Nurse leaders say staffing status quo is unsustainable.
Frontline nurses and healthcare leaders know the impact staffing and scheduling have on clinical outcomes, patient satisfaction, staff engagement, and financial and compliance outcomes. However, as technology, reimbursement structures, patient population, and nurse demographics have changed, the approach to staffing has remained relatively the same.
I recently asked leaders from three nursing professional organizations to share their thoughts on the future of staffing. I also interviewed leaders at two health systems to gain insights into their staffing models and how they are preparing for the future.
Leaders of professional associations
Leaders from the American Nurses Association (ANA), American Association of Critical-Care Nurses (AACN), and the American Organization for Nursing Leadership (AONL) lend their expertise to the discussion about the future of nurse staffing.
ANA: Moving from volume to value
As nursing continues to use traditional and often outdated staffing approaches, the healthcare delivery system has undergone immense change, with more changes ahead. According to Debbie Hatmaker, PhD, RN, FAAN, chief nursing officer (CNO) at ANA Enterprise, the move from volume to the value of care provided, along with changes that will likely impact how and where nurses deliver care, requires updated staffing and scheduling strategies. Furthermore, value-based payment systems will continue to put an increased focus on patients’ experiences, safety, and quality of care. Delivering patient-centered instead of census-based care is a major staffing transition. Hatmaker suggests learning from other countries about their approaches to nurse staffing.
Hatmaker says that ANA is working to develop resources to address the staffing challenge, including a new focused website page and a revised version of ANA’s Principles for Nurse Staffing.
ANA Enterprise sees several significant changes coming in the next 5 years.
• Delivery of care is moving toward a more team-based model in all settings.
• The expansion of nurse-led, home-based, and mobile care models will expand nurses’ reach beyond traditional inpatient settings.
• New patient care complexities and addressing social determinants of health will increase demand for nursing services.
• Overall work environment stressors and the need to increase the actual number of nurses providing care must be addressed together.
• New technology such as artificial intelligence and robots will change the role and need for nurses in ways we don’t yet understand.
Hatmaker maintains that collaboration is key to addressing these issues. To that end, ANA is teaming up with its specialty nursing organizational affiliates and other stakeholder groups to share information and strategies on staff ing and related factors. ANA also is working with federal officials to compel the Centers for Medicare & Medicaid Services to provide Congress with information about how they assess “adequate” staffing levels as part of its 2020 budget request.
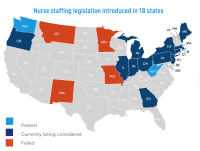
Another critical effort involves collaborating with Press Ganey to maintain National Quality Forum endorsement for two nurse staffing measures: skill mix and nursing hours per patient day, according to Hatmaker. Several states already require their hospitals to publicly report these measures, and ANA’s continued advocacy will focus on broad reporting at the national level, particularly with respect to Medicare.
When looking at how to address current and future staffing challenges, Hatmaker offers some suggestions. “First, we need to crea tively problem-solve with nurses to address staffing issues,” she says. “That means following the evidence that staffing levels impact patient outcomes and nurse sat isfaction, as well as continuing to test new models of care and pro cesses with ongoing input from direct-care nurses.”
Collaboration is key. “Nursing leaders must ensure that nurses at every level are empowered and represented whenever staffing is discussed,” Hatmaker says. “We also must create an active partnership across nursing and finance that includes clinical staff nurses.”
Hatmaker also points out that actively providing nurses with professional development opportunities that focus on leadership, innovative problem-solving, crucial conversations, finance, and strategies that promote high-performing teams is important.
Again, Hatmaker emphasizes that collaboration is critical. ANA continues to work with external partners to determine a unified legislative and regulatory approach that best fits direct-care nurses’ needs and ensures that they’re part of a collaborative decision-making process across all care settings.
AACN: Shifting from staffing as an expense to an investment
AACN is calling for a future where nurse staffing is viewed as an investment in patient outcomes, financial stability, and staff engagement. “Viewing staffing as an investment, and not merely an operational expense, is a major, grand-scale shift in how we think about delivering patient care,” says Christine Schulman, MS, RN, CNS, CCRN-K, past president of AACN. “Addressing pure numbers without also focusing on the environment and all of the other factors that influence how care is delivered won’t be enough.”
Schulman and other AACN leaders understand the complexity of the staffing issue.
AACN president Megan E. Brunson, MSN, RN, CNL, CCRN-CSC, says, “We are mobilizing our AACN community to identify innovative solutions and best practices that already work well or hold great promise for better outcomes.”
