This simple guide can facilitate interactions.
Takeaways:
- Be open minded when having a difficult conversation.
- Practice self-reflection to prepare for difficult conversations.
- Seek to understand and collaborate; keep the big picture in mind.
- Show grace and understanding.
An integral part of being a nurse is engaging in difficult conversations. Important nurses in history—Dorothea Dix, Clara Barton, Mary Eliza Mahoney, Florence Nightingale, Mabel Keaton Staupers, and others —had many difficult conversations in their efforts to advance nursing practice and improve health conditions for patients. Starting in nursing school, nurses are instructed to advocate for their patients and speak up when something isn’t right. Most nurses have opportunities for difficult conversations every day in the workplace. Unfortunately, many weren’t given the tools to have those conversations with colleagues. This article aims to give nurses a toolbox of discussion prompts and responses to help navigate difficult conversations with a win–win end in mind.
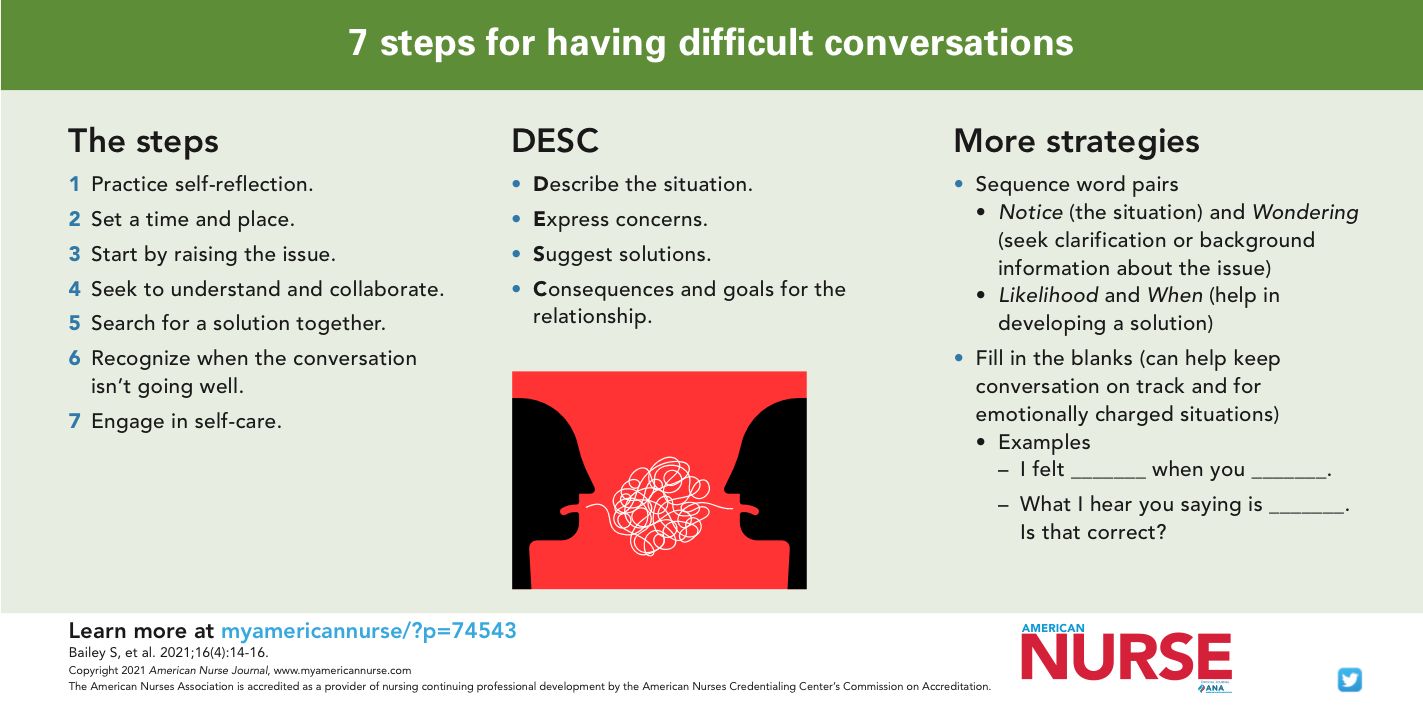
What is a difficult conversation? It’s one that evokes emotional responses to the words used or toward the other person. Just thinking about having the conversation can make the participants fearful, anxious, and angry, leading them to avoid initiating it. The conversation may feel like a burdensome chore instead of an exchange of ideas. Fortunately, seven simple steps can help you prepare for and initiate a difficult conversation.
