A role for all nurses.
Editor’s note: This is an early release of an article that will appear in the February 2022 issue of American Nurse Journal.
Takeaways:
- Nurses have an important role in helping patients, families, and communities access credible, trusted health information.
- Nurses should consider the foundational attributes of information sources when engaging on social media platforms where professional, social, and familial identities may converge.
On July 15, 2021, the U.S. Surgeon General issued an urgent plea for all Americans to take part in slowing a serious threat to public health. He wasn’t talking about the COVID-19 pandemic but rather the deleterious effects on personal and public health caused by the creation and spread of health misinformation. Nurses, cited as the most trusted profession for their honesty and ethical standards, have a critical responsibility in combating misinformation and in helping patients, families, and communities identify and access credible, trusted health sources.
Misinformation: Then and now
A difference exists between misinformation and disinformation. Misinformation is false, inaccurate, or misleading information. Disinformation is a deliberate intent to deceive for political, personal, and monetary gain. Health misinformation has a long history. A well-known example is an 1802 cartoon depicting people turning into cows after receiving smallpox inoculations. In America, the term “snake oil” refers to ineffective and even poisonous “medications” popularized by traveling salespeople and newspaper advertising.
Although these past incidents echo in the digital age, the high volume and wide array of sources of information and content—all propagated, refined, and disseminated at warp-speed via computing networks and platforms of previously unimaginable power and reach—amplifies the problem. Social media platforms (SMPs), a major source of information dissemination, provide visually appealing content (such as memes or engaging images or tweets) that communicates simplistic messages and evokes suspicion. This stands in contrast to peer-reviewed science publications that provide more accurate information but tend to be densely worded and complex, preventing the same impact or uptake of SMP messages. In addition, studies by Chen and colleagues and Vosoughi and colleagues indicate that false information may more rapidly diffuse and spread further in part because of the strong emotions they may elicit.
The spread of misinformation also may be driven by the commercial interests of SMPs to increase engagement by presenting opinions, statements, and images that reward, affirm, and closely affiliate with a user’s real, assumed, or social interests. SMPs use algorithms and prioritize content based on popularity or similarity to a user’s previously viewed content. The resulting information creates a bubble composed of narrowly tailored messages based on individual interests, exposing users to more extreme perspectives while insulating them from neutral or opposing ones.
SMPs’ high volume of information and lack of quality control can lead to a preponderance of low-quality information, misinformation, or disinformation when patients, families, and communities search for answers to health questions. Misinformation has accelerated during the pandemic, resulting in what the World Health Organization (WHO) calls an “infodemic.” The effects include confusion and support for behaviors that can harm health, lead to mistrust in science, and ultimately undermine the public health response to the pandemic.
SMPs must do more to minimize these harms. They must implement policies and technical improvements that evaluate, promote, and imbed information from credible and verifiable sources of health information. Content labeling and transparency also can help reduce misinformation.
Nurses and misinformation
Nurses play an important role in reducing health misinformation harm and helping patients, families, and communities access credible, trusted sources. The Code of Ethics for Nurses with Interpretive Statements includes the duty to respect the inherent dignity of every person, including protecting a patient’s right to autonomy. But truly autonomous decision-making and informed consent are possible only when information is accurate, complete, and understandable. Nurses must ensure that patients have access to credible information, which can be defined simply as that which is consistent with the best scientific evidence available at the time.
How do nurses and other health professionals identify credible information? Foundational principles of credible sources of health information proposed by Kington and colleagues include science-based, objective (biases and conflicts are disclosed), and transparent and accountable. (See Credible health information: Foundational principles and attributes.) Librarians, especially those specializing in health and undergraduate education, have developed many rubrics and tools to help consumers navigate the credibility and authority of online information.

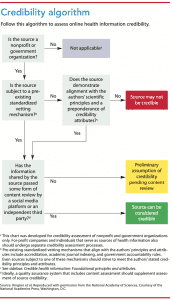
Blakeslee’s CRAAP (or CRAP) test, one of the most well-known and widely used formal tools for source criticism, encourages users to walk through brief pathways to identify key areas of online source credibility (for example, currency, relevance, authority [author’s credentials], and purpose). CRAAP and similar tests can help evaluate traditional websites but may be less helpful in analyzing social media misinformation and disinformation. Kington and colleagues also developed more granular attributes and an algorithm to aid in assessing sites and information. (See Credibility algorithm.)
