Imagine this scenario: A state senator, after reviewing a letter from a constituent supporting her bill to remove practice barriers for nurses, asks the nursing organization’s lobbyist, “Is this person a nurse?” These credentials followed the letter-writer’s signature: BSN, MSN, DNP, APRN-BC, CDE, FAANP, FAAN. Even as a nurse, I sometimes have a hard time understanding the alphabet soup of credentials, so imagine how difficult it must be for everyone else.
You work hard to meet the expectations and requirements of colleges, state agencies, and professional organizations to obtain degrees, licenses, certificates, and awards. After all of that work, you want the recognition that comes with placing the appropriate credentials after your name. However, you want to use them appropriately and to benefit your message.
To avoid confusion, follow recommended professional guidelines. This is what the ANA has to say about credentials: “…the use of credentials is an essential component to designate levels of attained education and licensure, certification, and professional achievement. The listing of credentials when identifying a nurse ensures credibility and competence to the consumers of nursing care.” You should also ask yourself, “Why am I using my credentials and who is my target audience?”
Here’s an overview of key credentials and recommendations on how and when to use them.
Educational credentials
Educational credentials include degrees or diplomas. Undergraduate nurses generally receive an associate degree in nursing (ADN) or a bachelor of science in nursing (BSN). The most common nursing graduate degrees are master of science in nursing (MSN), doctor of philosophy in nursing (PhD), doctor of nursing science (DNS), and doctor of nursing practice (DNP).
The ANA recommends you list the highest educational degree first, because once the criteria for a degree has been met, it’s permanent, unlike, for instance, a certification that is not renewed. You should also capitalize credentials without using periods, but with commas between each credential. If all of your degrees are from the same program area (for example, all nursing), only the highest degree should be provided (for example, S. Barton, MSN, not S. Barton, BSN, MSN). However, with different areas of focus, additional degrees can be included (for example, S. Barton, MSN, MBA).
Legal credentials
A nursing license is a legal credential, with each state requiring the title of registered nurse (RN). In the United States, specific criteria to obtain a license include passing the National Council Licensing Examination (NCLEX) and graduating from a state-approved nursing school. Your license credentials follow your educational credentials (for example, C. Hathaway, BSN, RN).
Legal credentials for nurses meeting criteria beyond that of an RN vary from state to state. The Consensus Model for Advanced Practice Registered Nursing- APRN Regulation, which is supported by many nursing organizations, recommends that the licensed title be advanced practice registered nurse (APRN). Within this model, there are four legal recommended titles or roles: certified registered nurse anesthetist (CRNA), certified nurse-midwife (CNM), clinical nurse specialist (CNS), and certified nurse practitioner (CNP). If you have an APRN license, you don’t need to include your RN title (for example, P. Crane, MSN, APRN, CNM). Keep in mind that not all states have approved this model. Other license titles include advanced registered nurse practitioner (ARNP), advanced practice nurse (APN), or adult nurse practitioner (ANP).
Professional credentials
