
It’s 7:30 am, and you’ve just received report on your patients. One of them, Anna Clark, age 77, is a postoperative patient who underwent an abdominal aortic aneurysm repair last evening. It was a difficult case, so instead of placing a minimally invasive stent in the aorta, surgeons performed an open repair that lasted several hours. During surgery, Mrs. Clark had a bleeding episode that caused her blood pressure to drop; she recovered after receiving three units of packed red blood cells and two units of fresh frozen plasma.
You review her laboratory results drawn at 5 am today, her first postoperative day. All values appear to be normal. Because of Mrs. Clark’s bleeding episode, you double-check her blood urea nitrogen (BUN) and creatinine values, as her advanced age and blood loss can decrease blood flow to the kidneys, causing acute kidney injury (AKI). You note her BUN is 13 mg/dL and her serum creatinine level is 0.4 mg/dL.
You set your priorities for the day, including medication administration, noting that Mrs. Clark is receiving the antibiotic vancomycin. In addition to monitoring her vital signs and urine output, you plan to start mobilizing her early and getting her out of bed.
For the rest of your shift, Mrs. Clark shows no signs of problems. The next day, you have the same patient assignment. On report, the night shift nurse mentions Mrs. Clark has been stable but her urine output is marginal at 4 mL/kg/hour. When you check her lab results, you see her renal function tests are at the high end of normal, including BUN at 24 mg/dL and creatinine at 1.0 mg/dL. Nonetheless, the nephrologist says he’s not concerned.