Nurses should consider these foundational attributes when interacting on SMPs where their professional, social, and personal identities may converge. In addition, they should integrate them into clinical practice. Health systems concerned with training, accreditation, and patient education can support and sustain health professionals’ scientific and statistical literacy beyond undergraduate and graduate education by providing continuing professional education, establishing journal clubs, and promoting awareness of reliable resources (such as Khan Academy and Cochrane’s Students 4 Best Evidence).
Patients and families trust nurses to identify, recommend, and affirm credible sources of information. However, recommending a source also must include assessing the appropriateness of how information is presented, how patients navigate complex health information, and whether they trust the sources (even if they’re credible). Many credible sources are fact- and text-dense, requiring advanced comprehension skills and vocabulary, and they may present complex findings that patients find difficult to understand. In addition, most credible scholarly research in the health sciences languishes behind subscription paywalls, making it inaccessible to most patients.
Many publishers, particularly those who work with practice guidelines and high-quality reviews (including Cochrane Reviews, the Joanna Briggs Institute, the Patient-Centered Outcomes Research Institute, and journals such as Pediatrics), have started to recommend or require plain-language summaries, infographics, video abstracts, and other comprehensible, openly available, and shareable content alongside the original scholarly document.
Before recommending sources, assess where and why people access health information. Many health professionals and librarians routinely refer patients to government websites, including the Centers for Disease Control and Prevention and National Institutes of Health (NIH). However, many individuals and communities, for historical or political reasons, don’t trust the government. Other credible sources, such as MedlinePlus, WHO, and KidsHealth, also rank highly in search results and could be shared as credible sources along with websites such as Snopes (snopes.com), FactCheck (Factcheck.org), and PolitiFact (politifact.org). Health website certification programs, such as Health On the Net (www.hon.ch), provide review and verification of health-related internet sites. Definitions of credible nonprofit entities can help you identify nongovernmental information sources.
Nurses and consumers must develop skills to evaluate information critically. A study examining the impact of trust in science found that people with a high trust in science were more likely to believe and disseminate misinformation about COVID-19 and genetically modified organisms in the presence of a scientific reference compared to false claims without scientific references. These findings underscore the importance of critically evaluating information, even from trusted sources.
A call to action
The Surgeon General recommends specific healthcare professional and organization actions to combat misinformation. Fundamental to these actions is to create an environment of trust by demonstrating empathy and curiosity, which encourages patients and families to share concerns and ask questions.
Proactively engage with patients and the public about health information.
- Acknowledge the barrage of health information available through technology platforms and other sources and the difficulty of “knowing who and what to trust.” (“I know there’s a great deal of information about COVID and not all of it is the same. Sometimes, it is hard to sort it out and know what to trust.”)
- Assess where patients and families get their health information and what sources they trust. Frequently, credible sources aren’t trusted sources. (“Where do you get most of your information about COVID-19? What makes that a trusted source for you?”)
- Provide alternate and accurate sources of information. (“I’m not familiar with that website, but I’ll look at it and let you know what I think. In the meantime, here’s where I get information and why I trust it.”)
- When correcting misinformation be nonjudgmental. (“I’ve heard similar information about not getting vaccinated. Here’s what I’ve learned from the science and why I believe getting vaccinated is important and safe.”)
Use technology and media platforms to share accurate health information with the public.
- In addition to serving as a subject-matter expert and sharing peer-reviewed research, provide broadly accessible information via various platforms. For example, Dear Pandemic (dearpandemic.org) is a team of researchers and clinicians, including nurses, committed to answering questions and concerns with facts about COVID-19. They have platforms on Twitter and Facebook and serve as sources for public and professional media.
- Although not all health professionals are comfortable with social media, you and your interprofessional colleagues should consider when and how your voices can be best used to promote credible, evidence-based health information.
Partner with community groups and local organizations to prevent and address health misinformation.
- Nurses are important members of many communities beyond their relationships with patients, including in faith organizations, school, work, and social circles. Use opportunities to partner with these to provide and clarify information about COVID-19.
- The NIH Community Engagement Alliance (covid19community.nih.gov) provides national and local resources that you can use and share.
Answer the call
COVID-19 has demonstrated the need to prioritize science communication and public engagement at every level of society. Nurses understand that facilitating education and public access to health information provides pre-exposure prophylaxis against misinformation. As we all know, prevention is better than cure. Treating people for the harms of the infodemic is both difficult and uncertain, but nurses have access to a wealth of tools, principles, and approaches for ensuring that patients and communities receive evidence-based, up-to-date, and credible health information. The COVID-19 pandemic and related infodemic are calling us all to act in our professional and personal lives. How will you answer the call?
