
Robert Walker*, your patient in the postanesthesia care unit, is recovering from laparoscopic cholecystectomy. The anesthesia provider tells you that the patient’s history is unremarkable and surgery went well. When you speak to Mr. Walker, he’s lethargic but awake and following commands. His vital signs are normal, and he’s receiving oxygen by face mask. He complains of moderate abdominal pain, and the anesthesiologist prescribes I.V. hydromorphone. Fifteen minutes later, you notice that Mr. Walker’s breathing is slow and shallow. He doesn’t respond to verbal commands but awakens with vigorous tactile stimulation. His pulse oximetry reading drops from 99% to 90%. What should you do?
Your knowledge and skill in basic airway management can mean the difference between life and death for your patient. This article offers simple, helpful tips for managing patients in respiratory distress or respiratory arrest using bag-valve-mask (BVM) ventilation. Applying these tips can help you save precious time.
What can go wrong
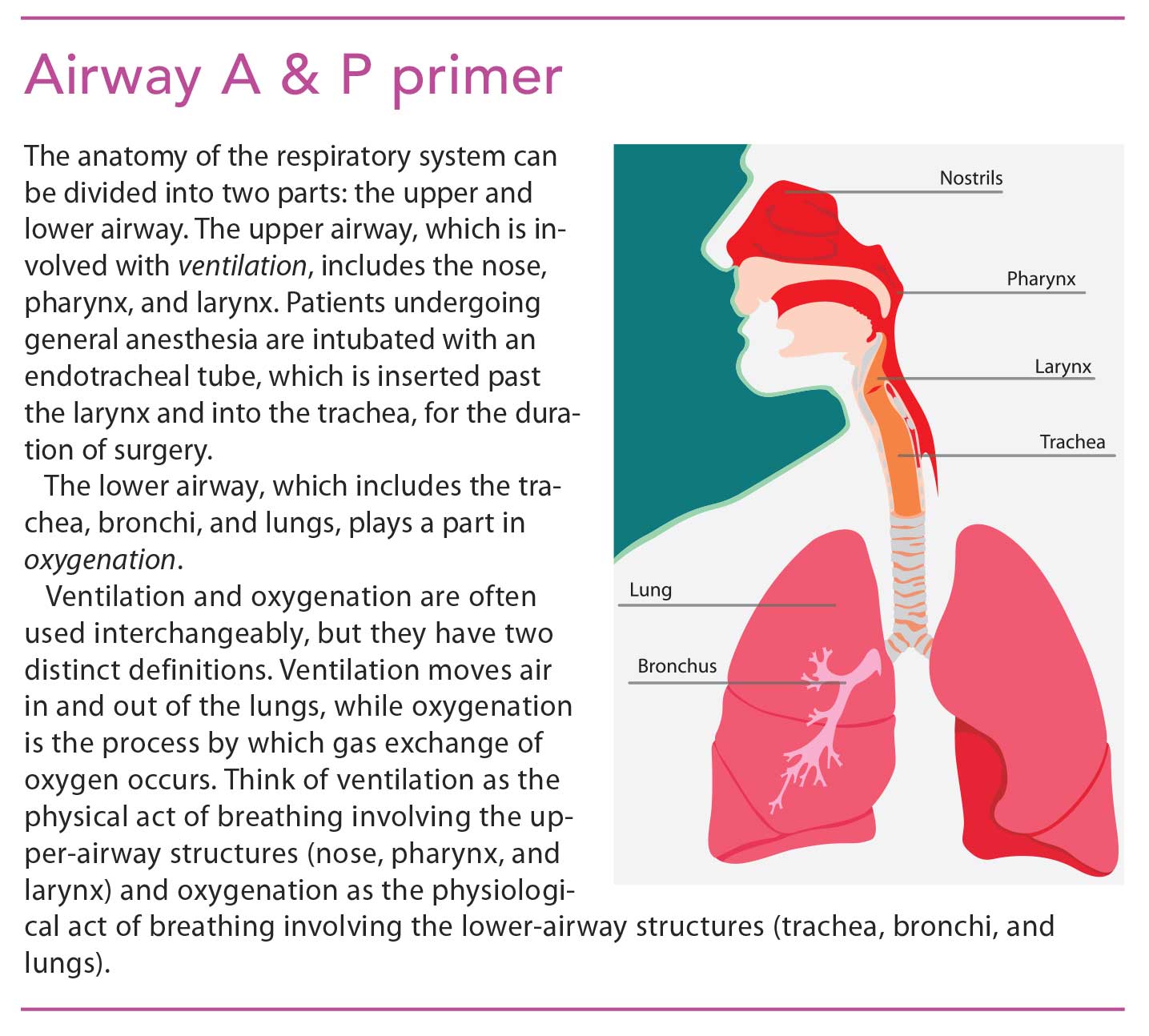
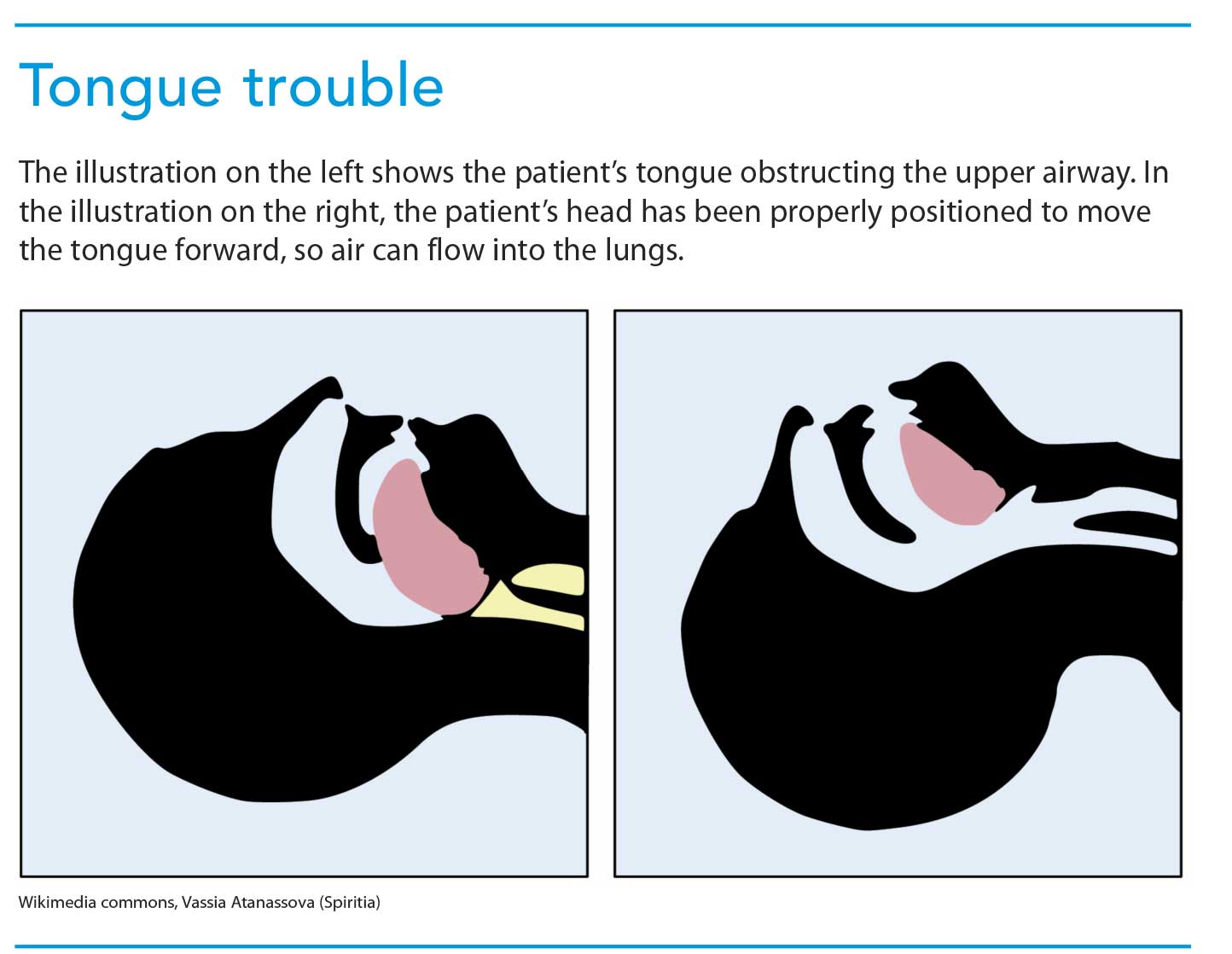
The respiratory system acts as a conduit for exchanging oxygen and carbon dioxide and fueling cells. (See Airway A & P primer.) When gas exchange is interrupted, respiratory distress may occur. This distress may be associated with an upper- airway obstruction, such as pharyngeal edema, laryngeal edema, trauma, or a foreign body lodged in the airway. But the most common cause of an upper-airway obstruction is the tongue. (See Tongue trouble.) Left untreated, respiratory distress can progress to respiratory arrest.
When you need BVM
You should use BVM ventilation in the following situations:
• a patient whose breathing is bradypneic, tachypneic, shallow, or weak
• a patient who has a decreased level of consciousness with or without decreased oxygen saturation
• a patient who is not breathing.
These indications are part of the ABCs of resuscitation, which start after you call for help when you find a patient in respiratory distress.
• Airway. Is the airway open? If the patient is unconscious, open the airway using the head tilt/chin lift (or jaw thrust if you suspect a cervical spine injury).