But if you think she’s doing well, you’re wrong. Although Mrs. Clark seems to be okay (despite her marginal urine output), she’s actually experiencing AKI. To make matters worse, on rounds, the team reviews her medications and orders an additional antibiotic, piperacillin/tazobactam.
A silent and deadly condition
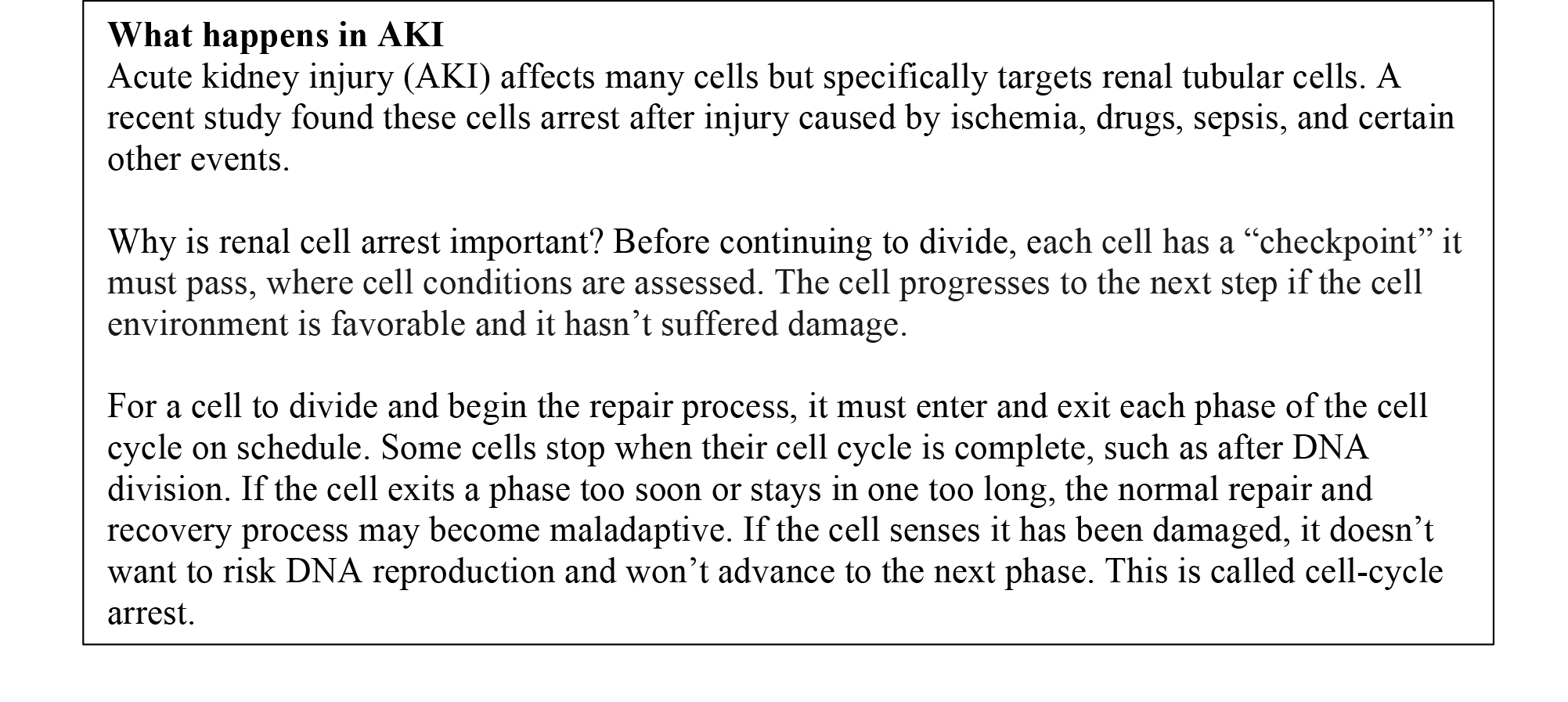
A serious complication for any patient, AKI can cause kidney impairment ranging from mild to complete loss of function. AKI is twice as deadly as myocardial infarction. Studies show patients who develop AKI have a significantly increased mortality risk. Even 1 day of AKI can increase the risk 20%. (See What happens in AKI.)
Unfortunately, no specific symptoms indicate in real time that kidney injury is occurring. For the most part, AKI is silent until kidney damage becomes severe. Most healthcare professionals rely on conventional blood tests—specifically BUN and serum creatinine—to determine if AKI has occurred. Yet these tests don’t reveal when kidney damage occurs or the degree of renal impairment.
Today, much more sophisticated tests are available that can predict AKI and indicate a patient has, or is likely to get, this serious condition. Within a few hours of renal injury, these tests detect biomarkers in the blood or urine, signaling the patient is likely to experience AKI or is already experiencing it.
Understanding AKI biomarkers
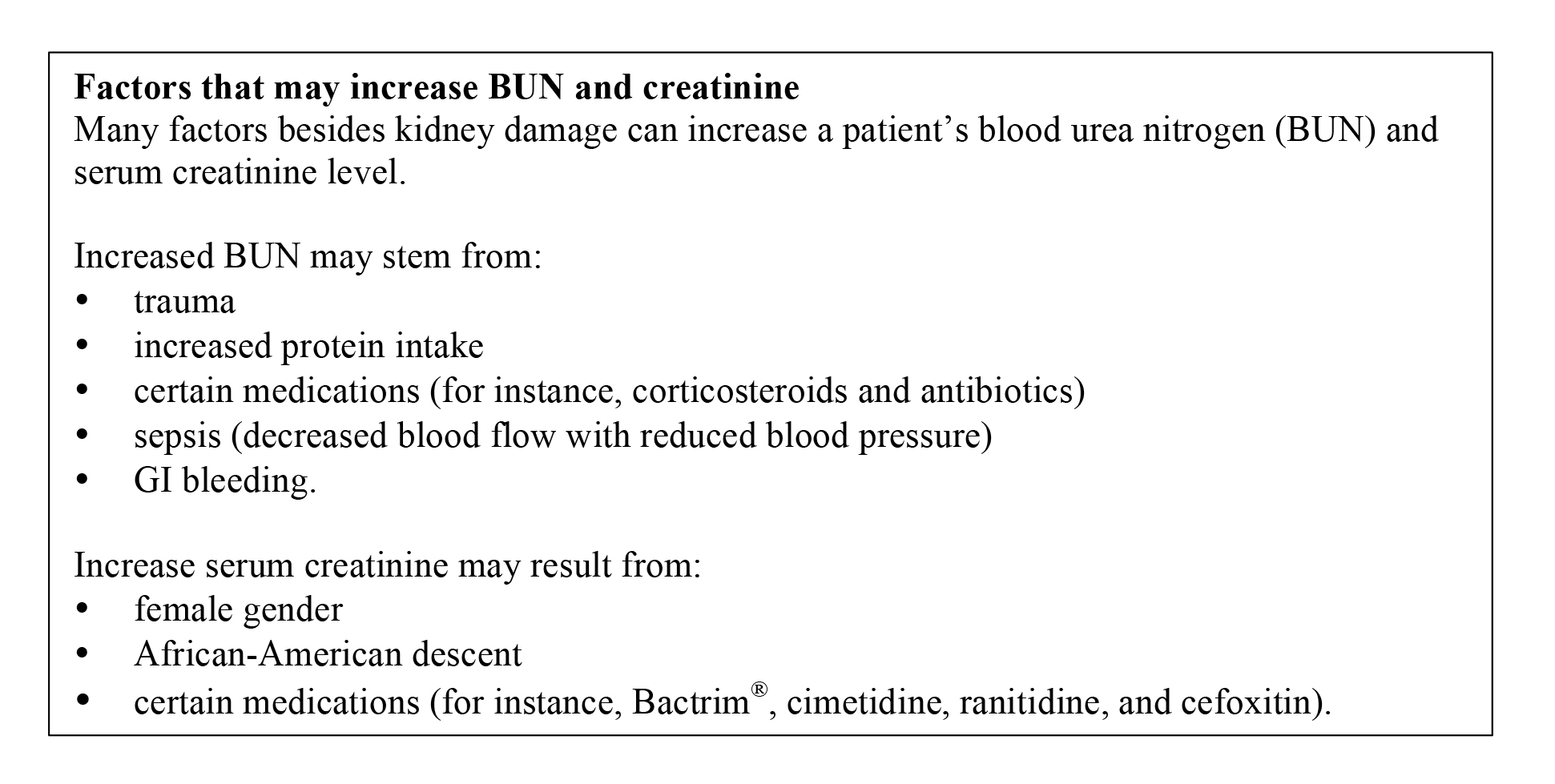
Until recently, AKI diagnosis and staging were based exclusively on serum creatinine and BUN elevations, decreased urine output, or both. But these tests are late indicators of AKI; what’s more, their results may be influenced by non-renal factors. For example, trauma, diet, and certain medications can affect BUN. (See Factors that may increase BUN and creatine.