Leaders across the healthcare industry must be aligned in addressing the critical issue of nurse staffing. “Collaborating with all key stakeholders is essential,” Brunson says. “AACN is actively partnering with other nursing organizations, healthcare finance executives, and patient quality and safety experts to share knowledge about staffing and collaboratively define new approaches.”

The Joint Commission recommends that organizations embrace innovation to design and systematically test new staffing models. Lisa Riggs, MSN, APRN-BC, CCRN-K, immediate past president of AACN, says that “AACN is taking that seriously,” and points out that it requires giving nurses time away from direct patient care so they can identify opportunities for improvement and create solutions to unit challenges. “What if nurses could do this routinely?” asks Riggs. “Imagine the solutions we could come up with. We understand best how we work.”
Riggs notes that without a better staffing approach, real risk exists that we’ll lose large numbers of nurses, which will further exacerbate an already challenging situation. In a recent study with 8,080 nurse participants, 54% said they plan to leave their current position within the next 3 years, 33% of those in the next 12 months. When those reporting an intent to leave were asked what would influence them to reconsider, the top response was better staffing (50%).
AACN has developed many valuable nurse staffing resources. (See Staffing resources.)
Access these resources to help your organization address staffing issues.
American Association of Critical-Care Nurses (AACN)
• AACN Guiding Principles for Appropriate Staffing
• AACN Appropriate Staffing resources
• AACN Synergy Model for Patient Care
American Nurses Association (ANA)
• Watch for more information and related educational activities
American Nurse Today
AONL: Focusing on patient-centered staffing
Mary Beth Kingston, PhD, RN, 2019 AONL president and CNO for Advocate Aurora Health in Illinois and Wisconsin, notes that the issue of appropriate staff ing has been with us for many years. Key to understanding it is recognizing that staffing isn’t just about nurses. Staffing ultimately affects a host of outcomes for the patient, the staff, and the organization. How ever, these outcomes can’t be achieved by nurse staff – ing alone.
“We often fail to see the whole picture of this multifaceted process with its many moving parts that intersect with the complexity of nurse staffing,” Kingston says. “Dialogue, partnership, and strategic planning with a multitude of people and departments, including the CFO, support services, pharmacy and physicians to name just a few, to address the issues of staffing together—that collaboration is what will result in excellent outcomes.” To that end, AONL is working with nursing and healthcare organizations to develop a shared vision of staffing strategies and models for the future. The ultimate outcome must be patient safety, Kingston notes.
Issues such as population health, continuity of care across the continuum, and demands for better quality outcomes within the context of cost pressures will require a commitment to patient-centered staffing. “Achieving both quality and cost outcomes can be done only if we first focus on patient-centered staffing to achieve the right outcomes, and then utilize data to drive staffing decisions,” Kingston says. “Nurses and healthcare workers must also have the opportunity to work in a safe place and to enjoy a reasonable work-life balance. The needs of both staff and patients must be accounted for.”
Staffing technology is seen as an adjunct to the work of nurses and other caregivers in Kingston’s world. The technology must enhance nurses’ work rather than complicate it. Systems will need to integrate evidence-based data about staffing best practices, predictive census and acuity, and staff availability. The ability to then use that integrated data to make suggestions that lead to outcomes will be a requirement.
Taking the lead
Several health systems, including Advocate Aurora Health and Duke University Health System, are leading the way on staffing solutions.
CASE STUDY—Advocate Aurora: Multidisciplinary “ecosystems” for continuous improvement
At Advocate Aurora, Margaret Gavigan, MSN, MBA, RN, system vice president for clinical operations, is working closely with Kingston and others to meet the challenges of the next 5 years. “Effective nurse staffing matters to patients, families, and nurses, and it’s undeniably linked to improved patient safety, patient and workforce satisfaction, and operational outcomes in healthcare organizations,” Gavigan says. “Innovation in staffing and redesign in structures, people, process, and technology will be crucial to meet future patient and nursing workforce needs. Timely concurrent information and analytics will be vital to move from reactive staffing plans and decision-making to proactive, predictive planning with improved, consistent results.”
Advocate Aurora Health has created a new acute care staffing model to create a more flexible workforce and to provide structure for moving nurses within and across hospitals. This will allow the entire organization to better match clinical resources to patient demand and provide the foundation to eventually move nurses to staff alternative settings as acute care utilization decreases. The team used big data analysis to understand the complexities of patient demand and clinical resource supply and combine them to reliably achieve the organization’s nurse staffing goals.