Nonprofit entities that share health information
Use this table to help identify nonprofit entities that share health information (excluding health care organizations, health plans, government organizations, and public health departments.)


a. For example, an organization could seek public comments on an interim set of health guidelines before finalizing and sharing the information more broadly.
b. A consensus process involves assembling a group of experts with diverse perspectives who assess a body of evidence and deliberate in order to arrive at an opinion or guidance that reflects the consensus of the group.
c. A peer-review process involves sharing the draft of a publication or other product with reviewers who have expertise or experience in the given topic and can provide feedback as to the product’s accuracy, balance, and appropriateness.
d. For example, an academic journal could maintain editorial independence (i.e., sole authority over published content) from the organization that funds it.
e. For example, an organization might host an advertisement for a cancer drug but keep this advertisement separate from the information it shares about cancer.
f. FACA stands for the Federal Advisory Committee Act, which established requirements for committees that advise the federal government. These requirements include public access to meetings and meeting notes, as well as summaries of expenditures (gsa.gov/policy-regulations/policy/federal-advisory-committee-management/advice-and-guidance/the-federal-advisory-committee-act-faca-brochure).
Source: Kington et al. Reproduced with permission from the National Academy of Sciences, Courtesy of the National Academies Press, Washington, D.C.
The authors work at the University of Pennsylvania. Antonia M. Villarruel is a professor, Margaret Bond Simon Dean of the School of Nursing, and senior fellow in the Leonard Davis Institute of Health Economics. Richard James is nursing liaison librarian and clinical outreach coordinator for the University of Pennsylvania libraries.
Acknowledgment
Aliza Narva, JD, MSN, RN, HEC-C, director of ethics at the Hospital of the University of Pennsylvania provided assistance by reviewing the article before submission.
References
American Nurses Association. Code of Ethics for Nurses with Interpretive Statements. Silver Spring, MD: ANA Enterprise; 2015. nursingworld.org/practice-policy/nursing-excellence/ethics/code-of-ethics-for-nurses/coe-view-only
Blakeslee S. The CRAAP Test. LOEX Quarterly. 2004;31(3). commons.emich.edu/loexquarterly/vol31/iss3/4
Center for Countering Digital Hate. Malgorithm: How Instagram’s Algorithm Publishes Misinformation and Hate to Millions During a Pandemic. March 9, 2021. counterhate.com/malgorithm
Chen J, Liu Y, Zou M. User emotion for modeling retweeting behaviors. Neural Netw. 2017;96:11–21. doi: 10.1016/j.neunet.2017.08.006
Chou W-YS, Gaysynsky A, Vanderpool RC. The COVID-19 misinfodemic: Moving beyond fact-checking. Health Educ Behav. 2021;48(1):9-13. doi:10.1177/1090198120980675
Kington RS, Arnesen S, Chou W-YS, Curry SJ, Lazer D, and Villarruel AM. Identifying credible sources of health information in social media: Principles and attributes. NAM Perspect. 2021. doi:10.31478/202107a
O’Brien T, Palmer R, Albarracin, D. Misplaced trust: When trust in science fosters belief in pseudoscience and the benefits of critical evaluation. J Exp Soc Psychol. 2021;96:104184. doi:10.1016/j.jesp.2021.104184
Office of Disease Prevention and Health Promotion. Health literacy online: A guide to simplifying the user experience. June 8, 2016. health.gov/healthliteracyonline
Office of the Surgeon General. Confronting Health Misinformation: The U.S. Surgeon General’s Advisory on Building a Healthy Information Environment. US Department of Health and Human Services. 2021. hhs.gov/sites/default/files/surgeon-general-misinformation-advisory.pdf
Saad L. U.S. ethics ratings rise for medical workers and teachers. Gallup. December 22, 2020. news.gallup.com/poll/328136/ethics-ratings-rise-medical-workers-teachers.aspx
Swire-Thompson B, Lazer D. Public health and online misinformation: Challenges and recommendations. Annu Rev Public Health. 2020;41:433-51. doi:10.1146/annurev-publhealth-040119-094127
Simpson E, Conner A. Fighting Coronavirus misinformation and disinformation: Preventive product recommendations for social media platforms. Center for American Progress. August 18, 2020. americanprogress.org/issues/technology-policy/reports/2020/08/18/488714/fighting-coronavirus-misinformation-disinformation
Vosoughi S, Roy D, Aral S. The spread of true and false news online. Science. 2018;359(6380):1146-51. doi.org/10.1126/science.aap9559
World Health Organization. Infodemic. 2021. who.int/health-topics/infodemic#tab=tab_1