Also, BUN doesn’t rise until many hours or days after AKI has occurred. Although urine output decreases if the glomerular filtration rate drops and before creatinine rises, decreased urine output may not specifically point to AKI.
As for serum creatinine—the current standard indicator of kidney function—it’s widely known to be insensitive to acute changes in kidney function. Although it’s an adequate marker of the glomerular filtration rate (GFR), it doesn’t reveal the degree of tubular injury. Nor does it correlate with the patient’s hospital survival or length of stay, whether measured at admission or the start of dialysis.
We know now that a change in renal function predicts short- and long-term outcomes. Preoperative creatinine levels have been shown to predict length of stays in the intensive care unit and mechanical ventilation time. Some studies show that in certain patients, such as those who’ve had cardiopulmonary bypass surgery, sepsis, or major surgery, AKI has a considerable effect on outcomes.
Like BUN, creatinine may not rise until hours or days after kidney injury; it doesn’t reveal AKI until about 50% of the renal tubules have been injured. So although it’s a good test for determining if renal function has deteriorated significantly, it doesn’t indicate current kidney injury. An ideal biomarker should predict AKI occurrence, duration, and severity.
Newly available biomarkers
Several new biomarkers studied in the past few years have been shown to detect AKI more accurately and quickly than BUN and creatinine levels. Many kidney biomarkers exist, including:
- neutrophil gelatinase-associated lipocalin (NGAL)
- kidney injury molecule-1 (KIM-1)
- cystatin C.
