
Use mnemonics to aid remembering and identifying abnormal findings.
Takeaways
- Many nurses find remembering the cranial nerves and their functions to be challenging.
- Neurologic assessments occur in all healthcare settings.
- Understanding normal and abnormal cranial nerve assessments can aid early diagnosis and treatment.
Acute and chronic neurologic presentations exist in all healthcare settings. Abnormal findings—subtle or gross—reflect sensory, motor, and reflexive function and have significant implications for nursing care. However, many nurses may find cranial nerve assessment challenging if they don’t perform it routinely. Mnemonics can aid assessment recollection and recognition of abnormal findings.
Cranial nerves
The 12 pairs of cranial nerves are referred to by Roman numerals (CN I through XII) or by name. The cranial nerves control most of the sensory and motor function in the head and neck in addition to peripheral nerves that exit from the midbrain or the brainstem. Each cranial nerve has either a sensory, motor, or a combined function.
Assessing and managing patients with chronic subdural hematoma
Evaluating the neurologic status of unconscious patients
Cranial nerve assessments help you determine cerebral cortex and brainstem function depending on the patient’s level of consciousness (LOC). A fully awake and aware patient can follow commands that permit bilateral assessment of all 12 cranial nerves. A patient with a decreased LOC will have limited participation in a full assessment. Regardless of LOC and cognition, the following cranial nerves usually can be assessed:
- CN III: Oculomotor (pupillary reflex)
- CN V: Trigeminal (corneal reflex)
- CN IX: Glossopharyngeal (gag reflex)
- CN XII: Hypoglossal (cough reflex)
In conscious patients, LOC changes provide the earliest indicator of neurologic compromise. In unconscious patients, pupillary light reflex response is the most sensitive indicator unless the patient had previous eye surgery or has pre-existing eye trauma. These changes don’t occur in isolation. They reflect a possible neurologic emergency that requires immediate intervention.
Mnemonics
Several mnemonics have been created to help nurses remember the name and function of the 12 cranial nerves. However, the most important component of a cranial nerve assessment is knowing normal vs. abnormal. Other creative tools for aiding cranial nerve recall include a University of Texas Southwestern Neurology YouTube video and a visual developed by Bolek.
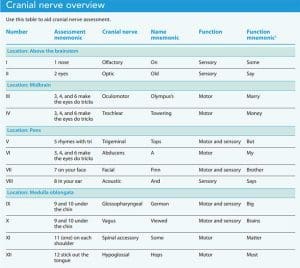
Remembering all 12 cranial nerve types and their functions can be overwhelming, so we recommend connecting each cranial nerve with a basic function. To connect the cranial nerve numbers with their names, use the saying “On old Olympus’s towering top a Finn and German viewed some hops.” The first letter of each word represents a cranial nerve beginning with the same letter. For example, “On” is the first word in the mnemonic and CN I is olfactory. Cranial nerves also can be remembered based on their function: sensory (S), such as smell (CN I) or vision (CN II), and motor (M), such as moving the eyes laterally toward the ear (CN VI) or sticking out the tongue (CN XII). Some cranial nerves have both sensory and motor function (B). For example, CN VII affects taste and the corneal response as well as upper and lower facial movement. (See Cranial nerve overview.)
Cranial nerve I (olfactory)
Mnemonic: 1 nose
Description: This sensory nerve detects odor and transmits smell.
Assessment and findings: Ask the patient to close their eyes and identify nontoxic smells under each nare. Impairment can be related to non-neurologic causes (smoking, nasal congestion, aging) or neurologic causes (trauma, Alzheimer’s disease, or Parkinson’s disease).
Care implications: Testing of this cranial nerve frequently is deferred in the acute settings.
Cranial nerve II (optic)
Mnemonic: 2 eyes
Description: This sensory nerve involves vision.
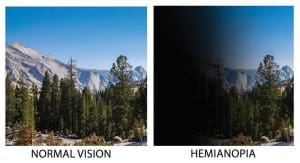
Assessment and findings: Testing is done with a Snellen chart or by having the patient read printed material or count fingers. Visual fields are evaluated with confrontation testing. Face the patient and ask them to cover one eye while you cover your eye on the same side. The patient looks straight ahead while you wiggle your fingers, moving them from the outside edge of the six cardinal visual fields to the center. If the patient can’t see the fingers, they may have a visual field cut (hemianopsia).