The organization’s systematic approach for continuous staffing process improvements involves engaging each hospital’s leadership teams, including CNOs, financial officers, human resources (HR) executives, clinical educators, nursing directors, and hiring managers. All team members have clearly defined roles with assigned accountabilities to ensure effective nurse staffing. At these “ecosystem” meetings, the key metrics that drive effective staffing are reviewed and action plans are created to close any identified gaps and problem-solve opportunities to remove barriers. Site-based frontline nurse teams review staffing plans, and feedback is obtained to ensure optimum results. These structured team meetings have been key drivers of Advocate Aurora’s sustained improved staffing results.
Advocate Aurora has achieved year-over-year sustained improvement in staffing measures of success. Current system results include improving and meeting targets in the following measures:
• overall RN voluntary turnover: 9.38%
• first-year RN turnover: 17.63%
• percentage of overtime and agency worked hours: reduced to 1.8%
• Illinois hospitals: Improved system RN perception of staffing composite in the Agency for Healthcare Research and Quality Culture of Safety Survey moved from the 36th percentile in 2015 to the 75th percentile in 2018.
CASE STUDY—Duke Health: Leveraging analytics and optimizing technology
At Duke University Health System, the connection between staffing and nurse recruitment/retention is crucial for nursing leadership to meet the challenges coming in the next 5 years. According to Vicky Orto, DNP, RN, NEA-BC, chief nursing and patient care services officer at Duke, “It will be imperative that CNOs focus on staffing and the hiring process as a strategic priority. Staffing must become job one. Often this will require the CNO to be the bridge between HR and nursing.” For Orto, innovative staffing models that make the most of scarce RN resources and provide nurse managers with ongoing support to assist with effective recruiting, hiring, and onboarding strategies also are priorities. Sylvia Alston, MSN, RN, NEA-BC, assistant vice president at Duke, adds, “It will be important to ensure that our nurses are practicing at the top of their scope/license and we are employing innovative recruitment and retention strategies.”
The team at Duke uses a collaborative approach to improve all processes related to nurse staffing, scheduling, hiring, onboarding, recruiting, and retaining, with a health system committee led by the CNOs with members that include HR partners, directors, nurse managers, and staff RNs.
Technology and analytics are at the core of Duke’s staffing strategy. Nursing has partnered with management engineering to ensure that it has data to drive staffing improvements, and an optimization project is underway to make sure technology supports staff ing. Duke also has developed a health system model for predictive hiring based on historical census and turnover, which allows managers to hire proactively based on those predictions. The commitment to technology and data is yielding results. Duke has seen its turnover rates and time-to-fill numbers decrease over the last 4 years. Results include:
• Overall turnover rates decreased from 17.9% to 14%.
• Time-to-fill days went from 69 to 51.
• Vacancy rates have remained stable at 2% to 3%, with an annual growth of 2% per year.
Critical first steps: What your organization can do today
After serving as CNO for three large health systems and in my current role as CNO for API Healthcare, addressing staffing challenges has been in my sights for decades. Unfortunately, staffing strategies haven’t kept up with the pace of healthcare change. Although the issue has become increasingly critical and long-term change will take time, I see cause for optimism. Leaders from ANA, AACN, and AONL and multiple disciplines are aggressively attacking the staffing issue and are working collaboratively to define the future of staff ing. And leading organizations across the country are effectively addressing this most pressing issue.
Consider implementing these proven strategies at your organization to pave the way for current and future success: • Collaborative multidisciplinary shared governance for staffing: Bring key stakeholders together for ongoing dialogue to develop strategies that invest in staffing to deliver balanced outcomes. • Policy and process standardization: When staffing policies and practices are standardized across an organization, matching nurses with patient care needs is easier, and valuable staffing resources are optimized. • Technology optimization: Use smart technology to strategically move from opinion-based, numbers-driven staffing to data- and research-driven staffing.
Although the issues surrounding staffing are riddled with complexity, Riggs provides us with clarity: “We must never forget our true north—the needs of patients and their families.”
Karlene Kerfoot is the CNO at API Healthcare, now a part of symplr in Hartford, Wisconsin.
Selected reference
Ulrich B, Barden C, Cassidy L, Varn-Davis N. Critical care nurse work environments 2018: Findings and implications. Crit Care Nurse. 2019;39(2):67-84.