Some biomarkers are approved for use only in Europe. However, in 2015, additional biomarkers—specifically, tissue metalloproteinase-2 (TIMP-2) and insulin-like growth factor binding protein 7 (IGFBP7)—were approved in the United States for predicting or detecting AKI. Both appear in the urine within 12 hours if kidney injury is present. In validation studies, TIMP-2 and IGFBP7 proved significantly better at detecting AKI than all previously studied biomarkers. When detected at levels above 0.3 mcg/mL2 x 1,000, these biomarkers indicate cell-cycle arrest. Earlier detection of tubular injury and cell-cycle arrest allows clinicians to diagnose kidney injury promptly and reevaluate treatment goals.
Because Mrs. Clark is at risk for AKI based on her age, ideally she should be screened for TIMP-2 and IGFBP7 shortly after surgery to help predict if she might develop AKI, or to detect if this condition is present. Instead, her healthcare team gains a false sense of assurance from her normal BUN and creatinine levels. As a result, they don’t change her treatment, which includes not only the nephrotoxic drug vancomycin but also piperacillin/tazobactam. Vancomycin alone can cause harm in patients with AKI; the combination of this drug with piperacillin/tazobactam increases nephrotoxicity risk. Mrs. Clark’s physicians aren’t yet aware she has AKI, so her drug therapy continues as if she has normal kidney function. If her AKI worsens, she may end up needing lifelong dialysis—if she survives.
Changing treatment goals based on biomarkers
NGAL, KIM-1, TIMP-2, and ILGFBP7 levels give early warning of kidney injury. Unfortunately, few clinicians are aware of these new options for detecting AKI, instead using BUN and creatinine levels, which show renal function only after injury has occurred.
AKI is a serious and potentially fatal complication for many hospital patients. Using biomarkers for early detection could change treatment strategies and improve outcomes.
Susan M. Dirkes is president of Nursing Resource Consultants, LLC, in Newport, Michigan.
Selected references
Bihorac A. Guiding AKI prevention using biomarkers. April 2, 2015.
Chawla LS, Amdur RL, Shaw AD, et al. Association between AKI and long-term renal and cardiovascular outcomes in United States veterans. Clin J Am Soc Nephrol. 2014;9(3):448-56.
Devarajan P. Biomarkers for the early detection of acute kidney injury. Curr Opin Pediatr. 2011;23(2):194-200.
Edelstein CL. Biomarkers of acute kidney injury. Adv Chronic Kidney Dis. 2008;15(3):222-34.
Haase M, Bellomo R, Devarajan P, et al. Novel biomarkers early predict the severity of acute kidney injury after cardiac surgery in adults. Ann Thorac Surg. 2009;88(1):124-30.
Kellum, JA , Chawla LS. Cell-cycle arrest and acute kidney injury: the light and the dark sides. Nephrol Dial Transplant. 2016;31(1):16-22.
Macedo E, Mehta RL. Measuring renal function in critically ill patients: tools and strategies for assessing glomerular filtration rate. Curr Opin Crit Care. 2013;19(6):560-6.
Meersch M, Schmidt C, Van Aken H, et al. Urinary TIMP-2 and IGFBP7 as early biomarkers of acute kidney injury and renal recovery following cardiac surgery. PLoS One. 2014;9(3):e93460.
Ronco C. Biomarkers for acute kidney injury: is NGAL ready for clinical use? Crit Care. 2014; 18(6):680.
Ruiz-Criado J, Ramos-Barron MA, Fernandez-Fresnedo G, et al. Long-term mortality among hospitalized non-ICU patients with acute kidney injury referred to nephrology. Nephron. 2015;131(1):23-33.
Sileanu, FE, Murugan R, Lucko N, et al. AKI in low-risk versus high-risk patients in intensive care. Clin J Am Soc Nephrol. 2015;10(2):187-96.
Singbartl K, Kellum JA. AKI in the ICU: definition, epidemiology, risk stratification, and outcomes. Kidney Int. 2012;81(9):819-25.
Wetz AJ, Richardt EM, Wand S, et al. Quantification of urinary TIMP-2 and IGFBP-7: an adequate diagnostic test to predict acute kidney injury after cardiac surgery? Crit Care. 2015;19:3.
















{kind=link}
{kind=link}