• Breathing. Is the patient breathing? If so, how effective are the breaths? In Mr. Walker’s case, his respiratory distress presents as slow, shallow breaths and a falling pulse oximetry reading. He needs your help with BVM.
• Circulation. Does the patient have a pulse? If not, start chest compressions. Fortunately, Mr. Walker has a pulse.
Be sure a colleague gathers essential airway management equipment, using the S.O.A.P. mnemonic to ensure everything necessary is brought to the bedside:
S—Suction
O—Oxygen
A—Airway (BVM, oral and nasal airways, endotracheal tube, laryngoscope blade, and airway crash cart)
P—Pharmacy (advanced cardiac life support drugs that are found on many crash carts).
Performing BVM ventilation
In patients like Mr. Walker who are experiencing respiratory distress but still breathing, use BVM ventilation to provide assistive breaths. Attach the BVM to an oxygen flow meter at greater than 10 L/min. Place the mask over the patient’s mouth and nose with one hand and, using your other hand, follow the patient’s breathing by gently and slowly squeezing the BVM to provide assistive ventilation.
Be aware that hyperventilation and overinflation forces air into the stomach, which can lead to gastric distention and place the patient at risk for aspiration. Also, the patient won’t be adequately ventilated. As you’re providing ventilation, watch for the rise and fall of your patient’s chest, listen for clear breath sounds on auscultation, and check for improved oxygen saturation and skin color.
Applying techniques you learned in basic life support help you manage the patient’s airway and ensure effective BVM ventilation.
Using the head-tilt/chin-lift maneuver
Use the head-tilt/chin-lift maneuver to open a patient’s airway, unless you suspect cervical spine injury, in which case, you should use a modified jaw thrust. Position the mask so it covers the patient’s nose and mouth. If the mask sits over the patient’s chin, you may have to readjust it so it sits near the edge of the chin, or get a smaller mask.
Inserting an oral or nasal airway
If you can’t provide adequate ventilation, the patient’s tongue may be obstructing the upper airway. Use an oral or nasal airway to displace the tongue forward. You can learn more about selecting and correctly placing oral and nasal airways at the American Red Cross website.
Maintaining a tight seal
To ensure oxygen is delivered to the lungs, you need an airtight seal over the patient’s mouth. To maintain that seal, use the E-C technique to hold the BVM: First, create a C-shape with your thumb and index finger over the top of the mask and apply gentle downward pressure. Then hook your pinkie, ring, and middle fingers around the patient’s mandible and lift it up toward the mask, creating an E.
Another option is the E-O technique. In this method, you use the web between your thumb and index finger to encircle the neck of the mask, while you lift the chin with your other fingers to provide chin lift.
If you have difficulty with the one-handed E-C or E-O techniques and another provider is with you, switch to the two-handed, two-person technique. Using both hands, grasp each side of the patient’s face using the E-C technique. Then pull the mandible up into the mask to provide an airtight seal. While you maintain the seal, the other provider ventilates the patient.
Clinical pearls
Using correct BVM technique, you can ensure proper ventilation of a patient in respiratory distress or respiratory arrest. Positioning your hands correctly on the mask and assessing for potential challenges increase your chance of success.
Pull, don’t push
A common mistake when performing BVM ventilation is to push the mask onto the patient’s face while delivering breaths. This pushes the tongue farther into the posterior pharynx, exacerbating the upperairway obstruction. To provide adequate ventilation, use the “E” fingers (pinkie, ring, and middle) from the E-C technique to pull the patient’s mandible into the mask, while at the same time using your thumb and index fingers to hold the mask in place.