Care implications: Hemianopsia is visual loss that impairs half of the visual field in one or both eyes. Depending on the injury location, several visual field deficits may exist that jeopardize safety. Environmental modifications are required. [See figure 1.]
Cranial nerve III (oculomotor)
Mnemonic: 3, 4, and 6 make the eyes do tricks
Description: The oculomotor nerve has three motor functions: eyelid elevation, pupillary light reflex or constriction to light, and extra-oculomotor movement (EOM).
Assessments and findings:
Elevating the eyelid. An easy way to remember the first motor function is to imagine a Roman numeral III, or a “pillar” elevating the eyelid. Ptosis (droopy eyelid) may result if the nerve is impaired.
Care implications: Ptosis can be unilateral or bilateral and caused by underlying nerve compression, trauma, or pathology.
Pupillary light reflex. A flashlight typically is used to assess a pupil’s constrictive ability. To eliminate subjectivity and doubt, consider using a quantitative pupillometry device to objectively measure the pupillary light reflex. Response documentation should include the bilateral pupil size (mm), shape, and briskness of response when light is shone into the eye (direct) or opposite eye (consensual). When pupils are dilated, unequal, sluggish or nonreactive to light (fixed), or don’t respond, further assessment is required. Pre-existing conditions that may affect the pupillary response include a history of cataract surgery or eye trauma (no response); use of opioids, benzodiazepines, or heroin (constriction, sometimes pinpoint); or use of mydriatics (atropine), alcohol, marijuana, cocaine, and hallucinogens (dilation).
Care implications: Ipsilateral (occurring on same side as the injury) pupillary dilation can indicate rising intracranial pressure mandating immediate attention.
Extraocular movements. The third function of CN III works in conjunction with CN IV (trochlear) and VI (abducens) to perform EOM. Instruct the patient to follow your finger with their eyes as you move it in an “H” or “N” pattern. This will highlight abnormalities or nerve palsies in these nerves. Normal eye movements include the ability to move them upward nasally and temporally, and downward symmetrically. [See figure 2.]
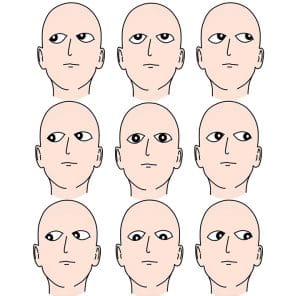
Care implications: Ideally, both eyes remain aligned and move in the same direction and at the same speed (conjugate). At rest, a disconjugate gaze indicates EOM compromise. Consider EOM compromise if the patient can’t follow commands but can follow or “track” movement around the room. EOM can’t be assessed in a patient who’s comatose, but oculocephalic (doll’s eyes) testing can be performed and providers may use oculovestibular (cold caloric) testing to determine if brain death has occurred.
Cranial nerve IV (trochlear)
Mnemonic: 3, 4, and 6 make the eyes do tricks
Description: The trochlear nerve moves the eyes nasally inward and down.
Assessment and findings: CN IV impairment can result in double vision (diplopia) and involuntary eye movement (nystagmus).
Care implications: Patients may experience increased fall risk, impaired mobility, headaches, and nausea.
Cranial nerve V (trigeminal)
Mnemonic: 5 rhymes with tri
Description: The trigeminal nerve has three bilateral branches: forehead (V1), cheeks (V2), and jaw (V3). It has both motor (teeth clenching) and sensory (sharp/dull discrimination, temperature, light touch) functions.
Assessment and findings: To assess the motor component of CN V, observe the strength and symmetry of movement when the patient clenches their teeth. To assess the sensory component, instruct the patient to close their eyes, and with a cotton swab lightly touch each of the three bilateral distributions of the nerve. CN V and VII (facial nerve) contribute to the corneal reflex response. Touching the cornea with a sterile wisp of cotton or drop of saline provides the sensation needed to stimulate the expected motor response (brisk blink). Assess both sides for symmetry.