Step 1 Self-reflection
The first step in preparing for the conversation is to take an honest look at yourself. Spend a few minutes reviewing your personal values, behaviors, and thoughts about the situation. Self-reflection is important to set the appropriate frame of mind for the conversation. Look for any bias or personal agenda, and consider possible trigger points that might cause an emotional reaction. Remember, the conversation should focus on the situation at hand and not personal emotions.
Next, take a moment to establish the tone of the conversation by setting an intention to do good for the other person. To keep the conversation on track, develop goals or outcomes and write them down. These goals can help engage the other person in a collaborative effort to reach them. Ultimately, you want to solve a problem, so you need to stay focused to help move the conversation toward a solution. Before beginning the conversation, commit to being empathetic, listening with an open mind, and considering the other person’s point of view
Step 2 Set a time and place
Schedule a time and place to have the difficult conversation in a private location. Avoid using phrases like “we need to talk,” which can make people defensive and apprehensive. Instead, tell the person what the conversation will be about. Be direct and to the point by saying: “I need to talk to you about what happened at the meeting yesterday. When would be a good time to meet?”
Step 3 Start by raising the issue
When you meet, get to the point and limit small talk, which might get you off track. The meeting is about the situation or issue not to catch up on what happened over the weekend. Greet the person and set the stage for the discussion by explaining the issue. Turn off cellphones to avoid distraction and so you can give your full attention to the conversation. Then focus on resolving the issue.
Experts say the hardest part of a difficult conversation is knowing how to begin. Use one of the following conversation patterns as a guide.
DESC script
The conflict resolution DESC (Describe the situation, Express concerns, Suggest solutions, Consequences and goals for the relationship) script, developed by Bower and Bower and one of the TeamSTEPPS® teamwork tools, can be used to describe the situation or event that prompted the need for the difficult conversation.
Example: Sally, I noticed that you haven’t attended any of the TeamSTEPPS training seminars this week (D). I feel frustrated because I believe this training will help improve the workplace environment for everyone (E). Could we talk a moment about what might be keeping you from attending the training sessions (S)? I hope we can work together on this to facilitate your attendance next week (C).
Sequence word pairs
Joy Baldridge developed word pairs—notice and wondering, likelihood and when—that can be used in sequence to start a difficult conversation. They can be used to start conversations about issues such as someone not carrying their share of the workload. Notice is the situation. Wondering seeks clarification or background information about the issue. Likelihood and when further the conversation by focusing on a solution.
Example: “Jill, I noticed the questions from your lecture aren’t loaded into the test for tomorrow and I’m wondering if something is wrong or if I can help.” After Jill answers, the speaker finishes the conversation by asking: “What’s the likelihood you’ll be able to meet the deadline for inputting the test questions, and when might that be?”
Fill in the blank
For new nurses or those who are having their first difficult conversation, a set of conversation starters designed as fill-in-the-blank sentences offer a little more structure and guidance. These sentences may be most helpful for conversations that are emotionally charged. They also can be used to keep the conversation on track and focus on delivering the message.
Examples:
- I felt________ when you ________.
- What I hear you saying is ___________. Is that correct?
- When you said_____________, I felt hurt and became defensive. I don’t think I was open to what you were saying. I’ll try to be more open-minded.
Step 4 Seek to understand and collaborate
Be open to different ideas and personal perspectives, focus on having a collaborative mindset while listening to the other person, and be empathetic. Rather than formulating a response while they’re talking, really listen. If necessary, take notes, but allow the other person time to tell their story. Avoid blame and accusatory language when telling your story or responding. Focus on the facts. Also, be mindful of body language to ensure it matches what’s being said. Body language that doesn’t match what the speaker is saying creates confusion. For example, telling someone you understand and are willing to be open-minded while your legs are crossed and you’re frowning sends two different and confusing messages.
Step 5 Search for a solution together
Brainstorm for multiple solutions to the situation. When an agreement (or an agreement to disagree) is reached, debrief to clarify what was said and to ensure both parties leave the conversation with a common understanding. Debriefing also should include the next steps you’ve agreed to take to resolve the issue. For example: “I’m glad we had this meeting today. I’ll work on giving positive feedback during evaluations and keeping an open mind about new staffing methods. I understand you’ll work on being receptive to changes in the workflow and provide feedback about how the changes are being implemented.” (See Wrapping it up.)
Wrapping it up
As appropriate, consider using one of these two sentences to end a difficult conversation.
