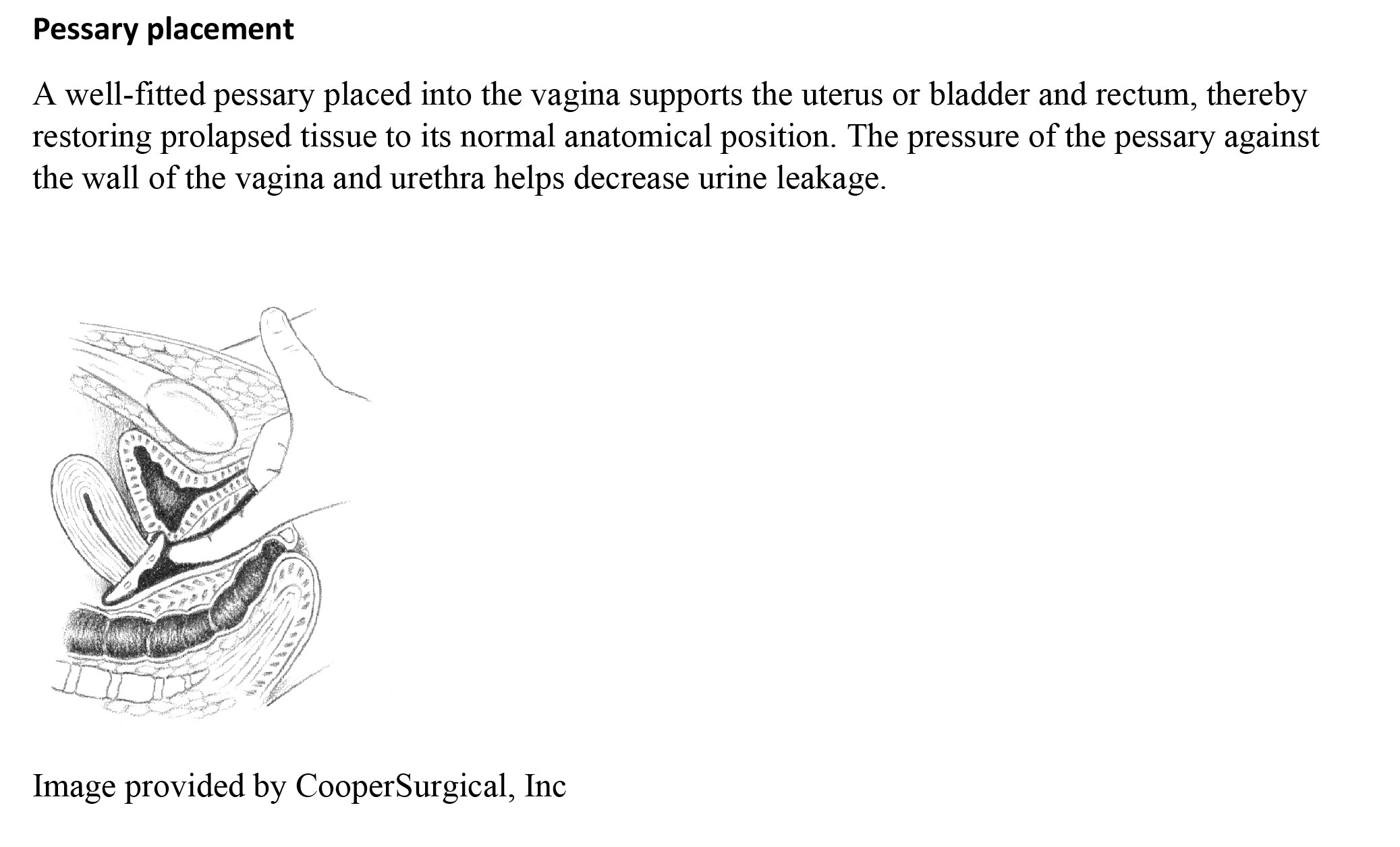
Women can be easily fitted with an appropriate pessary in an office visit, and have immediate relief of symptoms. (See Pessary placement.) After 1 year, satisfaction levels between women using pessaries and those who chose surgical intervention, was found to be similar in regards to urinary issues and sexual function.
A woman who is sexually active needs to be able to remove and replace the pessary comfortably. Women who don’t need to or are unable to remove the device on a regular basis need to schedule routine maintenance visits to their healthcare provider, at least within 3 to 4 month intervals, so that the pessary can be removed, cleaned, and reinserted after the vaginal tissue has been assessed. One of the risks of long-term pessary use without maintenance care is erosion of tissue from constant pressure of the pessary on vaginal wall tissue, which in a worst-case scenario can lead to development of a fistula.
Improving women’s lives
POP is common and costly, both in terms of health care dollars and the negative impact it can have on a woman’s quality of life. Nurses working in primary care are in a perfect position to increase awareness so that women recognize symptoms when they first occur. Once screening for symptoms becomes part of the routine health physical exam, prolapse will become readily diagnosed and women can benefit from conservative treatment. Ongoing support provided by nurses is critical in the long-term success of conservative treatment for POP and can lead to patients living more productive, less encumbered lives.
Ann E. Feeney is an assistant professor in the department of nursing at the University of Scranton in Scranton, Pennsylvania, and a nurse midwife and nurse practitioner in women’s health at Geisinger Tunkhannock in Tunkhannock, Pennsylvania.
Selected references
Awwad J, Sayegh R, Yeretzian J, et al. Prevalence, risk factors, and predictors of pelvic organ prolapse: a community-based study. Menopause. 2012:19(11):1235-41.
Coyne KS, Wein A, Nicholson S, et al. Comorbidities and personal burden of urgency urinary incontinence: a systematic review. Int J Clin Pract. 2013;67(10):1015-33.
Dumoulin C, Hay-Smith EJC, Mac Habée-Séguin G. Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women. Cochrane Database Syst Rev. 2014;5:CD005654.
Lewthwaite B, Staley D, Girouard L, et al. Characteristics of women with continued use of vaginal pessaries. Urol Nurs. 2013;33(4):171-7
Nygaard I, Brubaker L, Meikle S, et al. Long-term outcomes following abdominal sacrocolpopexy for pelvic organ prolapse. JAMA. 2013;309(19):2016-24.
Overby Z, Persons R, Carrillo M. Clinical inquiries: What is the best nonsurgical therapy for pelvic organ prolapse? J F Pract. 2014;63(8):471-9.
Richardson K, Hagen S, Glazener C, et al. The role of nurses in the management of women with pelvic organ prolapse. Br J Nurs. 2009;18(5):294-300.
Smith TA, Poteat TA, Shobeiri SA. Pelvic organ prolapse: an overview. JAAPA. 2014;27(3):20-4.














{kind=link}
{kind=link}
1 Comment.
I found it interesting that you state that symptoms can be overlooked, increasing the importance of a checkup. My wife has been looking for ways to prevent diseases so she can stay healthy for as long as possible. I will send her this information so she can look into getting a pelvic examination to check for abnormalities.