The ANA defines certification as “the formal recognition of the knowledge, skill, ability, judgment, and experience demonstrated by the achievement of formal criteria identified by the profession.” Nursing organizations that provide certifications must be accredited by organizations such as the National Commission for Certifying Agencies. Receiving a certification is generally a professional credential, but it also can be a legal credential if the law requires it. For instance, certified nurse midwife (CNM) is both the professional certification and the legal title in some states.
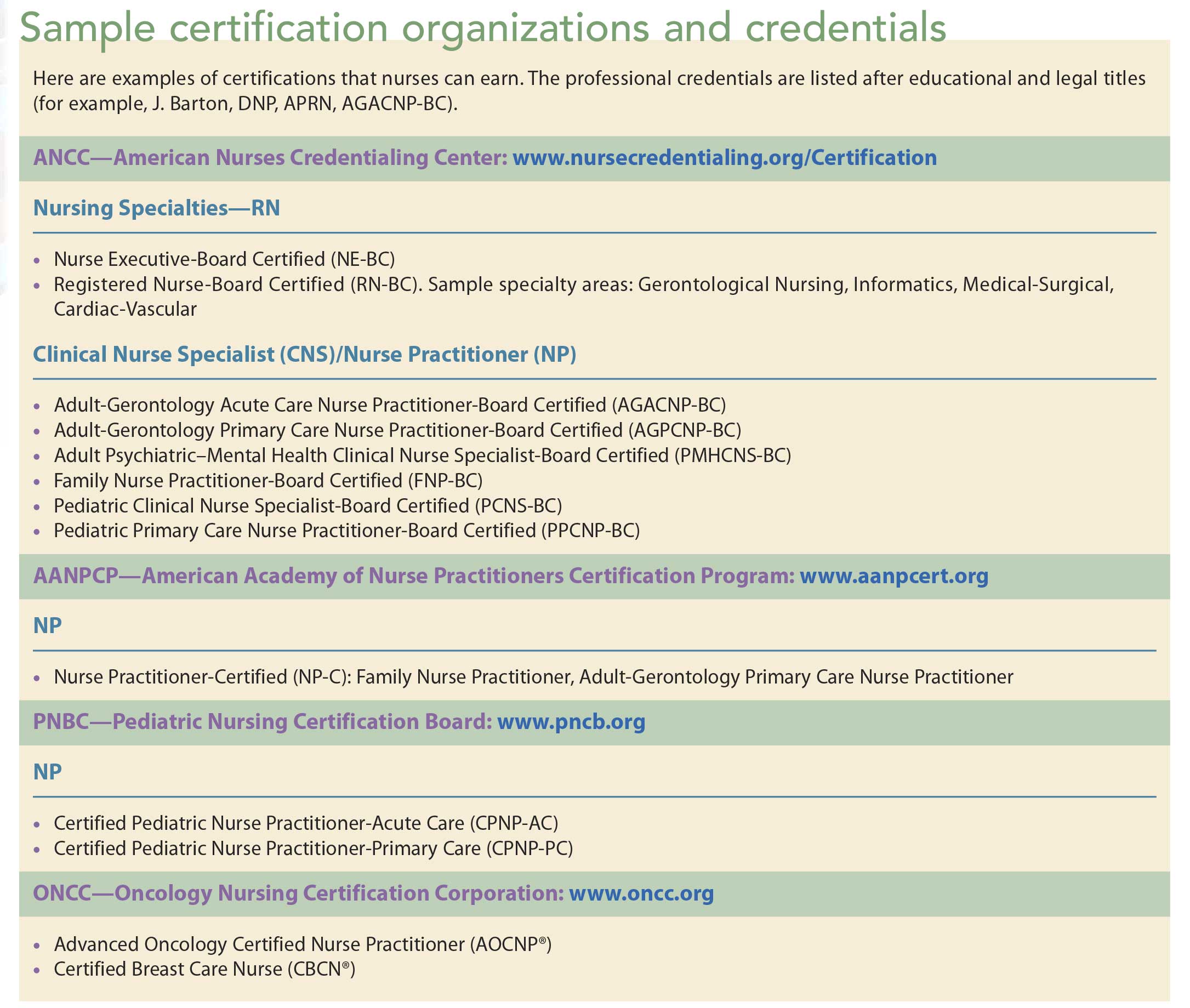
Certification typically requires that you complete a competency exam and, depending on the certification, specific educational or practice experiences. Many certification credentials need to be renewed by maintaining licensure and meeting renewal requirements. In most cases, certification is tied to a specialty role and not the legal title, unless the legal title is the same as the professional credential. Several organizations provide professional certification. (See Sample certification organizations and credentials.)
Most nurses get involved in leadership roles as well as research and community activities, which can lead to honors and awards. One of the highest awards in nursing is to be inducted as a Fellow of the American Academy of Nursing (FAAN). Other examples include Fellow of the American Association of Nurse Practitioners (FAANP), Fellowship in the American College of Nurse-Midwives (FACNM), and National League for Nursing Academy of Nursing Education Fellows (ANEF). These types of awards should be listed at the end of the credentials list (for example, J. Jones, PhD, CRNA, FAAN).
Know your audience
Determining when to use what credentials sometimes depends on your organization’s policy. Legal documents like charts and prescriptions, for example, typically require only the credential required by your state (RN or APRN). Depending on the legal document, you might want to include your educational credential, but check your employer’s policies. When applying for a job, an award, or submitting a professional presentation or paper, you’ll probably want to use all of your earned credentials.
But what if your audience is a group of policy makers or the public? In that case, the decision about what credential to use depends on what you’re trying to accomplish. Nurses continue to have the highest integrity rating in the nation, so using your RN credential can be a powerful tool. It can be especially helpful when communicating with the public in letters to the editor or trying to influence policy makers on essential health topics. That RN may be the only credential you need. Using educational or professional credentials, which most non-nurses do not understand, will only be a distraction.
However, if you’re trying to encourage policy change to remove practice barriers, policy makers need to understand our different roles and how they are linked to our education. In that case, using your relevant educational degrees may prove to be an advantage. Include your certification credential, but spell it out along with the abbreviation so everyone understands what it means.
Bottom line, when listing your credentials, know your audience and remember that listing more is not always better. Most important, always use RN or APRN to give voice to nursing.
Betty Smith-Campbell is a professor at Wichita State University School of Nursing in Wichita, Kansas.
Selected references
American Academy of Nursing. Academy Fellows.
American Association of Nurse Practitioners. Fellows Program.
American College of Nurse-Midwives. ACNM Fellowship.
American Nurses Association. Credentials for the Professional Nurse: Determining a Standard Order of Credentials for the Professional Nurse. Washington, DC: American Nurses Association; 2009.
American Nurses Association. Nursing’s Social Policy Statement: The Essence of the Profession . 3rd ed. Washington, DC: American Nurses Association; 2010.























{kind=link}