- Use this sentence for a conversation that’s progressed to an agreement to respectfully disagree:
- “I think we have a solid understanding of where we differ. How can we move forward and work through this issue together?”
- Use this sentence for a conversation that’s gone well:
- “I have a better understanding of how the situation was misunderstood. Thank you for taking the time to talk with me about it.”
Step 6 Recognize when the conversation isn’t going well
Sometimes conversations get off track and derail completely. When that happens, stop the conversation and schedule a time to revisit the situation. If the conversation becomes emotionally charged, openly hostile, or doesn’t seem to have a solution in sight, end it by saying: “I’m not comfortable with the direction the conversation is going. I think it would be hard to have a productive conversation when we’re both upset. Can we revisit this topic later?”
Plan to reschedule the conversation after some time has passed to allow everyone to calm down and reflect. If you’re concerned that the follow-up conversation also may become emotionally charged, ask a mediator to attend to help keep the conversation on topic. The mediator is responsible for helping the participants focus on possible solutions, not emotions.
Step 7 Engage in self-care
Having a difficult conversation can be mentally and physically exhausting. Recognize the effect strong emotions can have on the body and mind and take self-care steps. Take a minute to walk outside and practice deep breathing. Have a cup of coffee with a friend. Take a moment to sit, close your eyes, and clear your mind. Remember the bigger picture of why the difficult conversation needed to happen and applaud yourself for being courageous enough to engage.
Avoidance isn’t an option
Difficult conversations aren’t easy, but they’re necessary so you and your colleagues can safely and effectively care for patients. Difficult conversations provide opportunities for feedback that will improve communication, overall patient care, and the work environment. Avoiding difficult conversations isn’t an option.
Sandy Bailey is the coordinator of online programs at the Kitty DeGree School of Nursing, University of Louisiana Monroe.
References
Agency for Healthcare Research and Quality. About TeamSTEPPS. June 2019. ahrq.gov/teamstepps/about-teamstepps/index.html
Baldridge J. Difficult Conversations Made Easy
. TEDx. March 2018. ted.com/talks/joy_baldridge_difficult_conversations_made_easy
Baldridge J. The Joy in Business: Innovative Ideas to Find Positivity (and Profit) in Your Daily Work Life. Hoboken, NJ: Wiley; 2019.
Bower SA, Bower GH. Asserting Yourself: A Practical Guide for Positive Change. Lebanon, IN: Da Capo Lifelong Books; 2004.
Burchard B. (2016, February 12). How to Have Difficult Conversations
. February 12, 2016. youtube.com/watch?v=9-xmbBSeu-s
Clancy C. (2014). Critical Conversations in Healthcare: Scripts & Techniques for Effective Interprofessional & Patient Communication. 2nd ed. Indianapolis, IN: Sigma; 2018.
Clark C. Conversations to inspire and promote a more civil workplace. Am Nurse Today. 2015;10(11):18-23.
Clark C. Creating & Sustaining Civility in Nursing Education. 2nd ed. Indianapolis, IN: Sigma; 2017.
Farrell M. Difficult conversations. J Libr Adm. 2015;55(4):302-11. doi:10.1080/01930826.2015.1038931
Grant AM. Conversational mapping: Coaching others (and ourselves) to better have difficult conversations. Coaching Psychologist. 2017;13(1):34-40.
Ignat C. Conflict management strategies in mediation. Law Rev: Jud Doctrine Case-Law. 2019;10(2):185-91.
Kay B. Tough talks: How to find success with difficult conversations and move forward productively. J Financial Plan. 2019;32(3):24-6.
Luff D, Martin EB Jr, Mills K, Mazzola NM, Bell SK, Meyer EC. Clinicians’ strategies for managing their emotions during difficult healthcare conversations. Patient Educ Couns. 2016;99(9):1461-6. doi:10.1016/j.pec.2016.06.017
Porath C. An antidote to incivility. Harv Bus Rev. April 2016. hbr.org/2016/04/an-antidote-to-incivility
Robbins M. Mel Robbins: How to have difficult conversations
. October 19, 2018. youtube.com/watch?v=TQ48GVMfvMg&list=WL&index=24&t=5s
Stowe M. Empathy: The heart of difficult conversations
. TEDx. November 2017. youtube.com/watch?v=2UvDMQyBVLs&list=WL&index=21&t=14s
Versical C. How to have difficult conversations with people you love. Bergen Counseling Center. November 27, 2017. bergencounselingcenter.com/articles/difficult_conversations_with_family