Care implications: A normal assessment finding includes intact sensation and motor function in all three areas. Masseter and temporal muscle weakness and unequal or absent sensation in the forehead, cheek, or jaw can occur individually or bilaterally. Impacted chewing sensation and function increases the risk of aspiration. A new finding of decreased or absent corneal reflexes may indicate brainstem injury or increased intracranial pressure. For corneal impairment, lubrication and protection from direct injury prevents abrasions and ulcerations. Any deficit warrants nothing by mouth status and aspiration precautions until further evaluation.
Cranial nerve VI (abducens)
Mnemonic: 3, 4, and 6 make the eyes do tricks
Description: The abducens moves the eyes laterally beyond midline toward the ears.
Assessment and findings: To assess CN VI, ask the patient to follow your finger as you move it from midline toward the patient’s ear on one side and then the other. The affected eye won’t cross midline when following the finger to the ear. Impairment can result in diplopia and nystagmus.
Care implications: The abducens nerve travels the longest intracranial course, making it susceptible to injury that may result in a disconjugate horizontal gaze.
Cranial nerve VII (facial)
Mnemonic: 7 on the face
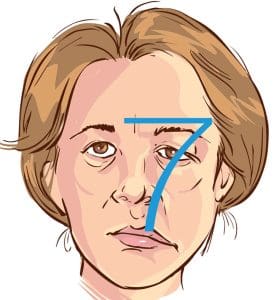
Description: The facial nerve has both motor and sensory functions. The motor component is responsible for facial expression, lip movement and tone, speech articulation, and corneal reflex response. The sensory component innervates the anterior two-thirds of the tongue, which detects taste. Imagine drawing a “7” across the eyebrows with the base ending at the mouth.
Assessment and findings: Abnormalities can be assessed when a noticeable droop in either the eyebrows, mouth, or both appear along the “7” when the patient is at rest. Asymmetry when the patient is asked to raise their eyebrows, smile, or open and close their eyes also is an abnormal finding. Place your finger on the patient’s closed eye. They should exhibit resistance as they attempt to open the eye. The nasolabial folds should be symmetric and not flattened. Because CN V is the sensory component of the corneal reflex and cranial nerve VII is the motor response, both must function for an intact blink response.
Care implications: Impairment of these nerves contributes to scratched or dry corneas with potential for infection and pain. Other problems include increased nasal and salivary secretions and pocketing food in the cheek, which raises aspiration risk. Any deficit warrants nothing by mouth status and aspiration precautions until further evaluation. [See figure 3.]
Cranial nerve VIII (acoustic or vestibulocochlear)
Mnemonic: 8 in the ear
Description: This sensory nerve allows for hearing and balance.
Assessment and findings: Determine if the patient can detect sound bilaterally. Examination techniques include whispering, rubbing fingers together, and observing if the patient leans forward or turns their head toward the sound. A tuning fork can aid assessment for sensorineural and conductive hearing issues. To evaluate balance, ask if the patient feels dizzy and assess their ability to sit, stand, and walk.
The Rinne and Weber tests, both of which are performed using a tuning fork, detect hearing loss. The Rinne test compares sound perception via air (placing the tuning fork next to the ear) and bone (placing the tuning fork behind the ear) conduction. Ask the patient to tell you when they no longer hear the vibration. At that point, quickly put the vibrating fork near the ear canal and ask the patient to alert you when they no longer hear the sound. Normally, the sound is heard longer in the air compared to the bone because it’s being amplified. If they hear the vibration longer on the bone, sound isn’t transmitting through the appropriate pathways. Conductive hearing loss is diagnosed when bone conduction is better than air conduction or sound doesn’t enter from the outer or middle ear. Sensorineural hearing loss is diagnosed when air conduction lasts longer than bone conduction or sound doesn’t reach the inner ear or nerve for synapsing.
The Weber test assesses for bilateral conductive and sensorineural hearing loss. The tuning fork is placed in the middle of the patient’s forehead, above the upper lip under the nose, or on top of the head equally distant from the ears. Louder sound in the affected ear demonstrates conductive hearing loss because bone conducts sound better than air. In sensorineural hearing loss, sound is heard better in the normal ear.
Romberg testing evaluates balance irregularities and distinguishes cranial nerve involvement from cerebellar dysfunction.