Grasp bone, not soft tissue
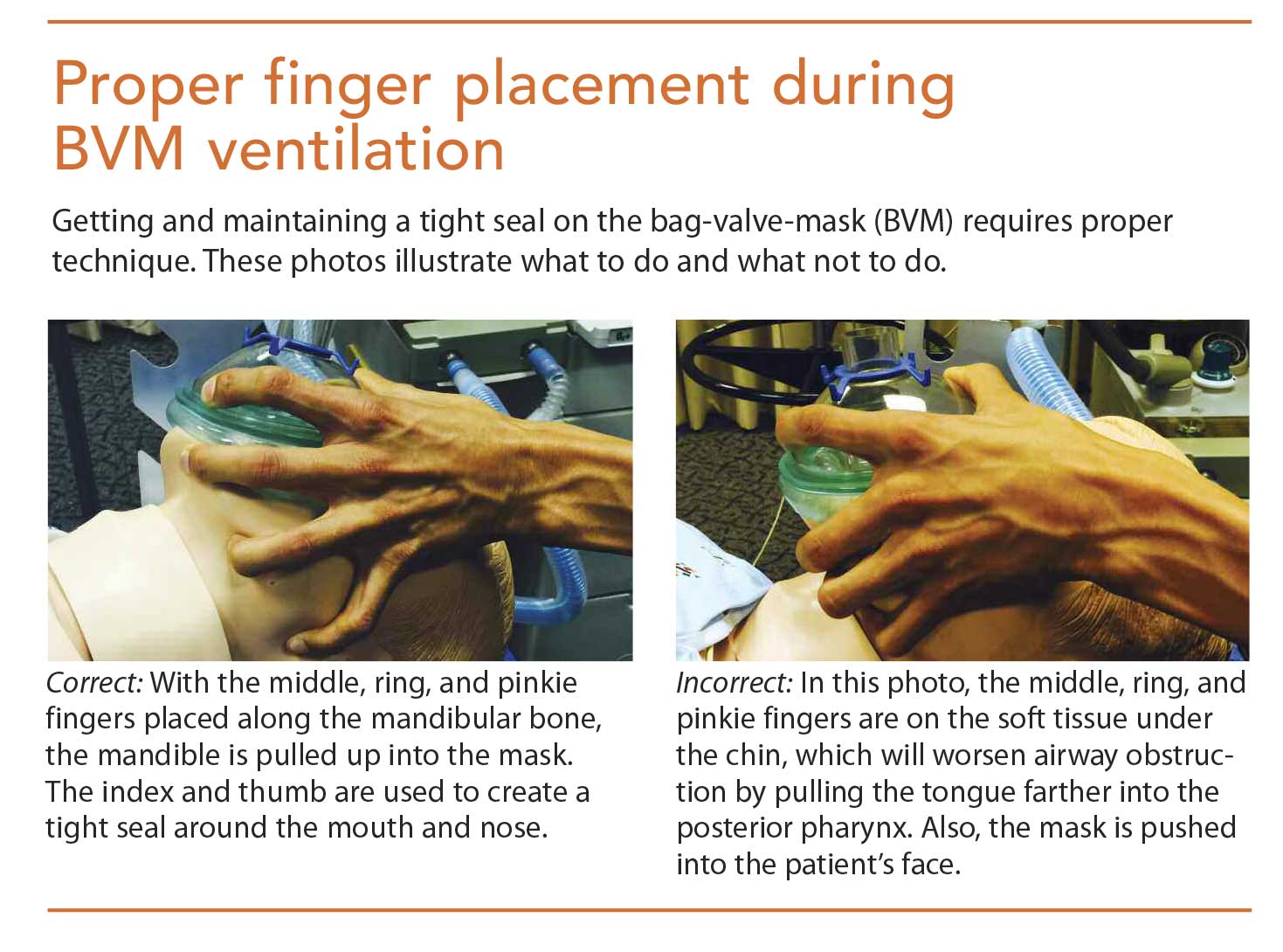
Another common mistake is using the fingers to grasp the soft tissue beneath the mandible. Like pushing on the mask, grasping the soft tissue can push the tongue into the posterior pharynx, worsening the obstruction. Use the E-C or EO techniques to avoid this error. (See Proper finger placement during BVM ventilation.)
MOANS
The MOANS mnemonic—mask seal, obese, age over 55, no teeth, and stiff—helps for problems you may encounter with the mask. These challenges can be overcome when you have the necessary materials and equipment nearby. (See Troubleshooting BVM problems.)
Airway management saves lives
Regardless of your patient’s comorbidities, using the simple techniques described in this article provides you with the tools you need to react quickly and appropriately when your patient suffers respiratory distress or respiratory arrest. Remember, airway management is the single most important skill needed to save a life.
Fortunately, your prompt intervention with a BVM to assist Mr. Walker’s breathing sustains him until he receives naloxone to reduce the sedative effect of hydromorphone. He does well and is discharged home without further problems.
Huy Vo, Matthew Park, and Simson Wang are certified registered nurse anesthetists at the University of California at Los Angeles.
*Names in clinical scenarios are fictitious.
Selected references
Apfelbaum JL, Hagberg CA, Caplan RA, et al. Practice guidelines for management of the difficult airway: an updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Anesthesiology. 2013;118(2):251-70.
Brown EN, Solt K, Purdon PL, et al. Monitoring brain state during general anesthesia. In: Miller RD, ed. Miller’s Anesthesia. 8th ed.
Philadelphia, PA: Elsevier Saunders; 2015: 1524-40.
Butterworth JF, Mackey DC, Wasnick JD. Airway management. In: Morgan & Mikhail’s Clinical Anesthesiology. 5th edition. New York, NY: McGraw Hill; 2013: 309-42.
Umesh G, Krishna R, Chaudhuri S, et al. E-O technique is superior to E-C technique in manikins during single person bag mask ventilation performed by novices. J Clin Monit Comput. 2014;28(3):269-73.
















{kind=link}
{kind=link}
{kind=link}