Care implications: Dizziness, impaired balance, and decreased hearing may compromise a patients’ safety. Implement and educate patients about protective measures such as hearing enhancers and fall precautions.
Cranial nerve IX (glossopharyngeal) and cranial nerve X (vagus)
Mnemonic: 9 and 10 under the chin
Description: The glossopharyngeal and vagus nerves control the gag and swallowing reflex, vocalization, and the posterior pharyngeal muscles. These nerves have motor and sensory functions and are assessed simultaneously. The glossopharyngeal nerve provides the sensory innervation for taste to the posterior tongue and some inner ear sensation.
Assessment and findings: Assess this cranial nerve by asking the patient to say “ah.” Watch for vocal clarity, uvula alignment, and symmetric posterior mouth movement. Gently touching both sides of the back of the throat with a tongue blade should elicit a gag response. In intubated patients, assess for presence and strength of cough via endotracheal suctioning.
Care implications: Hoarseness, uvula deviation, and absent or decreased cough may indicate aspiration and potential airway impairment risk. If any deficits are present, perform a formal swallow study. CN X also innervates most thoracic and abdominal organs, including the heart and GI tract. Deficits may cause cardiac arrhythmias and changes in bowel motility, which can lead to an ileus. Any deficit in CN IX and X warrants nothing by mouth status and aspiration precautions until further evaluation.
Cranial nerve XI (spinal accessory)
Mnemonic: 11 (one) on each shoulder
Description: The spinal accessory motor nerve elevates the shoulders and turns the head laterally.
Assessment and findings: Place your hands on the patient’s shoulders and ask them to shrug against your resistance and turn their head in both directions. Assess for symmetry and equal strength with movement.
Care implications: When considering extubation, ask the patient to lift their head off the pillow to determine if this nerve is intact.
Cranial nerve XII (hypoglossal)
Mnemonic: 12 stick out the tongue
Description: The hypoglossal motor nerve controls tongue movement and maintains it in a midline position.
Assessment and findings: Assess the nerve by asking the patient to stick out their tongue. Deviation to one side or the inability to stick out the tongue are abnormal findings.
Care implications: Any deficits in cranial nerves V, VII, IX, X, and XII indicate nothing by mouth status and aspiration precautions until further evaluation.
Prevent complications
Cranial nerves control essential sensory and motor functions, including protective reflexes. Understanding these functions can help you identify abnormalities and intervene to prevent potential complications.
Melissa Moreda is a diabetes clinical nurse specialist at the Duke Health System in Raleigh, North Carolina. Michelle Hill is the comprehensive stroke program coordinator at OhioHealth – Riverside Methodist Hospital in Columbus.
References
Bader MK, Littlejohns LR, Olson DM, eds. AANN Core Curriculum for Neuroscience Nursing. 6th ed. Chicago, IL: American Association of Neuroscience Nurses; 2016.
Bolek B. Facing cranial nerve assessment. Am Nurse Today. 2006;1(2):21-2.
Hickey JV. Comprehensive neurological examination. In Hickey JV, ed. The Clinical Practice of Neurological and Neurosurgical Nursing. Philadelphia, PA: Wolters Kluwer; 2019; 113-54.
Hickey JV. Neurological assessment. In Hickey JV, ed. The Clinical Practice of Neurological and Neurosurgical Nursing. Philadelphia, PA: Wolters Kluwer; 2019; 154-81.
Hickey JV. Overview of neuroanatomy and neurophysiology. In Hickey JV, ed. The Clinical Practice of Neurological and Neurosurgical Nursing. Philadelphia, PA: Wolters Kluwer; 2019; 47-92.
Hickey JV, Baumann JJ. Intracranial hypertension: theory and management of increased intracranial pressure. In Hickey JV, ed. The Clinical Practice of Neurological and Neurosurgical Nursing. Philadelphia, PA: Wolters Kluwer; 2019; 183-217.
Lussier BL, Olson DM, Aiyagari V. Automated pupillometry in neurocritical care: Research and practice. Curr Neurol Neurosci Rep 2019;19(10) 71. doi:10.1007/s11910-019-0994-z
University of Texas Southwestern Neurology. Cranial nerves music video. YouTube. January 14, 2016.

















